



A chemical, biological, radiological, and nuclear (CBRN) event is “the exposure (or risk of exposure) of a large number of individuals to hazardous Chemical, Biological, Radiological, and Nuclear materials which may occur through a variety of means including natural, accidental, and deliberate acts.” Reference Chilcott and Wyke1 CBRN events can have a large impact on society at a number of levels, with health care systems being significantly affected. Examples of CBRN events are coronavirus disease (COVID-19), a recent global biological event, Reference Djalante, Shaw and DeWit2 the chemical sarin attacks in Tokyo, Reference Okumura, Suzuki and Fukuda3 biological anthrax letters in the United States, Reference Koenig4 use of radioactive polonium-210 in London, Reference Day5 Birling Gap incident in East Sussex, Reference Greenfield6 and the Salisbury Novichok incident. Reference Vale, Marrs and Maynard7
In England, the Civil Contingencies Act (CCA) 8 lays out responsibilities on NHS organizations to uphold civil protection and act as the foundation to emergency preparedness, response, resilience, and recovery. The emergency department (ED) is exposed to the highest risk level in health care. Reference Bleetman, Sanusi, Dale and Brace9 First receivers (ED staff) are required to care for CBRN-exposed patients, risking the danger of becoming patients themselves. Reference Jones, Lukey, Romano and Salem10 CBRN plans (policies and procedures) are used to ensure that the requirements of the CCA 8 and NHS England National Core Standards for Emergency Preparedness Response and Recovery 11 are delivered in NHS organizations.
The ED has been described as a complex sociotechnical system, Reference Braithwaite, Wears and Hollnagel12 where groups of people such as patients, relatives, and clinicians interact with different technologies in various physical and organizational environments. Reference Carayon13,Reference Effken14 Complex sociotechnical systems have been associated with unexpected variability in performance in which patient safety can be compromised. Reference Saurin and Werle15
It has been reported that there is a lack of standardization with regard to NHS emergency planning, and there is an urgent need to standardize national planning, training, and evaluation of NHS staff who are expected to respond to CBRN events. Reference Linney, George Kernohan and Higginson16 This lack of consistency in clinical practice and processes results in variability in practice between health care organizations, departments, and even amongst clinicians, and creates challenges to responding to rare CBRN events.
Standardization aims to embed best professional practice while minimizing the risks of variation; this maximizes consistency of actions across teams, organizations, and the health system. 17 Standardization can overcome variability by “setting formal rules to guide employees‘ activities, which are operationalised in organisations by means of work instructions, guidelines, manuals, and work procedures” Reference Nissinboim and Naveh18 and is defined as “the process of developing, agreeing upon, and implementing uniform technical specifications, criteria, methods, processes, designs or practices that can increase compatibility, interoperability, safety, repeatability, and quality.” Reference Leotsakos, Zheng and Croteau19
The scientific discipline of human factors and ergonomics (HF/E) uses an understanding of physical, psychological, and social abilities and limitations to develop systems with safe, effective, and productive interactions as (re)designed tasks, environments, and tools. It has been recommended that HF/E can be applied to redesign health care work systems and processes to improve the safety and quality of care. Reference Xie and Carayon20
One way of improving work in health care environments is to follow guidelines, policies, and procedures (Work as Imagined, WAI); this is what designers, managers, regulators, and authorities believe happen, or should happen in the workplace. Reference Chuang and Hollnagel21,Reference Saurin, Rosso and Colligan22 Compliance with policies and guidelines would suggest that Work as Done (WAD; what workers actually do) is similar or identical. Reference Chuang and Hollnagel21 However, it has been suggested that absolute compliance with guidelines/procedures/policies is unrealistic because frontline staff need to improvise and adjust their work dynamically to respond to the situation and patient needs. Reference Chuang and Hollnagel21
This study aimed to provide standardized recommendations for the ED response to CBRN events by using hierarchical task analysis (HTA) to compare WAI with WAD.
Methods
HTA describes a task as a higher-level goal with a hierarchy of superordinate and subordinate tasks. Reference Shepherd23 HTA has been suggested to be an effective way of stating how work should be organized to meet a system’s goals. Reference Kirwan and Ainsworth24
Ethics, Study Environment, and Recruitment
Ethical approval was given by the Loughborough University sub-committee (C17-22). Health Research Authority approval was granted through the Integrated Research Application System (219968). Research and Development approval was given from both hospitals.
Data were collected in England at 2 Type 1 EDs defined as “consultant led 24 hour service with full resuscitation facilities and designated accommodation for the reception of accident and emergency patients.” 25 ED-A served a population of 1 million residents, ED-B served a population of 600 000 residents. ED-A treated 237 000 patients, and ED-B treated 116 000 patients during the study period (2016–2017).
First receivers were approached through recruitment posters and information sheets in staff rooms. Nurses in Charge (NIC) discussed the study at a staff handover meeting a week before the researcher attended the ED. Then the researcher attended handover meetings to meet the first receivers and was available throughout the shift for those interested in participating.
Work as Imagined: Document Analysis
An exploratory document analysis of hospital CBRN policies and procedures (plans) was used to develop the preliminary HTA. Document analysis requires data to be thoroughly examined and interpreted to elicit meaning, understanding, and develop empirical knowledge. Reference Bowen26,Reference Corbin and Strauss27 Applied thematic analysis was used to underpin the pragmatic approach, as well as being applicable to practical problems in applied research. Reference Guest, Macqueen and Namey28
Redacted CBRN plans for ED-A and ED-B were provided by the Lead Emergency Planning and Preparedness officer at both hospitals. The CBRN plans (2 parts) from the 2 EDs were analyzed:
-
Part 1: Set the scene for a CBRN event and how the ED should respond as a system within a system (hospital) and a larger system (Category 1 responder).
-
Part 2: First receiver action cards (n = 30).
Action cards (procedures), which are to be given to first receivers when a CBRN event occurs.
Pilot Study
To test the methods, a publicly accessible hospital CBRN plan was downloaded, analyzed, and converted into an HTA representation. The pilot exercise allowed reflection on data collection and available analysis software (eg, Human Factors Risk Manager, Microsoft PowerPoint, and Microsoft Visio). The pilot exercise allowed the formulation of a step-by-step plan for analysis, timescale planning, and familiarization with software; PowerPoint and Visio were used to provide clear and legible illustrations on 1 sheet of paper (of varying sizes), which supported the review/verification phases.
Data analysis
Data were extracted using document analysis and represented as HTAs. HTAs were analyzed with a 4-stage process:
-
1. Familiarization
-
2. Formation of superordinate tasks
-
3. Formation of HTAs
-
4. Manual analysis of HTAs, using applied thematic analysis and thematic color coding to support a comparative analysis
Human factors and ergonomics review
The HTAs were reviewed by 2 ergonomists and an academic with a clinical background (former ED nurse). Ergonomists are professionals who “seek to understand how a product, workplace or system can be designed to suit the people who need to use it.” 29 The review evaluated whether the HTA representations of the CBRN plans were optimal in terms of eradicating duplications. Inconsistences were highlighted with the intention of making the HTA more logical and usable.
Work as Done: Semi-Structured Interviews
An exploratory qualitative design was used to develop the semi-structured interview proforma. Scenario cards were used to present hypothetical patients as a prompt for first receivers to “talk the researcher” through what they would do to respond to the scenario. Scenario cards have previously been used to test incident command systems in hospital-based disaster simulation exercises Reference Thomas, Hsu and Kim30 and as tools for planning, improving, and handling CBRN events. Reference Sandström, Eriksson and Norlander31
The scenario cards were created from CBRN literature, observations at CBRN tabletop exercises at NHS hospitals, and Health Protection Agency (HPA) guidance. 32 A Hazardous Area Response Team (HART) specialist reviewed the CBRN scenario cards to ensure that they were realistic. Three scenario cards included:
-
1. Chemical: sarin
-
2. Biological: severe acute respiratory syndrome (SARS)
-
3. Radiological: acute radiological syndrome (ARS; Figure 1)

Figure 1. ARS scenario card.
Pilot Study
Each scenario card was piloted with 2 participants. The pilot data allowed initial HTAs to be developed and compared.
The ease of creating the pilot HTA (Figure 2) confirmed that presenting the scenario card in the ED would provide valid and reliable insights into ED responses.

Figure 2. First receiver (ED consultant) response to ARS scenario card.
The use of scenario cards in disaster management research
Obtaining valid and reliable insights into how first receivers would respond to CBRN-exposed patients was important. CBRN events could not be anticipated ethically or created due to the life-endangering nature. Therefore, a variety of means were explored to determine the optimal method, such as software simulations, tabletop exercises and drills, and scenario cards. Scenario cards were selected because they have been reported as efficient and effective tools for planning, improving, and handling CBRN events. Reference Sandström, Eriksson and Norlander31 Scenario cards were cost-effective, not time-consuming, and allowed the continuation of patient care.
Sampling
Participants were recruited from the 2 EDs. The inclusion criteria were ages 18 years and over, more than 3 months’ ED experience, ED as location of work, and belonging to first receiver staff group of allied health care professionals, doctors, medical physicists, nurses, porters, receptionists, and security staff, and employed in the ED for a minimum of 3 months on a substantive (permanent) contract.
A total of 57 participants were recruited (ED-A: 17 females and 11 males; ED-B: 13 females and 16 males). Ages ranged from 21–60 years (mean = 39 years, SD = 10). Participants were employed by the NHS in a different role or different department for an average of 12 years (SD = 8). The length of employment in the ED ranged from 3 months to 20 years (mean = 8 years, SD = 5).
Purposive sampling was used to identify and select individuals who were especially knowledgeable about, or experienced with, the phenomenon of interest. Reference Creswell and Plano-Clark33 A representative sample was ensured by calculating the percentage distributions of first receivers on a typical shift.
Data collection
During the first phase of semi-structured interviews, data were collected to obtain insights into WAD. Scenario cards were presented to first receivers. They were given time to read it and then asked to talk through their planned actions. Probes were used to expand on responses with “what, why, and who” questions. Field notes were made, which were later transcribed.
The second (verification) phase used the HTA developed from the first phase interview data. The verification process followed methodological guidance Reference Stanton34 to confirm the validity of the HTA representation (member checking). The verification process used the scenario card as a memory aid and explained the functions of HTA. The first receiver was then asked, “Do you think this diagram is a true representation of what you would do in a CBRN event?”—and they were prompted to discuss and amend the HTA.
Data analysis
Each transcript from the first phase (semi-structured interview) was read for familiarization to ensure complete immersion with the data. The field note and interview data were converted into HTAs (n = 57), using both Visio and PowerPoint. The HTAs were printed for manual analysis, and applied thematic analysis was used to systematically identify, organize, and code for patterns of meaning (themes) across the data set. Reference Braun and Clarke35
The synthesis of the themes provided a bottom-up perspective to standardization for WAD.
Rigor and credibility
Rigor is relevant to the reliability, validity, and reduction of bias in qualitative research. Reference Bowling36 Credibility, transferability, dependability, and confirmability Reference Lincoln and Guba37,Reference Yilmaz38 are evidenced in Table 1.
Table 1. Addressing criteria for rigorous research Reference Lincoln and Guba37,Reference Yilmaz38

Results
It was found that the ED response to CBRN events was different between the EDs for Work as Imagined (operational procedures) in terms of General Organizational Responsibilities (GORs). ED-A had 13 GOR themes and ED-B had 20 GOR themes, of which 13 overlapped, for themes such as decontaminate, don personal protective equipment (PPE), and isolate and contain. The HF/E review identified variance in the action cards for the following:
-
1. Prepare to respond to CBRN incident (ED-A and B).
-
2. Respond to CBRN incident (ED-A and B).
-
3. Initiate recovery from CBRN incident (ED-A).
-
4. Document CBRN incident (ED-A).
Color coding was used to illustrate the difference in the number of top-level tasks between ED-A and ED-B for the pre-incident, incident, and recovery phases (Figure 3 and Figure 4).
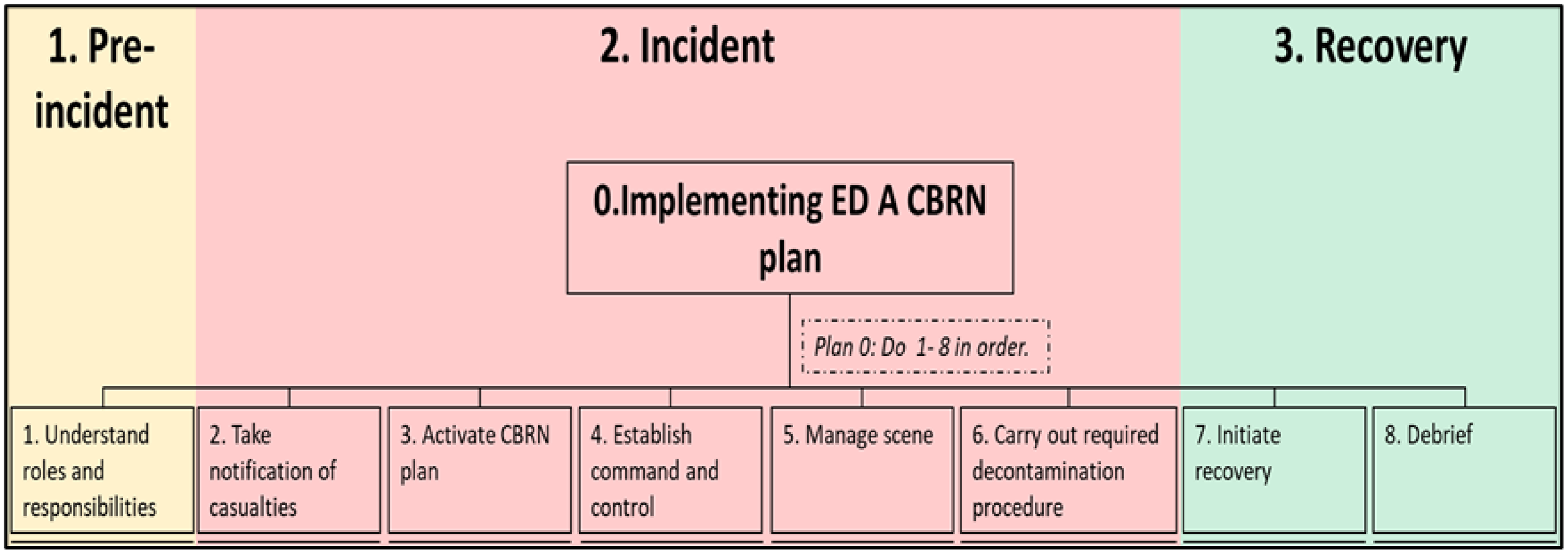
Figure 3. ED-A: GOR superordinate tasks.

Figure 4. ED-B: GOR superordinate tasks.
The pre-incident phase establishes an understanding of the potential actions required by the EDs for an effective response in liaison with other organizations such as Emergency Medical Services (EMS). The activation of the CBRN response was identical at both EDs.
The CBRN incident phase started with the notification of casualties. There was a difference in the incident phase with ED-A being more categorical in the response steps by having individual superordinate tasks such as “carry out required decontamination procedure.” ED-B combined the individual superordinate tasks under “respond to CBRN incident” and discussed specific CBRN procedures such as decontamination under “implement action pack.” An additional difference was the emphasis on documentation for operational procedures.
Both EDs stepped down from responding to the CBRN event by “initiating recovery.” At ED-A, recovery was associated with the decontamination of departmental infrastructure and the well-being of first receivers. At ED-B, recovery was a statement of ending the CBRN response.
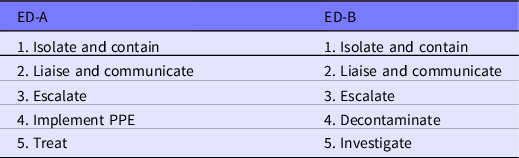
The semi-structured interviews provided insight into working practice (WAD). Nurses in Charge (NICs) at ED-A managed CBRN presentations by taking the lead while protecting their team and the environment. Nurses implemented crucial CBRN actions such as isolate and contain. There was a lack of involvement in the importance of carrying out decontamination amongst senior nurses across both EDs. Doctors made decisions at ED-B, and senior doctors additionally secured the department and managed staff. There was variability in the importance placed on key CBRN tasks for implementing PPE, decontamination, treat, and investigate (Table 2).
Table 2. Standardized main tasks in response to a CBRN presentation
Similarities between WAI and WAD at both EDs were that first receivers (WAD) prioritized patients’ needs (treatment, diagnosis, and patient care) compared with WAI. Senior nurses did not include decontamination in their CBRN response, even though leading the decontamination process was core to their role, based on operational procedures.
In terms of differences, WAI focused on documentation, whereas documentation was minimally discussed by first receivers at ED-B only. Additional differences were evident with most WAI action cards consisting of 3 phases at ED-A and 2 phases at ED-B. Furthermore, ED-B first receivers adhered more to WAI compared with ED-A first receivers, which was evidenced by ED-B first receivers including WAI themes in their responses to scenario cards.
The analyses of WAI and WAD provided an insight into the multi-dimensional variability across the CBRN response for first receivers. Variability was evident through differences in the number of first receivers included in the response, having different nursing roles across EDs, and unspecified banding/experience for CBRN roles.
Limitations
Data were generated from a purposeful sample at a single point of time, giving rich data but can also be a limitation, which is common in critical care services research. Reference Fealy, Donnelly and Doyle39 Collecting the data at a single point was planned for 2 reasons. First, CBRN events cannot be anticipated, and a real-time response was sought. Second, EDs are under extreme pressures with demand constantly exceeding capacity, in which challenges associated with overcrowding lead to stress in staff resulting in the high turnover. 40 As first receivers work varying shifts, a single point of data collection was the most appropriate to allow a quick turnaround time for verification interviews. It is important to note that the participating first receivers were a limited group, which excluded domestic employees and technicians; these individuals play a vital role in diagnostic testing and sanitization of infectious areas in the ED and should be included in future CBRN research.
Discussion and Recommendations
This study confirmed alignment between CBRN procedures and practice in the ED response to CBRN events, with actions such as isolation, escalation to senior first receivers, and activation of the CBRN plan being crucial. These actions aim to minimize the risk of secondary contamination, a known phenomenon in acute hospitals when responding to chemical events. Reference Larson, Orr and Auf der Heide41
Operational procedures (WAI) in the ED CBRN response differed between both EDs, in terms of general organizational responsibilities having varying phases as well as action cards consisting of varying top-level tasks.
Misalignment between CBRN procedures and practice was clear through a lack of emphasis on documentation, as evidenced through the limited discussion by first receivers. This can be explained by the busy, interruptive, and multi-tasking nature of the ED, which has been reported to delay or divert from documenting efficiently, Reference Sujan, Spurgeon and Inada-Kim42,Reference Werner and Holden43 as well as deviate from standardized operating procedures (SOPs). Reference Jones, Fawker-Corbett and Groom44
CBRN operational procedures (WAI) focused on actions such as documentation, checking, timing, and providing equipment, whereas CBRN practice (WAD) focused on the patients’ needs. A possible explanation is through the Prioritization of Tasks versus Prioritization of Patients’ Needs dichotomy, which includes assessment, treatment, and diagnosis. Although priority is given to minimize the number of deaths, it is advised to prioritize decontamination procedures to reduce the casualties’ exposure to CBRN materials prior to clinical treatment. 45
CBRN guidance protects responders from contamination; however, by nature, responders are known to help, as evidenced by the police officer contaminated in the Salisbury Novichok incident. Reference Clarke and Weir46 This explains why first receivers prioritize the needs of patients rather than follow guidance, such as keeping a paper trail of actions taken and prioritizing decontamination to minimize contamination.
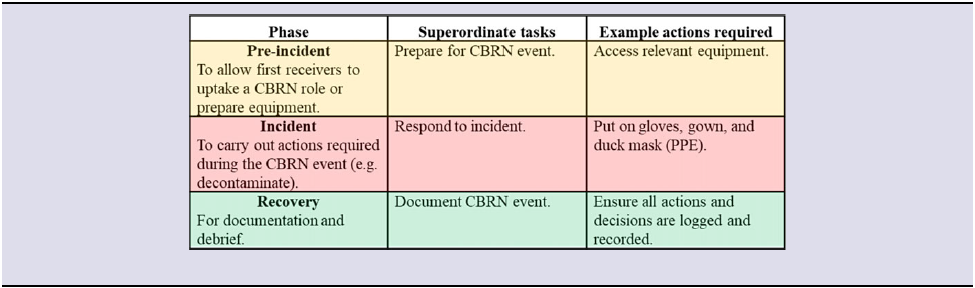
Responding to a CBRN event is a complex, multifaceted, and a non-routine work situation, which consists of variability (ie, decontamination void); it is suggested that standardization can reduce the reliance on team experience to ensure a safe and effective practice. Reference Künzle, Zala-Mezö and Kolbe47 The standardization of superordinate tasks for first receivers through document analyses and HF/E review introduced clarity and order across tasks, as illustrated in a standardized CBRN action card template for first receivers (Figure 5). Templates have been recommended to allow the implementation of “the choice approach” to standardization, Reference Nissinboim and Naveh18 which allows clinician discretion and encourages naturalistic decision-making. Reference Catchpole and Alfred48
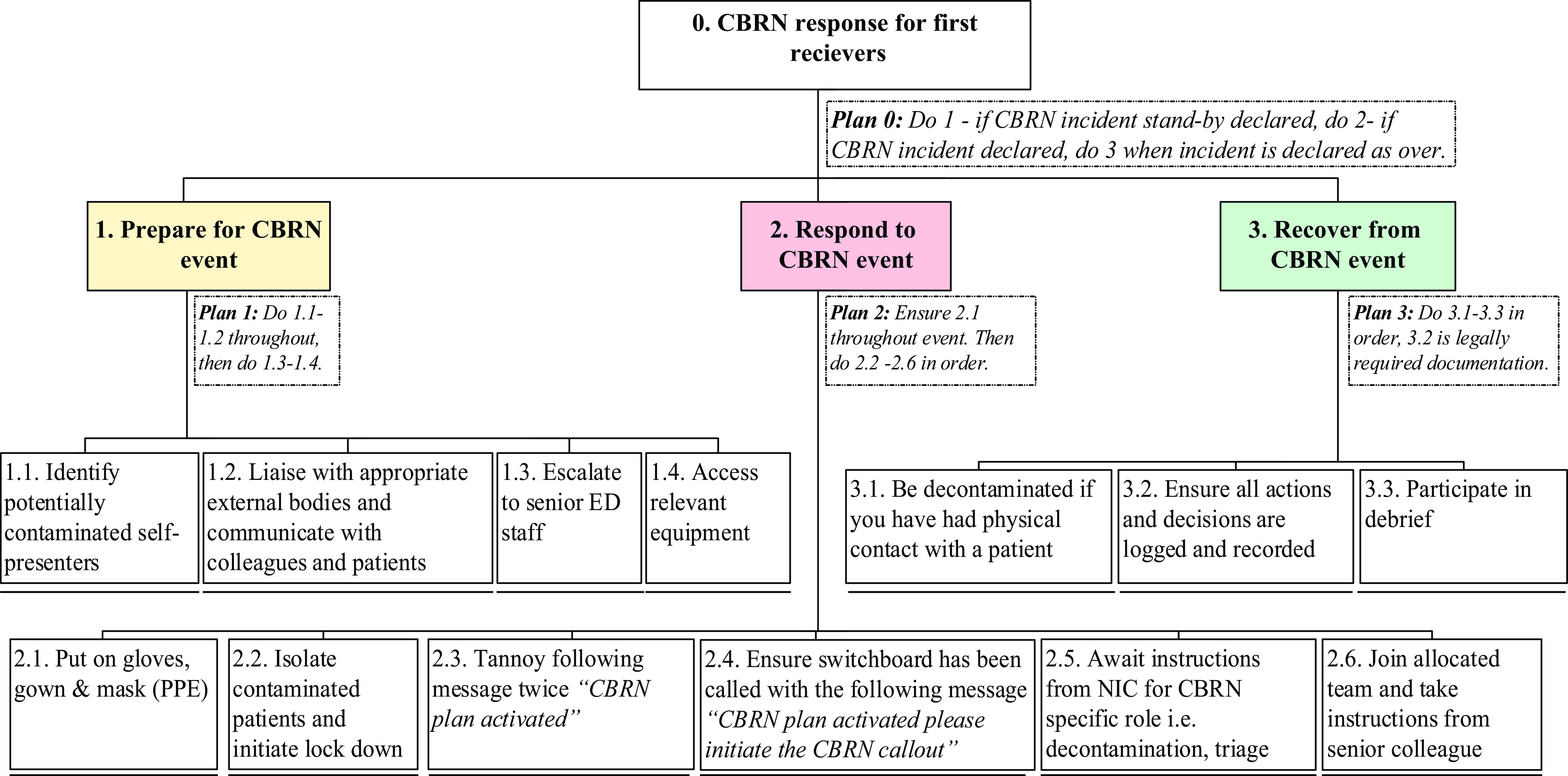
Figure 5. Standardized CBRN action card for first receivers.
To support effective standardization, the process needs to be well defined, described, and reproducible. Reference Schleef, Cherti and Guida49 It is recommended that the number of phases in a CBRN event should be defined and described through superordinate tasks, which are broken down into actions that are reproducible, as shown in Table 3.
Table 3. Standardized action card recommendations
This study synthesized WAI and WAD and identified phases of the ED CBRN response in line with previous literature Reference Johnson and Cosgrove50 consisting of general phases (initial response, consolidation phase, and recovery phase) for hospitals responding to major incidents (including CBRN events) and the following:
-
1. Evacuation
-
2. Triage
-
3. Decontamination for vulnerable individuals during CBRN emergencies Reference Hignett, Hancox and Otter51
Categorizing CBRN actions into phases allows the streamlining of an effective CBRN response, for example, by preparing for the arrival of casualties in line with previous findings Reference Jasper, Miller and Sweeney52,Reference Waage, Poole and Thorgersen53 as a means of freeing resources to deal with the surge of casualties.
There is no standardized system globally or nationally for key CBRN actions such as triage and decontamination. Reference Ramesh and Kumar54 The HF/E review resulted in CBRN GORs and action card HTAs, which flowed systematically, without repetitions, with clear allocations, and standardized phases of response. The updated HTAs were combined with the scenario card responses, and the themes aligned to give a complete integration of operational procedures (CBRN plans) and practice (first receiver responses). This forms the recommended standardized ED CBRN framework, shown in Figure 6. The standardized CBRN framework implements findings that overcome CBRN challenges associated with detection, decontamination, and diagnosis as reported previously. Reference Razak, Hignett and Barnes55 It implements systems that are flexible, easy to follow to the available medical resources, number of casualties, and severity of injuries, encouraging its usability. The framework provides an evidence-based, simplified template to respond to a multi-faceted CBRN event.

Figure 6. Standardized CBRN framework (represented as an HTA).
Conclusion
This research identified variability between WAI and WAD in the ED response to CBRN events by combining HF/E method (HTA) and theory. The findings were synthesized to provide a top-down and bottom-up insight to enhance the ED CBRN response through standardization. The standardized CBRN action card template embeds the choice approach to standardization by offering clinician discretion, which accounts for the prioritization of tasks and prioritization of patient’s needs dichotomy.
The standardized CBRN framework combines the categorization CBRN of phases, addresses challenges of detection, decontamination, and diagnosis, as well as aligning variability between operational procedures and practice. Finally, this study identified 2 key messages: WAI versus WAD is a useful theoretical framework to unpack a complex sociotechnical system, and HTA is an effective systems mapping tool in health care.
Funding statement
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict(s) of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.










 Open access
Open access