



1. Introduction
Priority-setting is a salient topic in health care systems, including the National Health Service (NHS) in England. During the Covid-19 pandemic, issues of priority-setting became acutely visible given the extraordinary demands of having to care for a high number of Covid patients in addition to non-Covid patients. While the pandemic increased the public awareness of the challenging decisions that frontline health care staff face, the core issue of how to allocate limited health care resources fairly is not novel. Several frameworks exist to inform and evaluate the fairness of priority-setting, for example Daniels and Sabin's (Reference Daniels and Sabin1997) Accountability for Reasonableness (A4R) framework, Clark and Weale's (Reference Clark and Weale2012) social values framework, and Kieslich's and Littlejohns' (Reference Kieslich and Littlejohns2015) Decision-Making Audit Tool (DMAT). These frameworks have been used to assess priority-setting processes in different countries, and at different levels of decision-making (e.g. Kapiriri et al., Reference Kapiriri, Norheim and Martin2009; Maluka et al., Reference Maluka, Kamuzora, San Sebastiån, Byskov, Olsen, Shayo, Ndawi and Hurtig2010; Coultas et al., Reference Coultas, Kieslich and Littlejohns2019;Littlejohns et al., Reference Littlejohns, Kieslich, Weale, Tumilty, Richardson, Stokes, Gauld and Scuffham2019); Charlton, Reference Charlton2020; Tumilty et al., Reference Tumilty, Doolan-Noble, Gauld, Littlejohns and Stokes2022), showing that priority-setting is a complex undertaking and that there are limits to the usefulness of ethical and technical frameworks (Peacock et al., Reference Peacock, Mitton, Bate, McCoy and Donaldson2009; Kieslich et al., Reference Kieslich, Bump, Norheim, Tantivess and Littlejohns2016). The limitations are further brought to light by studies examining how priority-setting happens in the ‘real world’, where context, politics and historical trajectories exacerbate the challenges of setting priorities in a fair and transparent manner through formalised processes (e.g. Gibson et al., Reference Gibson, Martin and Singer2005; Kieslich, Reference Kieslich2012; Robinson et al., Reference Robinson, Williams, Dickinson, Freeman and Rumbold2012; Kislov et al., Reference Kislov, Checkland, Wilson and Howard2023).
This article contributes to the empirical literature on priority-setting at the local (meso) level by reporting the findings of a qualitative interview study conducted between 2017 and 2018. The aim of the study was to understand if and how Clinical Commissioning Groups (CCGs) follow principles set out in frameworks for ethical priority-setting when they make decisions on which services to fund. We found that the ability of decision-makers to follow such principles was curtailed by the changes resulting from the Health and Social Care Act (HSCA) 2012 and the National Health System (NHS) Five Year Forward View (NHS England, 2014), including significant changes with regard to who is responsible for commissioning health services, and how different services work together. Concerns about the balance between central or local-led health care planning, a lack of clarity regarding mandates and accountability, difficult financial situations, and challenges surrounding the operationalisation of principles such as transparency were identified in the study as issues that influence priority-setting at the local level. We analyse what these findings imply for extant frameworks for health priority-setting and draw on the political science literature on health care reform, path dependency and policy change to show how frameworks such as the DMAT might be adapted to better incorporate issues of context and politics. We offer a set of considerations for what such an adaptation might look like, thus building on Smith et al. (Reference Smith, Mitton, Davidson and Williams2014) who argue that there are analytical and practical benefits to applying insights from political science and public policy. Despite the fact that CCGs were replaced by Integrated Care Systems (ICSs) in the Health and Care Act 2022 (HCA), our findings offer important lessons for priority-setting in theory and practice as they point to a disconnect between the normative aspirations of frameworks for priority-setting and the complex, political realities of setting priorities in practice.
2. Background and extant knowledge
CCGs were established by the HSCA 2012. They were organisations led by groups of general practitioners (GPs) that plan and commission services for local populations. Following the HSCA 2012, NHS England (NHSE) published a strategy called the Five Year Forward View that aimed to guide NHS managers and providers in making the NHS sustainable for the future, especially against the background of rising health care costs. The emphasis was on public health, prevention and integration, all of which are familiar features of health care reforms in Europe (Dixon and Poteliakhoff, Reference Dixon and Poteliakhoff2012). Following the NHS Five Year Forward View, Sustainability and Transformation Partnerships (STPs) were established as pan-regional collaborations of health care planners, providers and local government councils to develop integrated health care plans. Some of these STPs morphed into ICSs, for which the HCA 2022 provides the legal foundation (The King's Fund, 2022). When we conducted the interviews for this study, ICSs still functioned as non-statutory bodies that planned health care for their populations across areas bigger than CCGs.
The brief overview of the current NHS system illustrates that it is characterised by ongoing changes, and by multiple organisations and players. This feature of the NHS system is set against the challenge of resource scarcity. Pressures on health care budgets are rising due to aging populations, the availability of new and expensive pharmaceuticals, austerity measures introduced after the 2008 financial crisis and, more recently, the Covid-19 pandemic. At the same time, there are increased efforts to rectify poor quality standards in areas of NHS patient care following a number of care scandals in the last decade (see e.g. The Mid Staffordshire NHS Foundation Trust Public Inquiry, 2013). Against this background, it is assumed that setting priorities, and decommissioning services, is an inevitable task for health care planners. Put simply: ‘Priority setting in health aims to determine what, in the context of limited resources, is most important’ (Clark and Weale, Reference Clark and Weale2012: 293).
Tools and frameworks developed to aid priority-setting include technical approaches incorporating health economic analyses of costs and benefits, or ethical approaches incorporating principles of fair and ethical decision-making. The latter have been used to evaluate and examine decision-making on resource allocation at a local level (e.g. Robinson et al., Reference Robinson, Williams, Dickinson, Freeman and Rumbold2012; Kislov et al., Reference Kislov, Checkland, Wilson and Howard2023), showing priority-setting at this level is mostly informal, implicit and guided by a number of contextual factors. Daniels and Sabin's (Reference Daniels and Sabin1997) A4R framework is one of the most prominent frameworks for fair priority-setting. Based on notions of procedural justice, Daniels and Sabin (Reference Daniels and Sabin1997) argue that individuals are more likely to accept the outcome of a controversial decision if it is based on a fair and transparent process, even if they do not agree with the substance of the decision. They outline four conditions that need to be met for a priority-setting process to be considered fair: (1) publicity, (2) relevance, (3) appeals and (4) enforcement. The publicity condition refers to the principle that decisions, and the processes leading to them, should be transparent. They should also be made on relevant grounds and explained in a transparent manner, which is contained in the second A4R condition. Stakeholders and the public should have the opportunity to appeal to decisions and, lastly, organisational structures and mechanisms should be structured in a way that allows for enforcement of conditions 1–3.
While prominent, Daniels and Sabin's framework has been criticised on several grounds, for example, on the ground of not providing clarity about what a ‘relevant’ criterion could or should be, or who defines relevance (Rid, Reference Rid2009). Others have argued that A4R incorporates process values without much regard for content values such as cost or clinical effectiveness (Clark and Weale, Reference Clark and Weale2012). The DMAT builds upon Clark and Weale's social values framework by outlining four principles of process values (institutional setting, transparency, accountability and participation) and content values that contain a mix of technical and social considerations (clinical effectiveness, cost effectiveness, fairness and quality of care), which can help evaluate and understand how priority-setting decisions are made.
Despite these aids, scholars agree that priority-setting in health care raises intractable problems that require careful judgements when making decisions (e.g. Weale, Reference Weale1998; Klein, Reference Klein2010). Empirical knowledge on how priorities are set in practice, however, remains sparse, even though such knowledge helps in identifying the kind of judgements, criteria and challenges that concern decision-makers. This is especially the case for the micro and meso levels of priority-setting, where studies remain few and far between. The studies that do exist show that priority-setting at the local level is implicit, informal and/or not happening in a way that frameworks for fair priority-setting would recommend (Robinson et al., Reference Robinson, Williams, Dickinson, Freeman and Rumbold2012). A recent study of priority-setting for service improvement in English primary care even went as far as noting that: ‘It found no evidence of formal priority setting approaches being adopted across the region’ (Kislov et al., Reference Kislov, Checkland, Wilson and Howard2023: 8). This article contributes to the still limited number of studies examining the realities of local priority-setting by offering insights from interviews with CCG decision-makers and stakeholders on how resources are allocated.
3. Methods
The article addresses the following research question: How do CCGs make decisions on which services to fund and to prioritise, and to what extent do they consider principles of fair priority-setting in their decision-making? In this section, we outline the methods we employed to answer this question, loosely following the consolidated criteria for reporting qualitative studies (COREQ) (Tong et al., Reference Tong, Sainsbury and Craig2007).
3.1. Study design
We draw on data from a qualitative interview study of CCG priority-setting in South London. The interviews were carried out between October 2017 and May 2018. The semi-structured interviews focused on participants' understanding of priority-setting principles drawn from the DMAT (accountability, transparency, participation, clinical effectiveness, cost effectiveness, fairness, quality of care) as well as their understanding of other factors that bear upon CCG decision-making. The interview guide included questions about the criteria that the CCG uses to make decisions, how it balances between different, and sometimes competing, criteria such as clinical and cost effectiveness, and about the participants' understandings of principles such as transparency, fairness and legitimacy in the priority-setting process. The effects of the HSCA 2012 were not contained in the interview protocol, but emerged as issues of relevance in all but three interviews (Coultas et al., Reference Littlejohns, Kieslich, Weale, Tumilty, Richardson, Stokes, Gauld and Scuffham2019).
3.2. Participant recruitment
Eighteen individuals connected to 12 CCGs were interviewed in the study: nine CCG governing board members (voting members), two CCG staff members (non-voting) and seven Healthwatch representatives (see Table 1 for an overview). Healthwatch was established under the HSCA 2012 as an organisation with a statutory mandate to represent the views of people who use health and social care services in England (Healthwatch, 2022). As such, it has insights into commissioning for health care at a local level and is involved in commissioning processes.
Table 1. Interviews

The interviews took place at either the CCG offices or at the university department in which our research team was based at the time. In two cases, interviews took place at a café in South London. Interviews lasted between 25 (shortest interview) and 100 minutes (longest interview). Interviews were digitally recorded and transcribed verbatim. Ethical approval for the study was obtained from the King's College Research Ethics Committee.
Interviewees were recruited using a mix of purposive and snowballing sampling techniques. CCG board members, patient and public groups and Healthwatch organisations in London were invited by email to take part in the study. Despite multiple efforts on behalf of the researchers, including a follow-up to the original interview request by telephone, the response rates remained small. Several Chairs of CCG governing boards declined to partake in the study, citing severe time constraints as a reason. Despite this, the collected data contained a range of views that gave good insights into how priorities are set in health care decision-making at the local level. We were able to identify common themes, such as the challenges of ongoing reforms, after the first few interviews had begun. The topics discussed in this paper were identified as red threads in the data set.
Regarding the self-selection bias that may occur when only a small number of participants respond to an interview request, we were encouraged by the open and candid way in which the interview partners responded to questions. We hope this minimises the likelihood that self-selection bias or social desirability bias played a role in the data. Moreover, the fact that several potential interviewees declined the interview request due to time constraints underlines the daily pressures faced by commissioners; this was also highlighted by many of our interview partners. Some of these pressures relate to the efforts of implementing ongoing reforms, as shown in the findings section.
We cannot rule out for certain that the findings are skewed towards an urban setting considering the study's focus on South London. We would expect that interviews in other parts of London may have brought similar insights; for other parts of England differences may have emerged because challenges might be different in more rural areas (due to, e.g., longer distances between health care services and providers, access challenges for the elderly population, or workforce problems in rural parts of the country). Even with these caveats, however, our findings are similar to other studies of local priority-setting (Maluka et al., Reference Maluka, Kamuzora, San Sebastiån, Byskov, Olsen, Shayo, Ndawi and Hurtig2010; Robinson et al., Reference Robinson, Williams, Dickinson, Freeman and Rumbold2012) and hold valuable lessons for the effects of health care reforms on local priority-setting.
3.2. Data analysis
The transcripts were analysed using a mix of deductive and inductive content analysis. The deductive approach was informed by the DMAT (Table 2), which was used as a coding scheme. The DMAT combines a set of process and content criteria presented in the literature as important for evaluating the fairness of priority-setting in health care. The process criteria are institutional setting, transparency, accountability and patient and public participation. The content criteria are clinical and cost effectiveness, fairness/equity and quality of care. The definitions that guided the coding process can be found in Table 2. They are based on Clark and Weale's (Reference Clark and Weale2012) conceptualisations. The criterion ‘quality of care’ was added to the DMAT following two pilot workshops with stakeholders in South London in 2015, who felt it was important to include questions about quality in evaluating priority-setting processes.
Table 2. The Decision-Making Audit Tool (DMAT)
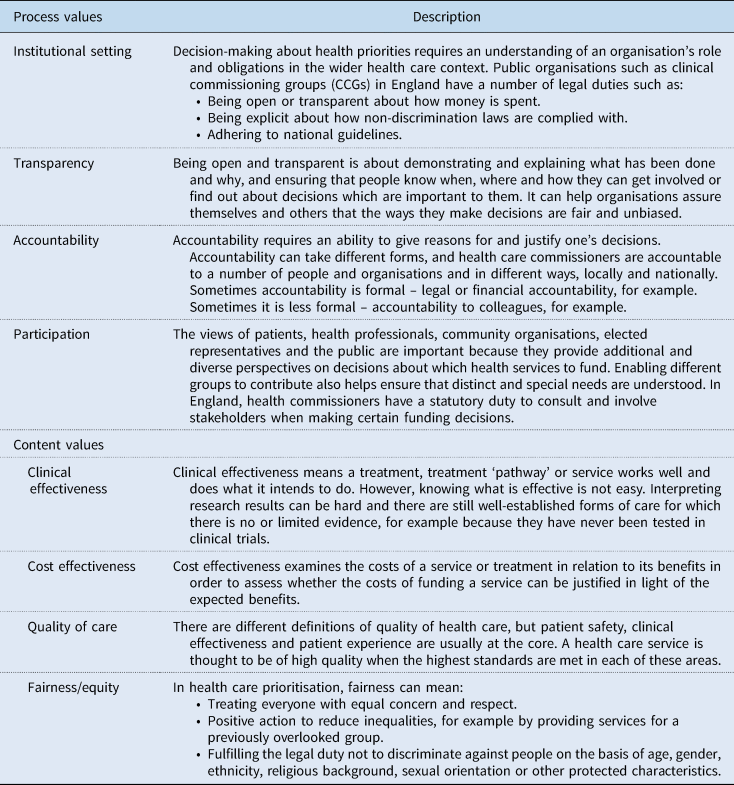
In addition to the findings from the coding process, themes relating to the contextual and political elements of priority-setting, and to the effect of recent health care reforms, emerged inductively. The interview data were double coded manually by two researchers of the team. Based on Berg's (Reference Berg2008) guidance on content analysis, a theme was labelled as dominant when it appeared in three or more instances, both within and across interviews. Themes were identified and interpreted through discussions between the authors.
4. Findings
Interviewees described a range of factors as influencing prioritisation decisions at CCG level. The considerations include reflections on principles of fair priority-setting that respondents were asked about, such as transparency, as well as factors that they were not specifically asked about, such as the effect of ongoing health care reforms. A thorough analysis of the challenges of conducting meaningful public and patient involvement (PPI) is published elsewhere (Coultas et al., Reference Coultas, Kieslich and Littlejohns2019, Littlejohns et al., Reference Littlejohns, Kieslich, Weale, Tumilty, Richardson, Stokes, Gauld and Scuffham2019) and only forms a small part of the discussion that follows.
4.1. The financial context: austerity and the lack of discretionary funding
Several interviewees reflected upon the difficult financial situation of the NHS. Rather than being able to make new investments, the system has been under pressure to make savings wherever possible. According to our interviewees, this leads to a situation in which there is little room for setting local priorities because the discretionary spend of CCGs is limited by existing commitments that must be met.
Well, […] there is very little discretionary spend in the overall budget. Our budget is something like £460 million. […] But when you look at where the money comes from and what it's already allocated to, there's very little discretionary spend. We are pretty good on contract management. You know, the non-discretionary spend. (CCG lay member 3)
This interviewee went on to explain how the CCG must meet a number of financial commitments within its annual budget. These include covering services that cannot be stopped or changed, for example, statutory provisions such as acute care. Then there are priorities that are set at the national level, such as the focus on mental health, population health and prevention. There are also multiple contractual obligations with providers that must be met, something the interviewee refers to as ‘contract management’. Here, there is some room for manoeuvre regarding cost efficiency in the system, but these possibilities are subject to negotiations. Another interviewee presented the problem of lack of funds for discretionary spending as follows:
[…] there is very little genuine discretion on expenditure, because […] most of it is demand-led. […] We have a total budget of quarter to half billion. About half, possibly more than half, goes to acute, roughly half, call it – then you've got mental health, community services, primary care. All of those have, as it were, existing histories and taps that you can't just turn off. And in the absence of growth, actually the debate – although it used to be about, about what to do with the marginal additional money you had, and that was the debate up to about a couple of years ago. I mean [Name of London borough redacted for confidentiality], our funding was reasonably, reasonably okay. And so each year we were able to genuinely to invest in new services, new initiatives and so on. At the moment, because the taps have been turned off basically in real terms. […] the debate is increasingly about where you can make savings and efficiencies. (CCG lay member 2)
The quote underlines that the budgets do not allow for significant discretionary spending once the CCG has met all its commitments. It also illustrates that financial pressures have been getting worse over the years with less and less room for new investments. Interestingly, respondents did not reflect upon the fact that formal priority-setting processes could help with decisions on how to spend the few discretionary funds that remain. Instead, what participants insinuated was that there was so little money left that formal priority-setting was rarely pursued.
4.2. The reform context: effects of the HSCA 2012 and the NHS Five Year Forward View
When asked about the process and context of priority-setting, many interviewees reflected on the effects of the HSCA 2012 and the NHS Five Year Forward View. They expressed doubts about the HSCA 2012 reforms achieving the aim of de-centralising health care planning, and of making health care more responsive to local needs. According to several participants, centrally mandated performance and accountability targets, as well as NHSE's perceived objective to regain control over health care planning, were obstacles to the HSCA's goals of decentralisation.
I think its [the CCG's] autonomy is […] curtailed by all this accountability. […] it's […] NHS England trying to take back control, because the whole point of Lansley's [Secretary of State for Health Care and Social Care in 2012] reforms was to have the Department of Health at arm's length from health care commissioners and providers. And that this looks like to me, on the ground, it's very much direct management by NHS England. (CCG Chair 2)
CCGs are subject to an enormous amount of top-down direction from the Department of Health and, you know, through NHS England. […] an enormous amount of target-setting and […] they are made […] accountable for both their own budget and the quality of the services they commission, and […] the things that they can't […] easily directly control, like the performance of hospitals. […]. (CCG Chair 1)
The above quotes highlight concerns that top-down directions in health care continued after the HSCA 2012 reform. The interviewees cited targets such as quality performance measures in multiple areas, even in areas such as hospital performance that were outside the control of CCGs, as indicators that top-down control of health care planning continued. The role of NHSE as the national body that leads the health service in England was repeatedly mentioned as the driver for continued top-down control of local commissioners through central government. The Five Year Forward View, introduced by NHSE in 2015 as a strategy to help tackle the challenges faced by the NHS, was seen as a policy that exacerbates the complexity of CCG decision-making by introducing requirements for integration with local governments and other players. As the following interview excerpt shows, however, it is not the principle of integration that is questioned, but the way NHSE sought to achieve it through measures that were seen as being in conflict with previous market-focused reforms.
[…] there is a big issue now about the extent to which the NHS should operate as a quasi-market and to what extent they should operate as a managed service. […] Lansley […] his whole model […] postulated that it's a quasi-market. But the pressure now is […] towards collaboration and working together. […] And not let the market get in the way of that. And that's […] created difficulties, because the structure isn't […] geared for that. […] the market […] says that every provider […] should operate as an island […] in competition with others. (CCG lay member 1)
These reflections reveal tensions between the infamous purchaser–provider split that has existed in the NHS since the 1980s and the HSCA 2012 reforms. According to some interview respondents, the local structures and contractual capabilities of local decision-makers were not set up to transition to more integrated ways of working:
[…] there's an acute contract […] which was to bring together our two main acute hospitals, which are both outside of the borough […] with the community provider […] and our GP alliance. And that they would hold shared responsibility for providing care to the population, which, it's a great idea. But […] the acute trusts didn't really sign up […] to the risk-sharing side of the agreement, the financial side of the agreements. […] so the process has been […] stymied. (Healthwatch manager 3)
The quotes show that questions surrounding the core ambitions of the HSCA 2012 reforms and NHSE's ensuing policies led to uncertainties about the relationship between commissioners and providers at the local level. These uncertainties affect, and sometimes even stifle, priority-setting because decision-makers are unclear about their role(s) or roles of the people or entities they work or negotiate with. As described by one of the interviewees in the previous section of this paper, one of the ways that commissioners can set priorities is through effective contract management. This, however, requires all parties to contract negotiation to subscribe to the same basic premises of rules and roles. If rules and roles are undergoing changes due to reforms or other factors, then priority-setting will likely become more challenging. The above excerpt suggests this is the case as this particular CCG's priority seems to have been to create efficiencies by bringing together different care providers whilst the hospital providers did not sign up to crucial parts of the agreement, i.e. the sharing of financial risk. It shows that local health care commissioners are influenced and curtailed by reforms, which take time to implement; during this time, priority-setting is even more constrained by context than usual.
4.3. The political and historical context: how the past affects the present
Interview respondents discussed the need to have public discussions about NHS priorities and what the NHS can afford, whilst acknowledging that this is a challenging undertaking. Several respondents referred to successful public campaigns to protect local services from changes or closures as examples that decrease the chances of successful changes at the local level because of the precedent that is set.
[…] a few years ago, we had a big programme called ‘Better Service, Better Value’, […] which then got stopped. […] it failed for all sorts of reasons. [There were] […] strong clinical arguments as well as financial ones as to why something had to change. […] when we did public consultation about those high principles, people bought it. […] but when you turn it to, so which one is going to change or close, […], you know, different entirely. […] We had demonstrations in […] meetings, we had placards, we had politicians turning up, giving speeches, questioning the personal motives of, […], people on the panel. […] when it gets down to that level, […] you're not actually having a rational discussion any more. You're having, […] – it is politics, capital P, small p […]. (CCG lay member 3)
It was […] an interesting exercise in how you […] successfully harness […] public pressure. [….] that's become a […] powerful part of [Name of London borough redacted for confidentiality] kind of whole understanding of what it means to keep […] local services. [….] therefore we slightly have an even tougher problem. […] what I found when I […], and this is not for the CCG, this is when I've just gone out and talked to friends, neighbours, […], that comes up each time, we saved […] [the] hospital and therefore we're going to save it all. You know, […] nobody's going to do anything to [Name of London borough redacted for confidentiality] ever again. (CCG lay member 2)
These statements speak to the contextualised nature of setting priorities. Depending on local historical trajectories, certain priority-setting endeavours or reform measures may or may not be possible. The respondents outline instances in which proposals to close and transfer services to other hospitals or other providers were halted by opposition from local populations and politicians, even when a clinical case for setting certain priorities could be made. This has implications for the implicit, and sometimes explicit, argument contained in frameworks for fair priority-setting about the rational and technical nature of the priority-setting process, i.e. that a solid rational or technical case for the need of change will increase the chances for public acceptance. The above excerpts, however, suggest that this is not necessarily the case: once change resulting from prioritisation efforts is seen to affect the local hospitals and services that are of communal or public value, opposition to such plans is likely.
4.4. The case for change: transparency of CCG decision-making
The above examples of negative public reactions to service change proposals in South London notwithstanding, interviewees largely agreed that transparency was necessary in order to make a case for change. A number of interviewees, however, expressed concerns over how statutory mandates for transparency function in practice. For example, they pointed out that the documents available on websites or in meetings are lengthy, difficult to understand or reached the audience too late in the decision-making process. There was also considerable concern about the language and the quantity of the information in the public domain, which makes it difficult for stakeholders and the public to know what is being proposed or decided, what the alternative options are and what is expected of them.
[…] the detail and that […] level of information [about priorities and service change], isn't always in the public domain where it needs to be, […] the documents […] talk about things in such generalities and in such anodyne language, that you can't not agree with them. But, at the same time, you have no idea what you'd be agreeing with, so you couldn't possibly agree with them. (Healthwatch manager 4)
In reality, a lot else happens [in the priority-setting process] and very little is actually put on there [the website]. […] putting minutes on a website […] [is] transparent in terms of you're not hiding anything […]. But actually, I feel […] to get proper engagement, too much information works like smoke and mirrors. It might not be intended but it's not accessible and you're actually blinding people […]. (Healthwatch manager 3)
Respondents agreed that CCGs put the minutes of meetings and strategic documents on their websites. However, the above excerpts suggest that what is put on the websites is often neither the content nor the format that would help stakeholders, the public and patients understand the reasons why decisions are made and how priorities are set. According to interviewees, strategic documents are presented in a high-level language with little insight into how and why decisions were taken.
5. Discussion
The findings reveal two important features of priority-setting at local level: (1) priority-setting takes place in the context of national reforms which can lead, aid or stifle prioritisation; (2) priority-setting happens against the backdrop of previous priority-setting or service reconfiguration efforts. The fact that current and past reforms are so crucial to what may or may not be feasible at the local level does not come as a surprise as scholarly work on health policy frequently points out that ongoing and ever new reforms are the default mode of health care systems (Fulop et al., Reference Fulop, Protopsaltis, King, Allen, Hutchings and Normand2005; Jones and Exworthy, Reference Jones and Exworthy2015). In other words, priority-setting does not operate in a historical or political vacuum. This creates challenges when it comes to meeting the principles of fair priority-setting enshrined in frameworks for the fair allocation of health resources. The principle of accountability, for example, requires decision-makers to give reasons for, and justify, one's decisions. As the findings section illustrated, however, reforms may lead to a situation where who is responsible or accountable for a decision is a topic of contention or confusion, thus making it difficult to uphold the principle of accountability. Similarly, the principle of transparency is at risk of being undermined by mistaking the publication of a large number of documents for the need to make information available in an accessible and understandable format and language.
In unravelling the complex interaction between health care reforms and priority-setting at a local level, it is helpful to consider the following aspects. First, health priority-setting at the local level is complex and messy; our study is not the first to illustrate this (see Reichenbach, Reference Reichenbach2002; Maluka et al., Reference Maluka, Kamuzora, San Sebastiån, Byskov, Olsen, Shayo, Ndawi and Hurtig2010; Robinson et al., Reference Robinson, Williams, Dickinson, Freeman and Rumbold2012). Second, reforms and priority-setting in health care have one important factor in common: They are aimed at bringing about change. Change in turn is likely to result in opposition. In other words, setting priorities in a fair and equitable manner is hard to do in the best of times; trying to do it against constant waves of new reforms is even harder, not least because every reform brings new directions that need to be integrated into local prioritisation plans. In an effort to make sense of these insights from our interview study, we looked to the health policy and political science literature.
5.1. Path dependency in health care and priority-setting
Many respondents talked about what they perceived as a contradiction between the HSCA 2012 aiming to give local health care planners more autonomy on the one hand, but the NHS Five Year Forward View curtailing this autonomy on the other. Giving local health commissioners more power required changing previous, more top-down, ways of working. Focusing on prevention and integration, however, meant working together to integrate different levels of health care planning. In an effort to support the latter, NHSE stipulated measures to support integration at local level. These stipulations were introduced almost simultaneously to CCGs constituting themselves as organisations, resulting in confusion about the extent to which CCGs were able to work autonomously. All of this happened when the purchaser–provider split was still a core feature of the NHS even though The King's Fund (2019) called the NHS’ Five Year Forward View a strategy that started to unravel it.
The debate about the advantages and disadvantages of central versus local-led health care systems is long-standing and one of most widely discussed topics in heath policy (e.g. Abel-Smith, Reference Abel-Smith1994; Blank and Burau, Reference Blank and Burau2004). Whether one or the other strategy is pursued, and whether it is successful, is usually a result of the structural features and historical trajectories of the health care system on the one hand, and the governing party's political agenda on the other. The importance of historical trajectories famously led Wilsford (Reference Wilsford1994) to conclude that health systems struggle to reform in a meaningful way because existing institutions and structures present obstacles to true reform. In other words, path dependency plays a role in what is or is not possible when attempting to reform health care systems.
The findings presented in this article indicate that path dependency also plays a role when setting priorities. Several of our respondents recalled examples of service overhauls that were stopped because politicians and members of the local community led successful campaigns against the proposed changes, which in turn made future reconfigurations less likely. Evaluated against A4R and DMAT principles, the examples met the standard criteria of fair priority-setting. For example, clinical and cost effectiveness studies presented a strong case for change. Decision-makers also engaged in consultation and other public involvement processes. Despite this, the proposed priorities were not implemented.
There are several ways to interpret this apparent failure in priority-setting. First, one could argue that decision-makers did not make a strong enough case for change. This, however, is difficult to prove post facto. Second, one could argue that it is not in fact a failure of priority-setting, but a success of setting priorities in a fair and procedurally sound process. The fact that the outcome of the process was not as intended by decision-makers is not a failure, but a sign that they were responsive to the political and participatory nuances in their area. This interpretation would suggest that frameworks for fair priority-setting should not be mistaken for frameworks that guarantee success for decision-makers. This is something that needs to be made more explicit when proposing frameworks for practice. Third, this apparent failure in local priority-setting demonstrates the importance of understanding local context and past historical trajectories. Understanding the local context helps to foresee likely opposition to, or even ‘no-go's’ in, priority-setting. It could help in building strategic alliances of support and in engaging with different community stakeholders earlier on in the process. The strength and passion of community campaigners is not something to underestimate, as illustrated in the findings section with one participant saying: ‘[…] we saved […] [the] hospital and therefore we're going to save it all. You know, […] nobody's going to do anything to [Name of London borough redacted to ensure confidentiality] ever again’ (CCG lay member 2).
5.2. The limits of transparency
Of all the principles of fair priority-setting included in the interview guide (see Methods section), several interviewees reflected upon transparency in much detail. They agreed that its complexity, but also its importance, was related to its two functions: (1) transparency as a key prerequisite for holding CCGs to account, (2) transparency as a precondition for putting changes into effect by ensuring that the public and patients are informed and involved. Concerns were raised about how transparency works in practice. Healthwatch representatives suggested that CCG documents are long, full of jargon and that the core of what is being decided, and why, is not easily discernible. This raises questions about the quality of transparency, suggesting that CCGs opt for quantity rather than quality of information. Making all documents and summaries of meetings available online binds time and staff resources, but its effectiveness is questionable if the audience cannot understand what has been decided and why. A lack of understanding for certain decisions might in turn lead to a situation in which local groups and campaigners oppose service reconfigurations, similar to the examples outlined in the findings section. Research has shown that PPI in priority-setting can and does often result in tokenistic rather than meaningful involvement attempts, but it has also shown that transparency, conceptualised as information presented in a format and language accessible to lay people, is key to improving PPI activities (Coultas et al., Reference Coultas, Kieslich and Littlejohns2019, Littlejohns et al., Reference Littlejohns, Kieslich, Weale, Tumilty, Richardson, Stokes, Gauld and Scuffham2019). As a principle of fair priority-setting, its importance cannot be emphasised enough because without it, principles of accountability and PPI are difficult to uphold.
That being said, the interviews also show that there are limits to transparency. Whilst its importance is undisputed, it does not guarantee that the public, patients and other stakeholders will accept prioritisation proposals. The examples of unsuccessful hospital ward closures or other service reconfigurations suggest that neither transparency nor a strong clinical case for change is a guarantor for change. One possible explanation for this is the phenomenon that people are likely to agree with a clinical case for change as long as it stays abstract, but that this agreement wanes when they realise that they, their community, or people close to them, are directly affected. This is sometimes referred to as the Not Out Of My Back Yard (NOOMBY) phenomenon, a play on words on the adverse public reactions to local wind farms often described as the Not in My Back Yard (NIMBY) phenomenon (Stewart and Aitken, Reference Stewart and Aitken2015). Research on this phenomenon has shown that reasons for opposing service changes are diverse and nuanced (Stewart, Reference Stewart2019). ‘Making the case’ thus needs to go beyond making a technical and transparent case, decision-makers must also engage in different participatory activities with members of the public and patients in order to understand the nuanced reasons for opposition (Stewart, Reference Stewart2019).
5.3. Implications for priority-setting frameworks
We found that commonly agreed upon principles of fair priority-setting such as transparency, accountability and patient and public involvement – in other words those principles firmly rooted in theories of procedural justice – were principles of which our interviewees were aware and about which they offered deeper reflections. As frameworks providing normative guidance and aiming to meet procedural criteria, the principles contained therein carry weight. Practically, however, the adherence to the principles is impeded by the difficulty of conceptualising and operationalising principles on the one hand, and the political and historical context on the other. The concerns about providing too much information in complex language, and too little information in an easily accessible and understandable format is an example of the difficulty to operationalise and act upon normative principles that are, in principle, undisputed. Such concerns are not new to priority-setting, but they are exacerbated in local contexts, and against the backdrop of ongoing health reforms and financial pressures.
The fact that interviewees referred to a lack of discretionary spending opportunities also offers interesting insights into priority-setting in practice. Whilst formal priority-setting frameworks have arguably been established to address precisely this problem of how to allocate limited resources, the reality of too many competing health needs and too little financial resources seems to lead decision-makers to not embark on the path of formal priority-setting. This suggests that an invisible (financial) threshold exists for when decision-makers believe that formal prioritisation processes are a worthy pursuit. It uncovers another flaw in the practicality of priority-setting frameworks for local decision-making: current frameworks assume that the person, group or entity setting priorities has a given budget, of which proportions can be allocated to services based on clinical, cost effectiveness or other considerations. The frameworks, however, do not provide insights into what decision-makers can or should do if the budgets are already allocated as a result of statutory or other commitments. Priority-setting frameworks are thus helpful as long as there are still at least some funds available; once all funds are spent on existing commitments it becomes cynical to talk about priority-setting as if this is something that local decision-makers can still do. This is not to suggest that frameworks for fair priority-setting are irrelevant, but that they are, at times, impractical.
5.4. Acknowledging politics and context in priority-setting at local level: a proposal
We propose a set of considerations to address the concern for impracticality, and to supplement current frameworks. The set of considerations (see Box 1) is based on insights from the political science and public policy literature about how and why change happens, including insights from the advocacy coalition framework (Sabatier, Reference Sabatier1988; Jenkins-Smith Sabatier, Reference Jenkins-Smith and Sabatier1994), principal–agent relationships, and path dependency in health policy (see previous discussion). The advocacy coalition framework suggests that change happens when different stakeholders form informal or formal coalitions to advocate for, and pursue change, based on shared values and ideas. Research shows that it can take several decades for coalitions to form and for change to come about (Sabatier, Reference Sabatier1988). This puts a rather stark perspective on efforts of local priority-setting, given they entail some form of change. That is not to say that every attempt at change is doomed to fail or that every prioritisation plan will take decades to realise, but it does explain why some proposals are not successful.
Box 1. Politics and context in priority-setting
Politics is the question of who gets what, when and how (Lasswell, Reference Lasswell1936). Identifying priorities in health care involves decisions about which regions, populations or patient groups get what level of access to health care services. A range of individuals, groups and institutions will seek to influence this process, for example, politicians, health care managers, health and social insurances companies (depending on the health system), professional associations, patient organisations or local campaign groups. These stakeholders will pursue their own agendas, and they will align with other groups if they can identify with their values and if it furthers their cause. In a given priority-setting process, it is therefore useful to ask:
• Which party currently holds power, and what are its priorities for health care?
• What are the current political alliances, both nationally and regionally?
• Who are the key individuals, groups or institutions that influence the decision-making process at the national or local level?
• What are some of the historic characteristics that define the area or region? Have there been public campaigns for or against changes in health care provision?
• Can a local or national leader who drives forward change be identified?
Another useful framework for thinking about priority-setting challenges at the local level is the principal–agent theory. In health politics, this theory means that an entity such as the government or a ministry for health (the principal) designates another entity such as GPs in CCGs (the agent) to implement a given set of health reforms or priorities. The crux of the principal–agent problem is that the room for manoeuvre is wide, and that agents will likely implement reforms in ways that fit their worldviews, or that they see fit for local context. This explains why change sometimes happens but has unforeseen consequences. In the case of the HSCA 2012 and the NHSE Five Year Forward View, there were many players, i.e. agents, in charge of implementing reforms, which led to fragmentation and confusion in the way reforms were implemented.
Based on the outlined insights, we propose a set of questions to consider when setting priorities at a local level, and when evaluating local decision-making processes (Box 1). These considerations are distinct from the considerations in the ‘institutional setting’ domain of some frameworks such as the DMAT. ‘Institutional setting’ focuses on the statutory duties of an organisation; political considerations are about identifying the relationships, networks, factors and politics that bear upon this role, and about the ability to bring about change. In other words, the institutional setting is about the laws and mandates that need to be followed, whereas the political considerations are about the people, groups and influences that shape them. It is therefore necessary to adjust frameworks such as the DMAT to incorporate questions of politics and context. The set of considerations we propose in Box 1 follow the format of the DMAT in that a description of the domain is followed by a set of questions; it thus serves as an example of what an inclusion of questions of context and politics might look like, but we envisage that this might alter slightly depending on the framework under review.
6. Conclusion
This article contributes to the empirical knowledge on priority-setting at the local level. It underlines that contextual factors such as the financial, reform, political and historical setting can lead, aid or stifle priority-setting processes. This can lead to a situation in which decision-makers are not able to pursue formal prioritisation strategies because contextual influences prevent them from doing so. At the time of the interviews, the HSCA 2012 and the NHS Five Year Forward View were still in the process of being implemented, leading to confusion about the roles of people and organisations; additionally, CCGs were faced with a budget reduction in real terms. This combination of factors creates a situation in which it is difficult to implement priority-setting strategies.
The HCA 2022 abolished CCGs; they have since been formally replaced by ICSs. Far from rendering the findings outdated, however, this recent reform underlines our argument that reforms are a constant feature of the English NHS (and of other health care systems). We conducted the interviews for this study in 2017 and 2018, nearly 6 years after CCGs were established. Our interview partners told us that they were still finding their places within the CCG structures, whilst simultaneously dealing with the ICS developments that were already underway. It is unlikely that CCG decision-makers and other stakeholders ever found themselves in a position to set priorities in a systematic and long-term fashion before the organisations they worked for were abolished, or at least morphed into ICSs. That is not to say that reforms should be avoided at all costs; some reforms such as the NHSE's workforce plan are of needed to ensure the future functioning of the NHS. Reforms, however, potentially have unintended consequences, especially when they are of a structural kind, that is when they aim to restructure organisations and responsibilities. This holds an important lesson for priority-setting: reforms disrupt the conditions for achieving ‘routine’ priority-setting and resource allocation in health care. This insight goes a long way in explaining why, more often than not, a prioritisation strategy that follows principles enshrined in some of the aforementioned frameworks for ethical priority-setting is a distant goal in local commissioning for health care.
In light of our findings, we propose a set of political and contextual considerations to supplement current priority-setting frameworks, and to make them more applicable to the local specificities of health resource allocation. In doing so, we sought out the literature on policy change in political science because by its nature priority-setting seeks to bring about change. For decision-makers, we hope that these considerations will help them identify fruitful avenues for collaboration and cooperation, and perhaps avoid some of the frustrations of being unsuccessful with one's plans. For researchers, we hope that these considerations will help to examine priority-setting in a more holistic fashion that acknowledges the role of politics and context.
We conclude with two important questions that the study raises for the research and practice of priority-setting: First, how should the ‘success’ of priority-setting be defined and measured? Second, what is the role of formal priority-setting in times of austerity? The first question is one that, in our view, the research community has not been explicit enough about. Frameworks for priority-setting such as A4R are based on procedural values, suggesting that priority-setting efforts are fair as long as fair and consistent procedures are followed. This normative assumption, however, seems to be at odds with the practical purpose of priority-setting, i.e. to help determine what is most important in the context of limited resources (Clark and Weale, Reference Clark and Weale2012). Several examples discussed in this article show that following priority-setting principles such as transparency and PPI did not result in the outcome that was perhaps desirable, or ‘most important’, on clinical or cost effectiveness grounds. This highlights the need to distinguish between different, nuanced, perceptions of value. The service that a community values may be different from the service that is most clinically and cost effective. It is crucial to recognise potential conflicts of value and values (Weale, Reference Weale1998), and to acknowledge that prioritisation has not necessarily failed if a decision for keeping certain services is made. In times of austerity and reduced health care budgets, however, decision-makers are expected to prioritise high value – in health economic terms – services at the expense of low value services. This creates an unresolved tension: the normative aspiration of priority-setting is met when processes are fair, whereas the practical aspiration is met when investment and disinvestment happen as a result of such processes, which in turn does not always align with the needs and values of the local community. At the very minimum, researchers and decision-makers must be open about this tension and the need for trade-offs it creates.
Acknowledgements
We thank the interview participants for taking the time to participate in the study. We thank the writing group of the Department of Political Science at the University of Vienna for their comments on a previous version of this article. The authors were supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care South London (NIHR CLAHRC South London) at King's College Hospital NHS Foundation Trust, and CC and PL were later supported by the National Institute for Health and Care Research, Applied Research Collaboration South London (NIHR ARC South London) at King's College Hospital NHS Foundation Trust. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Competing interests
None.



 Open access
Open access