



Introduction
Motor neurone disease (MND), also known as amyotrophic lateral sclerosis, is an adult-onset neurodegenerative disorder leading to progressive muscle paralysis. Although MND is essentially a motor disorder, it has multisystem involvement including cognitive, sensory, and/or autonomic symptoms (Hardiman et al. Reference Hardiman, Corr and Logroscino2017; Talbot Reference Talbot2009) where 50%–75% of people living with MND will develop behavioral and cognitive symptoms and 15% frontotemporal dementia (Ringholz et al. Reference Ringholz, Appel and Bradshaw2005). With no known cure to date, the life expectancy is of 2–3 years (Shaw et al. Reference Shaw, Quinn, Daniel, Oliver, Borasio and Johnston2014). While there are different subtypes of MND, amyotrophic lateral sclerosis is the most common form of the disease (Hardiman et al. Reference Hardiman, Corr and Logroscino2017).
Most people living with MND are cared for at home by a family member (Pagnini Reference Pagnini2013; Peters et al. Reference Peters, Fitzpatrick and Doll2012). Due to the disabling nature of the disease, family carers have a demanding role during caregiving and transit a parallel journey from the person living with MND (Rabkin et al. Reference Rabkin, Albert and Rowland2009). Previous systematic reviews (Aoun et al. Reference Aoun, Bentley and Funk2013; Mockford et al. Reference Mockford, Jenkinson and Fitzpatrick2006) explored experiences of MND family carers revealing compromised physical and psychological health, diminished quality of life, strained relationships, and challenges in accessing MND information and service provision. Further qualitative research highlighted the many practical tasks carers had to take care of and learn (Aoun et al. Reference Aoun, Connors and Priddis2012), carers’ fears for the future, and feelings of anger and frustration (Oyebode et al. Reference Oyebode, Smith and Morrison2013; Whitehead et al. Reference Whitehead, O’Brien and Jack2012). Qualitative studies have also examined carers’ assistance with gastrostomy (Stavroulakis et al. Reference Stavroulakis, Baird and Baxter2016), carers’ involvement in decision making (Hogden et al. Reference Hogden, Greenfield and Nugus2013), non-invasive ventilation’s limited influence on carer burden (Baxter et al. Reference Baxter, Baird and Thompson2013) and the need for early palliative care (Flemming et al. Reference Flemming, Turner and Bolsher2020). Carer grief has also been explored (Aoun et al. Reference Aoun, Connors and Priddis2012; Oyebode et al. Reference Oyebode, Smith and Morrison2013; Whitehead et al. Reference Whitehead, O’Brien and Jack2012). In addition, a narrative review revealed factors contributing to carer emotional distress, such as the severity of MND symptoms, carers’ coping styles, relationship satisfaction, and social support (Gluyas et al. Reference Gluyas, Mathers and Hennessy Anderson2017). Emotional wellbeing refers to an individual’s positive feelings towards life, including their everyday experiences and reflections about life satisfaction and meaning, and the ability to accomplish goals in life (Park et al. Reference Park, Kubzansky and Chafouleas2022). In this paper, we will refer to emotional wellbeing to describe the emotional experiences of MND family carers, which contribute to their life satisfaction and quality of life.
A review of qualitative literature described diverse experiences impacting MND carers’ emotions, such as changes in their lifestyle compromising their personal and social time, and isolation arising from limited communication with healthcare professionals (HCPs), the person living with MND, family members, and friends and in their relationships’ dynamics (Holkham and Soundy Reference Holkham and Soundy2018). Similarly, a recent systematic review examining factors affecting MND informal carers’ grieving processes emphasized how factors, such as the uncertainty of the disease, being deprived of a social life, and changes in roles and communication affected carers’ emotions during the progression of MND and highlighted the need for emotional support (Trucco et al. Reference Trucco, Backhouse and Mioshi2023).
Few studies have examined carers’ coping strategies to manage their emotional challenges. A qualitative study reported that some coping strategies encompassed carers’ attitudes (e.g., having a positive approach, not planning ahead, or anticipating problems), problem-solving skills (e.g., negotiating solutions with the person with MND), managing time effectively, and socializing with others (Gent et al. Reference Gent, McGarry and Pinnington2009). Another qualitative study found that strategies used were the gradual acceptance of MND, engaging in meaningful activities, focusing on positive and present aspects of life, spending time without thinking about MND, and receiving support from HCPs, friends, and family (Pinto et al. Reference Pinto, Geraghty and Yardley2021).
The need to better support family carers of this population in the emotional, psychological, practical, informational, and social areas has been documented by review literature (Gluyas et al. Reference Gluyas, Mathers and Hennessy Anderson2017; Oh and Kim Reference Oh and Kim2017). Nevertheless, research focusing specifically on understanding which personal coping strategies family carers use to maintain their emotional wellbeing to be able to manage their own emotions remains sparse. Thus, the aim of this study is to explore the emotional experiences and coping strategies of family carers currently supporting people living with MND. By elucidating carers’ emotional journeys, we aim to identify relevant areas of focus for potential interventions to support and meet the needs of carers’ emotional wellbeing.
Methods
Design
This was an interpretive descriptive study (Thorne Reference Thorne2016; Thorne et al. Reference Thorne, Kirkham and MacDonald-Emes1997, Reference Thorne, Kirkham and O'Flynn-Magee2004) using semi-structured interviews and a reflexive thematic analysis (Braun and Clarke Reference Braun and Clarke2006, Reference Braun and Clarke2021a). We used an interpretive descriptive approach as it seeks to uncover and understand recurring themes and patterns within subjective human experience while accounting for participants’ and researchers’ subjectivity. Beyond the mere description of the phenomenon, it generates credible and relevant experiential knowledge applicable to care practice Thorne Reference Thorne2016).
Participants and recruitment
We recruited 14 current family carers from MND carers’ support groups via online or face-to-face presentations, MND clinics providing leaflets to family carers, and media releases with study information. Furthermore, participants taking part in an MND questionnaire study, part of a higher degree project, were asked to provide their details if interested in the present study. We contacted potential participants by email or telephone and provided a participant information sheet. To be included in the study, participants had to be at least 18 years old, have conversational English, have the capacity to consent for themselves and be a partner/spouse currently living with and supporting someone diagnosed with MND. Among 24 interested participants, two were ineligible, two did not join the interview due to unforeseen circumstances, four did not reply to the email sent, one was hospitalized, and one had scheduling constraints. The 14 participants (female = 10; male = 4) were all co-habiting spouses of a person living with MND and living in different regions of the United Kingdom. All participants signed an informed consent form and completed the interview. No participants were previously known by the researchers.
Data collection
Semi-structured interviews followed a topic guide with broad and open-ended questions specifically designed by APT and TB to examine and understand how carers’ experiences of caring affected their emotional wellbeing and how they coped with arising emotions. Questions were devised from the literature and refined after discussions with two carers of people with MND and one pilot interview. A.P.T. (an experienced occupational therapist working with neurological diseases in academic and clinical settings) conducted recruitment and data collection. We assessed sample size during the research process through constant information power appraisal of the data, which considers the study aim, sample specificity, use of theory, dialogue quality, and analysis strategy. Given our focused aim, specific participants, and the strong dialogue drawing on considerable experience of the researcher with MND carers, we reached information power after 14 interviews. At this point, no new codes and themes were being generated (Braun and Clarke Reference Braun and Clarke2021b; Malterud et al. Reference Malterud, Siersma and Guassora2016). To obtain rich and in-depth accounts of participants’ experiences, we used probes, such as “How did you cope with these feelings?” and “Can you tell me a bit more?.” By probing we aimed to generate deeper knowledge without guiding the participant to a specific response. Interviews were audio-recorded if conducted face-to-face (n = 6) at a location of the participant’s choosing and video-recorded if conducted online (n = 8). We conducted the interviews between August 2022 and February 2023, and they lasted on average 75:33 min.
We reassured participants they could withdraw from the study at any stage, not answer questions they did not feel comfortable with and take as many pauses as needed. At the end of the interview, participants were de-briefed, and encouraged to check a wellbeing contact list providing signposting to relevant services if upsetting emotions arose.
Data analysis
Interviews were professionally transcribed verbatim. Subsequently, all identifiable information was anonymized. We decided to not conduct member checking due to the sensitive nature of the study, time, and burden implications for carers, and the potential negative impact on participants, since distressing emotions could be triggered when reading their transcripts (Hallet Reference Hallet, Midgley, Danaher and Baguley2012). A.P.T. and T.B. (an experienced social scientist post-doctoral researcher with a social care background) analyzed data inductively with reflexive thematic analysis (Braun and Clarke Reference Braun and Clarke2006, Reference Braun and Clarke2021a), which accounts for researchers’ subjectivity and perspectives inflected by their position. We independently immersed ourselves in the data during data collection by repeatedly reading the transcripts and began to identify relevant patterns. We met regularly to discuss initial impressions and reflections on the data. We generated codes encompassing both surface (semantic) and underlying (latent) features, with regular discussions to examine analytical observations. Once data collection was complete, APT coded and collated all data. Transcripts were uploaded into NVivo12 Pro to assist in the management of the analysis process. By constantly comparing the codes, collated data, and our interpretations (Clarke and Braun Reference Clarke and Braun2020) and asking big questions of the data, such as “what is happening here” and “what are the dimensions of this?” (Thorne Reference Thorne2016; Thorne et al. Reference Thorne, Kirkham and MacDonald-Emes1997, Reference Thorne, Kirkham and O'Flynn-Magee2004), we proposed initial candidate themes ensuring a coherent pattern between them and participants’ experiences. E.M. (an experienced applied MND researcher and occupational therapist) joined to discuss codes, collated data, and potential themes, which were re-checked against coded data, refined and reviewed further to capture the overall story in the data. The final themes combined both semantic and latent meanings about carers’ emotional experiences to account for the reality of their emotions and coping strategies.
Results
Participants’ demographics are summarized in Table 1. The analysis produced three intersecting themes which reflect the emotional journey current family carers (FC) experienced while caring for a person living with MND.
The analysis examined how changes and losses due to MND impacted on carers’ emotions and the coping strategies they identified as useful to face the emotions arising. An overview of the themes is presented in Figure 1, and coping strategies most used are summarized in Table 2. The three themes were:
1. Destabilization of diagnosis;
2. Adapting to new circumstances and identifying coping strategies;
3. Maintaining emotional coping.
Table 1. Demographics of family carers currently supporting people living with MND and the people living with MND they support

MND = motor neurone disease.

Figure 1. Emotional journey of family carers currently supporting people living with MND.
Table 2. Overview of themes and coping strategies family carers of people living with MND use
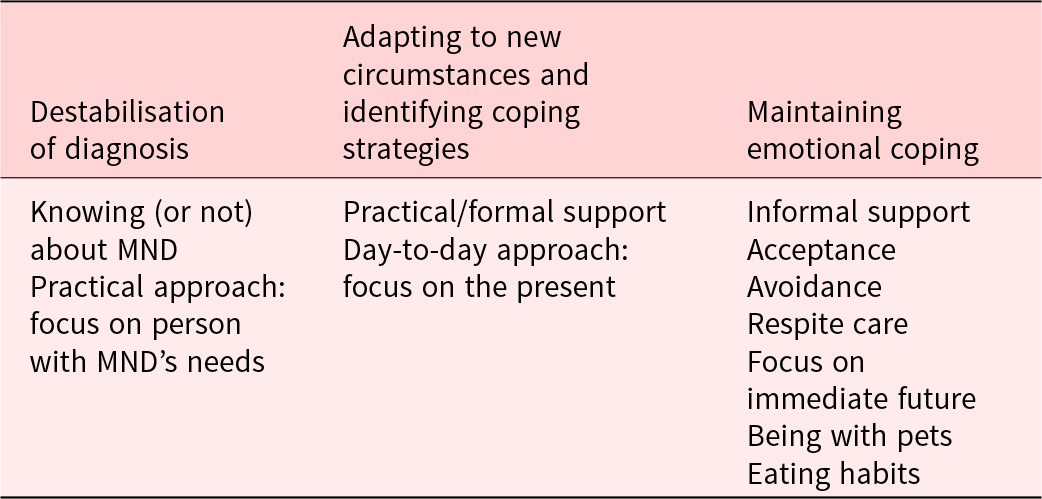
MND = motor neurone disease.
Destabilization of diagnosis
The emotional journey started when the first symptoms presented, but intensified greatly when the actual diagnosis of MND was conveyed. Diagnosis triggered distress and often left carers not knowing what to do, destabilizing their lives.
All participants described the impact of the diagnosis in terms of shock and devastation, characterized by feeling overwhelmed, anxious, and lost.
Just utter shock…disbelief…we’d obviously heard of it, but you just don’t think that you and your family are going to be affected…I was just pretty devastated… (FC3, female)
These emotions worsened when carers received unclear information about MND. Most participants discussed that when HCPs explained MND symptoms, progression, and prognosis, uncertainty-related emotions, stress, and anxiety reduced. MND nurses were mentioned by some participants to provide comfort. While some participants self-searched for more information (e.g., internet and books), others preferred not to investigate further. In both cases, knowing more, or not, impacted on carers’ emotions by reducing distress.
[Name] was given literature about MND and the different impacts…I don’t want to know. I will deal with now, there’s no point in reading what might happen. Because it might not…For everybody, it’s an individual journey. (FC1, female)
Participants’ communication of the diagnosis to others was influenced by the carers and the person living with MND’s feelings. While some carers shared the diagnosis immediately, others delayed as they were concerned about how family members would cope with it, particularly when living far away or experiencing personal stressful situations.
We hadn’t told our sons because one of them was in [country] and we wanted to tell them face-to-face…we needed to come to terms with it first…we needed to accept it before…there was also this concern about how much it would affect them mentally and emotionally… (FC12, female)
Carers actively worked to cope with and transit the initial shock by adopting personal strategies to gradually temper the early overwhelming emotions. Knowing more about MND, or not, and taking a practical approach by focusing on what the person with MND needed to have comfort were the most common strategies used during this first period.
…the initial diagnosis was difficult for both because you were entering a world of unknown, neither of us knew anything about MND…And I remember us both sitting down and thinking, well crying, and…what could I say to [name] to help him? (FC5, female)
Family carers described this first period as causing great destabilization in their emotions and in their everyday activities and had difficulties embracing this new reality.
Adapting to new circumstances and identifying coping strategies
Following the impact of diagnosis, carers started experiencing everyday changes and losses due to MND and gradually adapted to these by identifying strategies to better face their circumstances.
All participants described changes in their relationship with the person with MND, mainly caused by a shift from being a spouse to a caring role and due to MND symptoms (e.g., communication and physical symptoms).
Carers also expressed sharing limited family time causing feelings of sadness, particularly when lacking time with children and grandchildren.
One thing that I really do miss…I have a daughter in [city] with three grandchildren. I used to go over once every six weeks…wouldn’t leave [name] now, so I miss that. (FC9, female)
Participants described how losing freedom to perform and engage in personal activities led to frustration, anger, and distress. Self-care time diminished and three carers reported reducing work for caregiving. Most carers also felt deprived of a social life and expressed sadness for the lack of spontaneity to make plans, particularly if these involved holidays.
And it doesn’t matter what plans you have made-up until that point…if the plan was today, yesterday…we had plans that were going forward for months or years…that is completely gone out…Your whole life becomes very much more short term. (FC2, male)
During this period, learning how to do things previously accomplished by the person with MND added to carers’ emotional distress. Participants explained how they started performing new household chores, such as fixing things and cleaning, and how this contributed to feelings of anxiety and tiredness.
I was doing everything…learning DIY [Do It Yourself] and how to use saws and screwdrivers and just lots of different things…probably [name] watching me and, you know, I say things and it’s tough. (FC3, female)
Feelings of resignation for not being able to change, fix, or control the present situation arose across all participants.
I suppose the overall feeling is frustration…Frustration that I can’t fix her; frustration that I can’t make her better; frustration, how did it happen…there is nothing you can do to fix it… (FC8, male)
Receiving practical support from HCPs and MND organizations, such as obtaining equipment and having HCPs’ appointments reassured carers that the person with MND was well supported. The lack or disorganization of this support made carers feel anxious, upset, and disappointed.
…I found it totally overwhelming, there were all these different people who were presenting themselves…two people came around, and I thought they were occupational therapists, but they were from Social Services, and we never did understand why they came to see us… (FC6, female)
During this period, carers gradually began to accept that their lives had changed. Carers actively found ways for not giving up and continued coping with their emotional journey, represented by sadness, tiredness, anger, frustration, and loneliness, which worsened during the nights as negative thoughts about their reality crept in. Focusing on the present and taking one day at a time were professed as the most useful strategies to help carers emotionally transit this post-diagnosis period.
Maintaining emotional coping
With time, participants identified their own emotional coping strategies. While several emotions still arose, carers were now capable of adapting and accepting continuous changes and losses, while maintaining their emotional coping and not destabilizing.
At this stage, informal support, such as spending time with family and friends, allowed carers to not think about MND, easing negative emotions. Attending MND carers’ support groups was helpful for some carers as they felt understood by others facing a similar reality. However, other carers avoided them so as not to encounter MND progression.
One carer had formal carers who came to sit and stay with the care recipient and some carers reported having access to respite care was useful and described it as recharging energy for their continuous caring role.
…my family and my friends are good support…when [name] goes for respite, that’s a great support to give me a break…helps me deal with things a little bit better… (FC14, female)
How the person living with MND faced their own challenges, changes, and losses had an important impact on carers’ emotions. When they were positive about the present situation and future, carers felt stronger and happier. When they felt sad, withdrew from social activities, and experienced negative emotions, carers felt distressed. Under these circumstances, carers tried to support the person with MND by remaining positive but consequently confronted tiredness and burden.
…so I just felt I needed to support him…I had to carry it for him sort of thing. Be strong for him. (FC9, female)
Carers’ allowance (government payment received for caring) made carers feel their role was being recognized. However, carers were disappointed about the amount of allowance and the difficulties accessing it.
Planning for end-of-life care with the person with MND and having a power of attorney in place made carers experience a sense of relief.
And pre-planning…legal things like with power of attorney and things like that…we got all that sorted and out of the way, so that, at the time we were doing it all, it was very hard but I’m glad that’s all sorted. (FC4, female)
Conversely, some carers preferred not to look into future planning as it influenced their emotions negatively.
Looking forward to doing things in the immediate future, such as meeting family or friends, or going on holidays were useful strategies most carers identified for coping with their emotions. Some carers also found emotional comfort by changing their eating habits, such as eating chocolate. Pets were also considered a source of emotional support, particularly dogs, with their presence reducing carer stress and anxiety. Furthermore, one carer reported that having a sense of achievement by completing small tasks, such as tidying the bed, made them cope better as these were things they could control.
Most carers described that not thinking about what the future could bring and how they would manage with potential changes, was the strategy that best worked for them for managing their emotions.
…it’s a day at a time. Try and take a day at a time…just deal with each situation as it arises and try not to worry about what might be and try and live with and not die from. (FC4, female)
At this time of their emotional journey, while carers still experienced negative emotions with new changes and losses, knowing the strategies that worked for them to maintain their emotional coping made distressing emotions ease quicker.
Discussion
This study presented the emotional journey MND family carers experienced while caring for the person living with MND and the strategies they used to maintain their emotional coping when facing continuous losses and changes throughout the progression of MND. Three themes were identified. The first theme revealed the state of shock and devastation carers experienced when receiving the diagnosis and how learning and knowing about MND helped them transit this overwhelming period. The second theme described how carers experienced and gradually adapted to losses and changes happening by identifying coping strategies to manage emotions. The third theme recognized the different coping strategies used by carers, which enabled them to accept and adjust to the constant challenges of losses and changes while maintaining coping.
These findings align with a previous thematic review which identified changes and losses in relationships, future plans, daily activities, and feelings of isolation (Holkham and Soundy Reference Holkham and Soundy2018). Previous research also identified similar coping strategies, such as focusing on the present moment, receiving support, and not thinking about MND (Pinto et al. Reference Pinto, Geraghty and Yardley2021). Furthermore, studies have highlighted the importance that support from family, social networks, and formal care have on carers’ emotional wellbeing (Aoun et al. Reference Aoun, Cafarella and Hogden2021; Trucco et al. Reference Trucco, Backhouse and Mioshi2023). Similarly, this study revealed how being close to family, informal support, linking with networks (e.g., MND associations) and connections with HCPs influenced carers’ emotions and caring experiences positively. This study provides an in-depth understanding of carers’ emotional journeys and how they adapt and adjust to new circumstances. Our findings show that when conveying the diagnosis, guidance on caring and support options should be provided. Early practical support, particularly from HCPs and MND organizations should be offered as carers’ emotions ease when feeling well supported. As disease progresses, addressing isolation, such as pursuing family meetings, targeting acceptance, and day-to-day approaches, could be beneficial. Further attention should be given to coping mechanisms such as avoidance, i.e., not thinking about MND, withdrawing from social activities. In some cases, this avoidant style of coping might have negative effects on advance and end of life care planning, lack of preparedness for progression, as well as on emotional wellbeing and grieving processes after the care recipient’s death (Papastavrou et al. Reference Papastavrou, Charalambous and Tsangari2012; Trucco et al. Reference Trucco, Backhouse and Mioshi2023).
These findings have important implications for professional and support services which highlight the need to provide MND information and offer respite care. Surprisingly, no participants mentioned hospice or generic day services for the person living with MND, and only one participant had formal carers who came to sit and stay with the care recipient. Perhaps these services were not available, the person with MND was not accessing them, or if they did, it did not impact on carers’ wellbeing. However, this type of support could potentially relieve carers from caring responsibilities and should be considered. In addition, psychological interventions, such as Acceptance and Commitment Therapy, could help carers continue engaging in meaningful activities, while focusing on the present moment and embracing emotional challenges associated with their present situation (Han et al. Reference Han, Yuen and Jenkins2021). Interventions targeting resilience should also be contemplated, as they target the negative impact of situations by seeking adaptation by reducing emotional distress caused by the emotional and physical demands of caregiving (Palacio et al. Reference Palacio, Krikorian and Gómez-Romero2020).
This study has limitations that should be considered. We acknowledge that individual caring experiences could have been influenced by economic possibilities to access support and the variation of support received in each UK region (e.g., carers’ allowance, availability of MND care coordinators, and community neurology nurses), which were beyond the scope of this study and may have affected the findings. Moreover, although the sample size was large enough to provide sufficient information power, we did not collect data from family members other than spouses or on carers’ ethnicity which might have captured different emotional experiences. This was a one-time interview study and we did not recruit according to time of caring and symptoms of MND. Consequently, this might have impacted on the findings, since not all participants were transiting through the same period of the disease. Additionally, since participation was completely voluntary, it is likely that carers who took part were emotionally coping with MND.
We recommend that future studies explore the emotional experiences of family carers of people living with MND other than spouses and conduct longitudinal studies to capture their experiences at different stages of disease progression. Future research could consider focusing on carers’ knowledge about support possibilities to assess if this information is correctly disseminated. Exploring coping strategies with a coping scale, such as the Brief Cope (Carver Reference Carver1997) which assesses similar strategies found in this study could provide further understanding of mechanisms used in response to different stressors.
In summary, this study examined the emotional journeys that family carers experienced since the diagnosis of MND. Starting with overwhelming feelings of shock and devastation and adapting to the losses and changes occurring subsequently, carers gradually identified several coping strategies to manage their emotions enabling continued engagement in everyday activities, responsibilities, and caring role.
Acknowledgments
We would like to express our gratitude to all the participants for sharing their lived emotional experiences when caring for their family member. We would also like to thank MND Scotland and MND Association for disseminating the study opportunity, and to Chris Bennet, Sue Heal, and the MND team from the Norfolk Care and Research Network for their constant support.
Funding
The authors disclosed the following financial support for the research, authorship, and/or publication of the present article: A.P.T.’s PhD studentship is funded by MND Scotland. T.B. is supported by a research fellowship from the National Institute of Health and Care Research (NIHR) Applied Research Collaboration (ARC) East of England. E.M. is also supported by the Applied Research Collaboration (ARC) East of England.
Competing interests
All authors declared no potential conflicts of interest regarding to the research, authorships, and/or publication of the present article.
Ethical approval
The study was ethically approved by the West Midlands-Black Country Research Ethics Committee (UK) [IRAS 281943, REC 20/WM/0185].




 Open access
Open access