



Background
Three years after the emergence of SARS-CoV-2, more than 670 million cases of COVID-19 and 6.7 million COVID-19-related deaths have been reported. 1 Within a year, several SARS-CoV-2 vaccines with different formulations were developed, tested, and found to be efficacious (Pfizer’s BNT162b2, Moderna’s mRNA-1273, and Johnson & Johnson’s Ad26.COV2.S), and made available to adults.
SARS-CoV-2 evades the human immune response by altering protein translation, which reduces the production of interferons and interferon-stimulated gene products. Reference Siu, Chan, Kok, Woo and Jin2,Reference Hsu, Laurent-Rolle, Pawlak, Wilen and Cresswell3 Stimulation of host interferon defenses halts disease progression and shortens hospital stays in infected patients. Reference Nakhlband, Fakhari and Azizi4 Currently, the Centers for Disease Control and Prevention (CDC) and the Advisory Committee on Immunization Practice’s “General Recommendations on Immunization” caution against vaccination during moderate to severe acute illness, Reference Services5 citing that vaccination during this period could cause “diagnostic confusion between manifestations of the underlying illness and effects of vaccination or superimposing adverse effects of the vaccine on the underlying illness.” Reference Brady, Byington and Davies6 However, data supporting the rationale that acute illness may alter outcomes are limited. In the setting of most vaccine-preventable infections (including influenza), vaccines rarely cause high fever. 7,8 The COVID-19 vaccine is a notable exception, as these vaccines targeted toward SARS-CoV-2 stimulate side effects similar to an acute phase reactant. 9,10 While fever from a vaccine might affect whether to return to work or other clinical decision-making, there have not been studies formally evaluating the safety of vaccination in the period immediately surrounding COVID-19 illness.
Therapeutic vaccination is a strategy that relies upon the immune response induced by immunization to alter the disease course in a sick patient. Therapeutic vaccination is an active area of investigation in Hepatitis B Reference Brady, Byington and Davies6 and HIV 7 research, with therapeutic vaccines shown to be safe in chronically infected individuals. 8,9 Case reports documenting curative therapeutic vaccination for arteritis caused by P. insidiosum exist, 10 and postexposure prophylaxis with inactivated rabies vaccine has eliminated cases in the US among those treated. Reference Ugolini and Hemachudha11,Reference Ahmad, Moor-Smith and Hasselback12 However, CDC guidelines advocate against vaccination during COVID-19 illness despite the absence of prior studies assessing the effect of vaccination in the immediate peri-diagnostic period on clinical outcomes.
Earlier treatment with exogenous interferon-beta, which accelerates immune response, correlates with shorter duration of illness and lower ICU admission rates in hospitalized COVID-19 patients. Reference Rahmani, Davoudi-Monfared and Nourian13,Reference Alavi Darazam, Shokouhi and Pourhoseingholi14 Accordingly, we raised the question of whether vaccination during acute COVID-19 infection might improve clinical outcomes by stimulating alternative pathways for the immune system to fight infection as demonstrated previously for other diseases that evade immunity. Reference Thitithanyanont, Mendoza and Chuansumrit15
Exploring the association between peri-diagnostic vaccination and clinical outcomes is challenging because clinicians rarely ignore CDC guidelines recommending against the practice. Accordingly, single-site studies would not provide an adequate sample size to explore this question. A large, national database, however, might provide sufficient samples of this rare event to facilitate exploration. This retrospective observational study harnessing a large, national database of patients diagnosed with COVID-19 across the United States serves as a first line of inquiry into this important research question.
Methods
Objective
This study evaluated the effect of COVID-19 vaccination immediately prior to or following diagnosis of COVID-19 (either by PCR or positive antigen test).
Study design
We conducted an observational retrospective cohort study using a national repository of electronic health record (EHR) data to explore the relationship between peri-diagnostic vaccination and clinical outcomes in adult patients with COVID-19 infection. The overall population of interest consisted of previously unvaccinated patients over 18 who were diagnosed with COVID-19 via polymerase chain reaction (PCR) or antigen testing between December 11, 2020 (the date of vaccine emergency use approval in the United States) and December 19, 2021 (the last day for which we had 30-day follow-up data). Patients without documented vaccination up to seven days prior to infection were considered unvaccinated. To minimize the effects of immune memory from prior infection, we only included the first documented COVID-19 infection within the database for each patient included in our study.
From this population, the exposure group consisted of patients who received their first COVID-19 vaccination within 7 days before or after diagnosis. We examined vaccinations given during this period based on data that suggest the pooled incubation period for all COVID-19 variants is approximately 7 days. Reference Wu, Kang, Guo, Liu, Liu and Liang16 As date of symptom onset was not logged in the Optum database, choosing a cutoff of 7 days on either side of a positive test allows us to examine patients who were vaccinated earlier in their illness course while also confining vaccination to the period of acute infection. The control group consisted of patients who remained unvaccinated for 30 days following diagnosis. Included vaccines were Pfizer’s BnT162b2, Moderna’s mRNA-1273, and Johnson & Johnson’s Ad26.COV.S. The database reported vaccinations administered by contributing sites as well as patient-reported vaccinations; we included both in this study. Initial COVID-19 diagnosis for both groups was defined by the first instance of a positive PCR or antigen test. Patients were ineligible for the study if they had received at least one dose of any of the candidate vaccines more than 7 days prior to their initial positive COVID-19 test.
The primary outcome was clinical progression of COVID-19 disease during days 8–30 following diagnosis. We conducted two analyses: one for patients not hospitalized at diagnosis and another for patients hospitalized at diagnosis due to differing definitions of clinical progression. For nonhospitalized patients, progression was defined as admission to the inpatient or intensive care units. For hospitalized patients, progression was defined as admission to the intensive care unit. We excluded patients who were admitted to intensive care at the time of diagnosis. We did not include outcomes on days 0–7 because this would overlap with the period during which vaccination was permitted, meaning that some outcomes would be logged before our exposure (vaccination) occurred. Further, all human studies exploring COVID-19 vaccine effectiveness started on day 7 or 14 following the first dose of vaccine. Reference Sadarangani, Marchant and Kollmann17 Among nonhospitalized patients, outcomes observed were transition to hospitalization and/or intensive care. We identified hospitalizations based on patient classification as “observation,” “inpatient,” or, alternatively, “other patient type” with a procedure or medication specified by the WHO-Clinical Progression Scale. Reference Marshall, Murthy and Diaz18 Patients requiring endotracheal intubation, mechanical ventilation, tracheostomy placement, high flow nasal cannula, and noninvasive positive pressure ventilation without a documented intensive care unit (ICU) stay were included in the intensive care severity category. Because all data were deidentified, no institutional review board approval was required for this study.
Data source
We used Optum’s longitudinal EHR repository, which is derived from dozens of healthcare organizations in the United States and includes patients’ healthcare data from more than 700 hospitals and 7,000 clinics (Optum Inc., Eden Prairie, MN, USA). The data are certified as deidentified by an independent statistical expert following HIPAA statistical deidentification rules and managed according to Optum’s customer data use agreements. The COVID-19 data set incorporates a wide swath of raw clinical data, including new, unmapped COVID-specific clinical data from inpatient and ambulatory EHRs, practice management systems, and numerous other internal systems. Information is processed from across the continuum of care, including acute inpatient stays and outpatient visits. The COVID-19 data captures point-of-care diagnostics specific to the COVID-19 patient during initial presentation, acute illness, and convalescence with over 500 mapped labs and bedside observations, including COVID-19-specific testing. The Optum COVID-19 data elements include patient-level information like demographics, hospitalizations, Emergency Department (ED) visits, intensive care unit (ICU) admissions, mortality, medications, laboratory tests, procedures, and diagnoses. The data are comprised of multiple tables linked by a common patient identifier (an anonymous, randomized string of characters).
Statistical analysis
For patients hospitalized (but not receiving intensive care) between days 0 and 7 after diagnosis, we used binary logistic regression to evaluate progression to ICU-level care on days 8–30. For patients not hospitalized during days 0–7, we used proportional odds logistic regression to evaluate progression as an ordinal outcome including hospitalization and ICU level care on days 8–30. Ordinality was assessed in advance using the Wald test for parallel lines. Due to how deaths are registered in the Optum database (all deaths, regardless of actual date, are recorded as having occurred on the first of the month), deaths were not included in the analysis. Assuming a significant effect in the unadjusted models, we performed propensity score matching using the following covariates: age, sex, race, ethnicity, region, body mass index (BMI), insurance status, and past medical history using individual elements from the Charlson Comorbidity Index. Overall model performance was evaluated compared to the null model using likelihood ratio χ2 tests. Alpha was set to 0.05 for significance testing. Statistical analysis was performed using Stata version 17, Parallel Edition (StataCorp, College Station, TX, USA).
Results
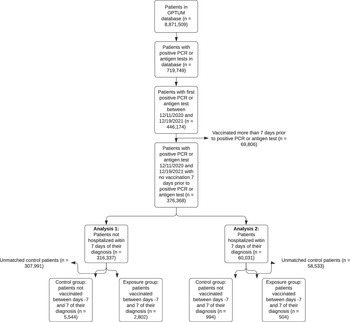
The Optum database contains information on 8,871,509 patients. These patients had a mean age of 47 [St. Dev. 22.9] years. Patients were largely female (56.1%), White (67.1%), and non-Hispanic (77.1%). Patients lived in the Midwest (41.6%), Northeast (21.6%), South (14.9%), and West (9.3%) (Supplementary Table S1). As of January 19, 2022 (the last date for which data were available), 2,056,878 patients had at least one dose of the three approved vaccines documented. A CONSORT diagram of patient selection during the study is depicted in Fig. 1.

Figure 1. CONSORT diagram illustrating how patients were selected from the OPTUM database for inclusion in the study.
Among hospitalized patients, those who received peri-diagnostic vaccinations were older (mean age 61.6 [17.6] vs 56.6 [19.2], P < .001), less often Hispanic (12.9% vs 16.9%, P = .044), more commonly located in the Northeast (23.4% vs 14.1%, P < .001), and more commonly insured by Medicare (32.8% vs 25.5%, P < .001) or commercial payors (43.5% vs 41.8%, P < .001) (Table 1). Among nonhospitalized patients, those receiving peri-diagnostic vaccinations were older (mean age 49.2 [17.0] vs 45.4 [17.2], P < .001), more often female (63.7% vs 55.8%, P < .001), White (71.4% vs 64.1%, P < .001), and more commonly insured by Medicare (12.5% vs 8.9%, P < .001) or commercial payors (64.4% vs 52.9%, P < .001) (Table 2). The prevalence of illnesses measured in the Charlson Comorbidity Index was higher among vaccinated patients in both groups (Tables 1 and 2).
Table 1. Characteristics of all patients hospitalized between day 0 and day 7 postinfection

Table 2. Characteristics of all patients not hospitalized between days 0 to 7 postinfection

Among hospitalized patients, there were 543 patients (0.9%) who were vaccinated between days −7 and 7 and 59,488 (99.1%) patients who were not vaccinated. Progression was observed in seven vaccinated patients (1.29%) and 497 unvaccinated patients (0.84%). The binary logistic regression (LR) model evaluating clinical progression as a function of vaccination had a nonsignificant LR χ2 test (P = .232). Among nonhospitalized patients, there were 2,844 (0.9%) of patients vaccinated between days −7 and 7, and 313,493 (99.1%) were not vaccinated. The data set had a Wald test of parallel lines assumption that was not significant (P = .987), which suggests that the proportional odds/parallel lines assumption was not violated, supporting the use of a proportional odds model (Table 3). The proportional odds logistic regression model evaluating clinical progression as a function of vaccination among nonhospitalized patients also had a nonsignificant LR χ2 test (P = .643) (Table 3).
Table 3. Rates of progression in hospitalized and nonhospitalized patients

* Indicates P-value reported for OR.
With no significant difference observed in unadjusted models, we then performed propensity score-matched analysis to explore whether cohorts comparable in demographic and comorbid factors experienced any clinical difference following vaccination. In hospitalized and nonhospitalized patients, propensity score matching yielded cohorts that were statistically indistinguishable regarding demographic data and rates of comorbidities (Supplementary Tables S2 and S3). Among hospitalized patients, clinical progression was more common in those who were vaccinated than those who were not (Table 3; 1.39% vs 0.30%). Relative to vaccinated patients, unvaccinated patients had an OR of progression of 0.21 (95% CI 0.05–0.83) (Table 3). Among nonhospitalized patients, clinical progression did not differ between those who were and were not vaccinated peri-diagnostically (Table 3).
Discussion
In this observational study, we evaluated whether peri-diagnostic vaccination was associated with worse clinical outcomes among adult patients with COVID-19. Patients who received peri-diagnostic vaccinations were more often White, older, more commonly located in the Northeast, more commonly insured by Medicare or commercial firms, and more burdened by comorbidities. As Optum only logs month, not date of death, this outcome was not assessed in our analysis. Our partial proportional odds model showed that vaccination between days −7 and 7 of a positive test was not associated with clinical progression in patients, regardless of whether they were hospitalized at the outset. However, analysis of propensity-score matched vaccinated and not vaccinated groups showed that vaccination was associated with clinical progression to a higher level of care during days 8–30 postinfection in hospitalized patients. This result contradicts our hypothesis that peri-diagnostic vaccination would decrease rates of clinical progression. It is important to note the number of patients included in our PSM analysis who progressed from hospitalization to ICU care was very limited in vaccinated and not vaccinated groups (7 and 3, respectively), making interpretation of this result difficult. Vaccination was not associated with clinical progression to a higher level of care in ambulatory patients.
Multiple theories could explain the limited association between peri-diagnostic vaccinations on clinical progression. Acute-phase SARS-CoV-2 infection causes lymphopenia, Reference Chen, Wu and Guo19 which could impair the immune response to vaccination. SARS-CoV-2 vaccines largely work by stimulating plasma cell production of broadly neutralizing antibodies, which are not produced in large quantities before most acute infections resolve. Reference Mascellino and Oliva20 Though exposure to spike protein from vaccination induces innate immune responses (as evidenced by vaccine-induced fever), our results suggest that these responses are not sufficient in the context of acute illness to meaningfully alter outcomes. Study in humans shows that, though levels of bloodstream inflammatory monocytes and expression of genes encoding interferons increase 1–2 days following an initial immunization against SARS-CoV-2, the induction of innate immune responses with the second vaccine dose is several-fold greater. Reference Arunachalam, Scott and Hagan21
As COVID-19 moves from pandemic to endemic, host-directed therapies are needed to protect from severe illness caused by new viral variants. Our results suggest that the innate immune stimulation from first-dose vaccination is likely not sufficient to meaningfully alter clinical outcomes. Approached differently, the fact that vaccines do not meaningfully alter clinical course can be leveraged to promote vaccine uptake among unvaccinated (or undervaccinated) patients when hospitalized with COVID-19 illness. Nearly 3 years into the pandemic, 22% of American adults remain unwilling to obtain COVID-19 vaccines. 22 Nonetheless, more research is needed to elucidate specific mechanisms of innate immunity that allow patients to promptly recover from COVID-19. Peri-diagnostic vaccination, aided by adjuvants, could have a role in fighting SARS-CoV-2 and other viral illnesses in the future, but our results suggest that, given the natural history of COVID-19 and the time taken for vaccines to stimulate adaptive immunity, currently available vaccines are unlikely to meaningfully affect outcomes when administered immediately after diagnosis.
Limitations
Our study, like any study using a large national EHR data repository, suffers from limitations. Evaluated 2 weeks following the initial dose, the three vaccines employed in our study (mRNA-1273, BNT162b2, and Ad26.COV2.S) induce CD8 T cell responses at similar rates, but mRNA-1273 and BNT162b2 stimulate higher titers of neutralizing antibodies than Ad26.COV2.S. Reference Zhang, Mateus and Coelho23 Further study stratifying results based on vaccine type might identify differences in efficacy between vaccines in the peri-diagnostic period; unfortunately, our data collection did not allow us to distinguish between vaccine types. Among vaccinated individuals, the difference in the interval between diagnosis and vaccination might affect outcomes, and future analyses should further interrogate this question. Interpretation of our results is limited by the diversity of individuals in our cohort, particularly the low representation of Hispanic/Latino patients (Table S1). The median ages of patients included in our analysis of nonhospitalized and hospitalized patients were approximately 49 and 61, limiting the applicability of our results to older patients, who are the most vulnerable to SARS-CoV-2 infection. Reference Crimmins24 Differences in care, such as variability among hospitals in the use of steroids and remdesivir during early infection, likely affected clinical outcomes in our hospitalized group. Since peri-diagnostic vaccination is against current guidelines, the exposure of interest was very rare among the population included in the database. This very small sample size is a significant limitation and a larger sample might show a different signal. Unfortunately, such a sample is unlikely to be identified given the rarity of peri-diagnostic vaccination. Viewed another way, the size of the Optum database is a strength since it allowed us to perform this study in the first place. We had a low rate of missing comorbidities, however, this number may have been falsely low, especially for patients with limited entries in the database. Despite the limitations that come with studying a rare, complex event in the context of a public health emergency, our study provides further evidence for the CDC’s recommendation against vaccination shortly following infection and generates intriguing questions regarding the ideal vaccination timeline.
Conclusions
In this retrospective observational cohort study, we did not observe an association between vaccination for COVID-19 during acute illness and severity outcomes in unmatched cohort analysis. When cohorts were matched for demographic and comorbid conditions, vaccination was associated with greater odds of clinical progression. Despite the large size of the Optum electronic health record data set, vaccination was rare in the acute phase, and our sample size was limited. Further studies using other national and international data sets are recommended to further evaluate this important clinical question.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ash.2023.417
Acknowledgements
As all data used were deidentified, the University of Texas Southwestern Human Research Protection Program Policies, Procedures, and Guidance did not require institutional board approval for this study.
Author contribution
Designed study: JAC, BT, TMP, MH, HL, PS, DS, AN, CUL, RJM, RWT, Performed analysis: JAC, BT, MID, MP, SNS, RWT, Wrote and revised manuscript: JAC, BT, CUL, RJM, RWT, Revised manuscript: TMP, JJH.
Financial support
This study was supported by internal funds.
R. J. M. has received grant funding from the Centers for Disease Control and Prevention and research funding from Verily Life Sciences, the Sergey Brin Family Foundation, and the Texas Health Resources Clinical Scholar program.
Competing interests
The authors declare no competing interests.
Patient consent statement
This study does not include factors necessitating patient consent.






 Open access
Open access