



A 65-year-old man anticoagulated for atrial fibrillation and previous stroke presented with sudden deafness. Examination revealed normal fluent language, but he was deaf to intense sound. The computed tomography (CT) showed encephalomalacia in the left temporal lobe, and the multiphase CT angiogram revealed hypoperfusion in the superior right temporal lobe (Figure 1A) causing the acute deafness. Thrombectomy successfully recanalized the MCA branch occlusion (Figure 1B) with the return of the patient’s hearing. Magnetic resonance imaging (MRI) confirmed the acute infarct in the right Heschl’s gyrus (Figure 1C/D) and the chronic left transverse temporal gyrus infarct (Figure 1D). Sudden deafness is an uncommon, but treatable presentation of stroke. Reference Leussink, Andermann and Reiners1
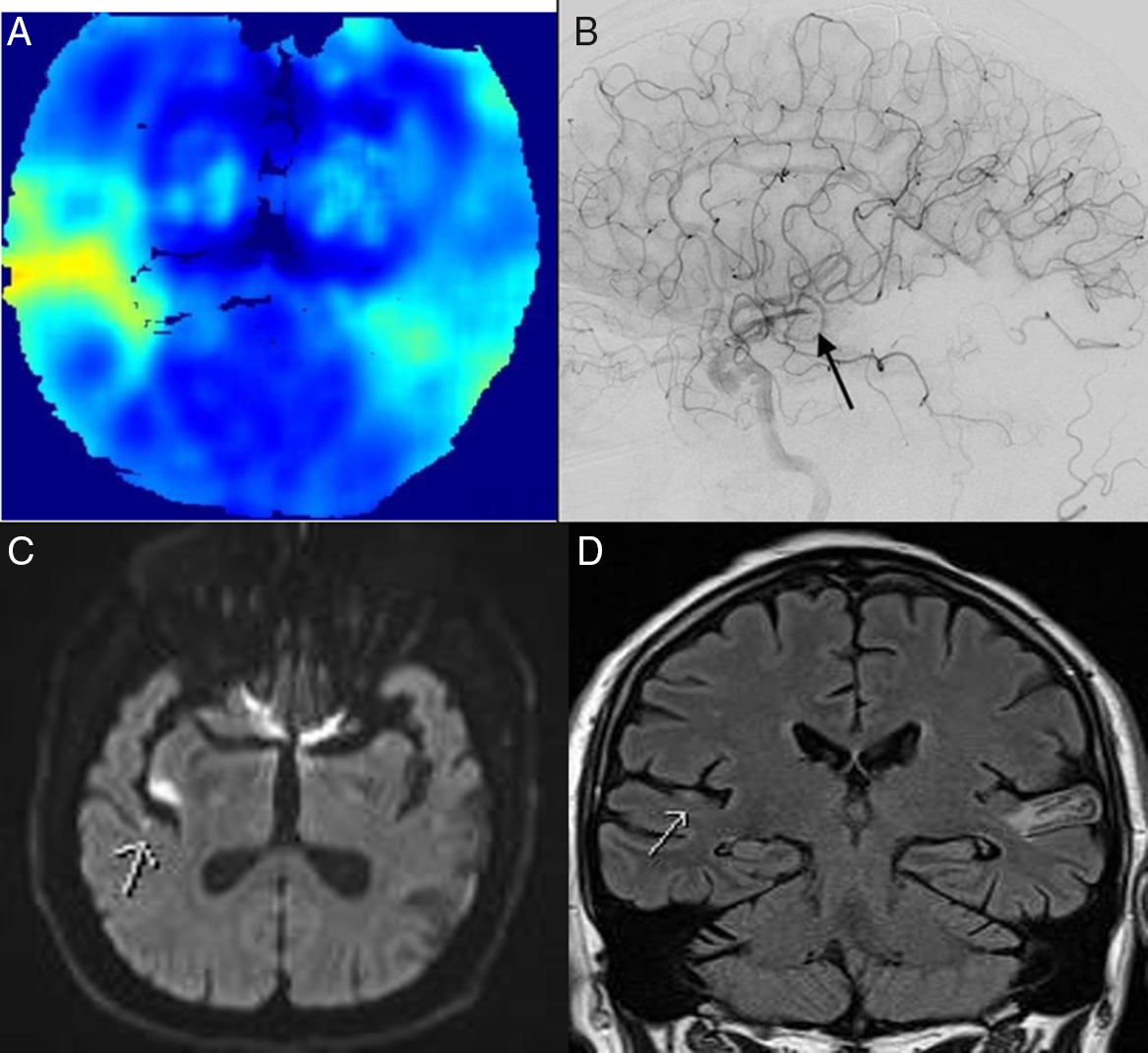
Figure 1: CTA perfusion image (SPIRAL)Reference McDougall, Chan and Sachan2 showing right superior temporal lobe hypoperfusion (A). Right internal carotid catheter angiogram (B) demonstrating right posterior M3 branch occlusion. Diffusion weighted image (C) showing small right transverse temporal gyrus acute infarct following thrombectomy. Coronal FLAIR MRI (D) demonstrating acute right temporal and chronic left contralateral infarcts.
Disclosures
The authors have no conflicts of interest to declare.
Statement of Authorship
REM: drafting and revision of manuscript. RAJ: data collections and interpretation; revision of manuscript. CDdE: data collection and interpretation. CCM: data collection and interpretation. WFM: revision for intellectual content; data collection. PAB: data collection; drafting and revision of manuscript.

