
5 results
Prescriptions patterns and appropriateness of usage of antibiotics in small and medium- sized hospitals in Korea
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s19
-
- Article
-
- You have access
- Open access
- Export citation
-
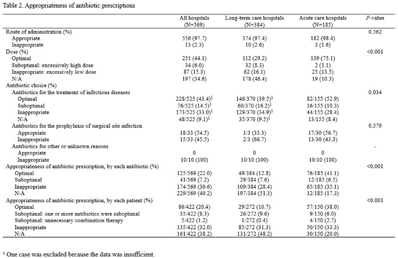
Background: Although small- and medium-sized hospitals comprise most healthcare providers in South Korea, data on antibiotic usage is limited in these facilities. We evaluated the pattern of antibiotic usage and its appropriateness in hospitals with <400 beds in South Korea. Methods: A multicenter retrospective study was conducted in 10 hospitals (6 long-term care hospitals, 3 acute-care hospitals, and 1 orthopedic hospital), with <400 beds in South Korea. We analyzed patterns of antibiotic prescription and their appropriateness in the participating hospitals. Data on the monthly antibiotic prescriptions and patient days for hospitalized patients were collected using electronic databases from each hospital. To avoid the effect of the COVID-19 pandemic, data were collected from January to December 2019. For the evaluation of the appropriateness of the prescription, 25 patients under antibiotic therapy were randomly selected at each hospital over 2 separate periods. Due to the heterogeneity of their characteristics, the orthopedics hospital was excluded from the analysis. The collected data were reviewed, and the appropriateness of antibiotic prescriptions was evaluated by 5 specialists in infectious diseases (adult and pediatric). Data from 2 hospitals were assigned to each specialist. The appropriateness of antibiotic prescriptions was evaluated from 3 aspects: route of administration, dose, and class. If the 3 aspects were ‘optimal,’ the prescription was considered ‘optimal.’ If only the route was ‘optimal,’ and the dose and/or class was ‘suboptimal,’ but not ‘inappropriate,’ it was considered ‘suboptimal.’ If even 1 aspect was ‘inappropriate,’ it was classified as ‘inappropriate.’ Results: The most commonly prescribed antibiotics in long-term care hospitals was fluoroquinolone, followed by β-lactam/β-lactamase inhibitor (antipseudomonal). In acute-care hospitals, these were third-generation cephalosporin, followed by first-generation cephalosporin and second-generation cephalosporin. The major antibiotics that were prescribed in the orthopedics hospital was first-generation cephalosporin. Only 2.3% of the antibiotics were administered inappropriately. In comparison, 15.3% of patients were prescribed an inappropriate dose. The proportion of inappropriate antibiotic prescriptions was 30.6% of the total antibiotic prescriptions. Conclusions: The antibiotic usage patterns vary between small- and medium-sized hospitals in South Korea. The proportion of inappropriate prescriptions exceeded 30% of the total antibiotic prescriptions.
Funding: None
Disclosures: None



The effect of a parenteral-to-oral conversion program for high-bioavailability antibiotics use
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s3-s4
-
- Article
-
- You have access
- Open access
- Export citation
-
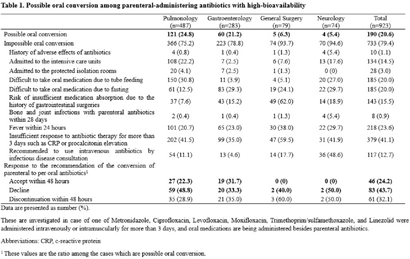
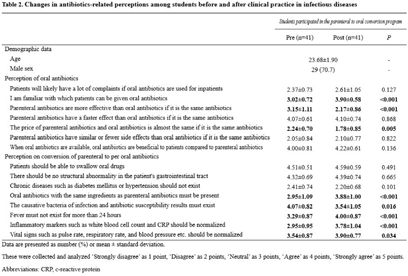
Background: Appropriate conversion of antibiotics from parenteral to the oral route can lower the risk of catheter-associated infections, reduce medical costs, and shorten hospitalization. We investigated the effect of a parenteral-to-oral conversion program on high-bioavailability antibiotics conducted by medical students and the changes in perceptions of oral antibiotics after participating in the program. Methods: The parenteral-to-oral conversion program was implemented as a core clinical practice course for the fifth-year medical students in 2021 at the infectious diseases department in an affiliated hospital of a medical school in Korea. Half of the students in this class participated in the program from January to October 2021. An evaluation of the possibility of oral conversion was performed for parenterally administered, high oral-bioavailability antibiotics including ciprofloxacin, levofloxacin, moxifloxacin, metronidazole, linezolid, and trimethoprim–sulfamethoxazole. These agents are prescribed in the departments of pulmonology, gastroenterology, general surgery, and neurology. The medical students reviewed medical records for the patients treated with those antibiotics and wrote a recommendation for oral conversion for the cases with “possible oral conversion” after an infectious disease specialist confirmed their assessments. The cases without administration of any oral drugs or with the duration of parenteral antibiotic use of <3 days were excluded from the evaluation. The following cases were considered as “impossible oral conversion” and were excluded from the intervention: (1) admitted to the ICUs, (2) admitted to the protected isolation rooms, (3) difficult to take oral medication, (4) risk of insufficient medication absorption, e) bone and joint infections, (5) fever within 24 hours, (6) insufficient response to antibiotic therapy, and (7) recommended to use intravenous antibiotics by consultation with an infectious disease specialist. Furthermore, a survey was conducted on the perception of oral antibiotics in medical students before and after clinical practice to evaluate the educational effect of this program. Results: In total, 923 cases were reviewed, and 190 (20.6%) of 923 antibiotics prescriptions with high oral bioavailability were found to be administered parenterally even though they could be converted oral administration. Among these 190 antibiotics prescriptions, 46 (24.2%) were changed via a written proposal within 48 hours, 83 (43.7%) proposed changes were declined, and 61 (32.1%) antibiotics prescriptions were discontinued within 48 hours. Through this program, students have gained a better perception of oral antibiotics. Conclusions: This parenteral-to-oral conversion program showed a 24.2% acceptance rate of oral antibiotics conversions in the hospital, and it had significant educational effects on medical students regarding an appropriate perception of oral antibiotics.
Funding: None
Disclosures: None


Differences in the Clinical Outcome of Community-Acquired APN According to the Appropriateness of Antibiotic Use
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s6
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The purpose of this study was to find out the relationship between appropriateness of antibiotic prescription and clinical outcomes in patients with community-acquired acute pyelonephritis (CA-APN). Methods: A multicenter prospective cohort study was performed in 8 Korean hospitals from September 2017 to August 2018. All hospitalized patients aged ≥19 years diagnosed with CA-APN at admission were recruited. Pregnant women and patients with insufficient data were excluded. In addition, patients with prolonged hospitalization due to medical problems that were not associated with APN treatment were excluded. The appropriateness of empirical and definitive antibiotics was divided into “optimal,” “suboptimal,” and “inappropriate,” and optimal and suboptimal were regarded as appropriate antibiotic use. The standard for the classification of empirical antibiotics was defined reflecting the Korean national guideline for the antibiotic use in urinary tract infection 2018. The standards for the classification of definitive antibiotics were defined according to the result of in vitro susceptibility tests of causative organisms. Clinical outcomes including clinical failure (mortality or recurrence) rate, hospitalization days, and medical costs were compared between patients who were prescribed antibiotics appropriately and those who were prescribed them inappropriately. Results: In total, 397 and 318 patients were eligible for the analysis of the appropriateness of empirical and definitive antibiotics, respectively. Of these, 10 (2.5%) and 18 (5.7%) were inappropriately prescribed empirical and definitive antibiotics, respectively, and 28 (8.8%) were prescribed either empirical or definitive antibiotics inappropriately. Patients who were prescribed empirical antibiotics appropriately showed a lower mortality rate (0 vs 10%; P = .025), shorter hospitalization days (9 vs 12.5 days; P = .014), and lower medical costs (US$2,333 vs US$4,531; P = .007) compared to those who were prescribed empirical antibiotics “inappropriately.” In comparison, we detected no significant differences in clinical outcomes between patients who were prescribed definitive antibiotics appropriately and those who were prescribed definitive antibiotics inappropriately. Patients who were prescribed both empirical and definitive antibiotics appropriately showed a lower clinical failure rate (0.3 vs 7.1%; P = .021) and shorter hospitalization days (9 vs 10.5 days; P = .041) compared to those who were prescribed either empirical or definitive antibiotics inappropriately. Conclusions: Appropriate use of antibiotics leads patients with CA-APN to better clinical outcomes including fewer hospitalization days and lower medical costs.
Funding: No
Disclosures: None
Table 1. 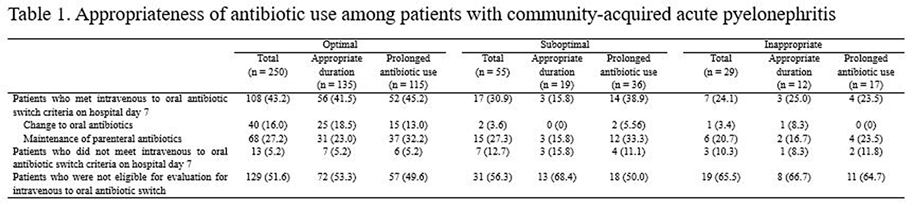
Table 2. 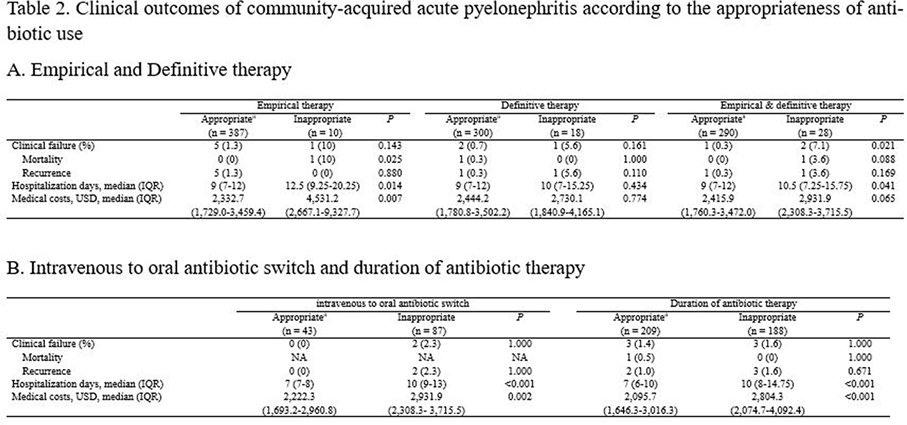


How Does Antimicrobial Resistance Increase Medical Costs in Community-Acquired Acute Pyelonephritis?
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s23
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: The proportion of antimicrobial-resistant Enterobacterales that are causative pathogens for community-acquired acute pyelonephritis (CA-APN) has been increasing. We examined the effect of antimicrobial resistance on medical costs in CA-APN. Methods: A single-center retrospective cohort study was conducted at a tertiary-care hospital in Korea between January 2018 to December 2019. All hospitalized patients aged ≥19 years who were diagnosed with CA-APN were recruited, and those with Enterobacterales as a causative pathogen were included. Comparisons between CA-APN caused by extended-spectrum β-lactamase (ESBL)–producing pathogens (ESBL+ group) and those by non–ESBL-producing organisms (ESBL– group) as well as CA-APN caused by ciprofloxacin-resistant pathogens (CIP-R group) and those by ciprofloxacin-sensitive pathogens (CIP-S group) were performed. Log-linear regression was performed to determine the risk factors for medical costs. Results: In total, 241 patients were included in this study. Of these, 75 (31.1%) had an ESBL-producing pathogen and 87 (36.1%) had a ciprofloxacin-resistant pathogen. The overall medical costs were significantly higher in the ESBL+ group compared with the ESBL− group (US$3,730.18 vs US$3,119.32) P <0.001) as well as in CIP-R group compared with CIP-S group (3,730.18 USD vs. 3,119.32 USD, P =0.005). In addition, length of stay was longer in ESBL+ group compared with ESBL-group (11 vs. 8 days, P <0.001) as well as in CIP-R group compared with CIP-S group (11 vs. 8 days, P <0.001). There were no significant difference in the proportion of clinical failure between ESBL+ and ESBL- groups; CIP-R and CIP-S groups. Based on the log-linear regression model, the costs associated with ESBL-producing Enterobacterales as the causative pathogen would be, on average, 27% higher or US$1,211 higher than its counterpart (P = .026). By the same token, a patient who is a year older would incur US$23 higher cost (P = .040). Having any structural problem in urinary tract would incur US$1,231 higher cost (P = .015). A unit increase in Pitt score would incur US$767 USD higher cost (P < 0.001) higher cost, all other things constant. Conclusions: Medical costs for hospitalized patients with CA-APN are increased by the existence of ESBL-producing Enterobacterales but not by the existence of ciprofloxacin-resistant Enterobacterales.
Funding: No
Disclosures: None
Figure 1.
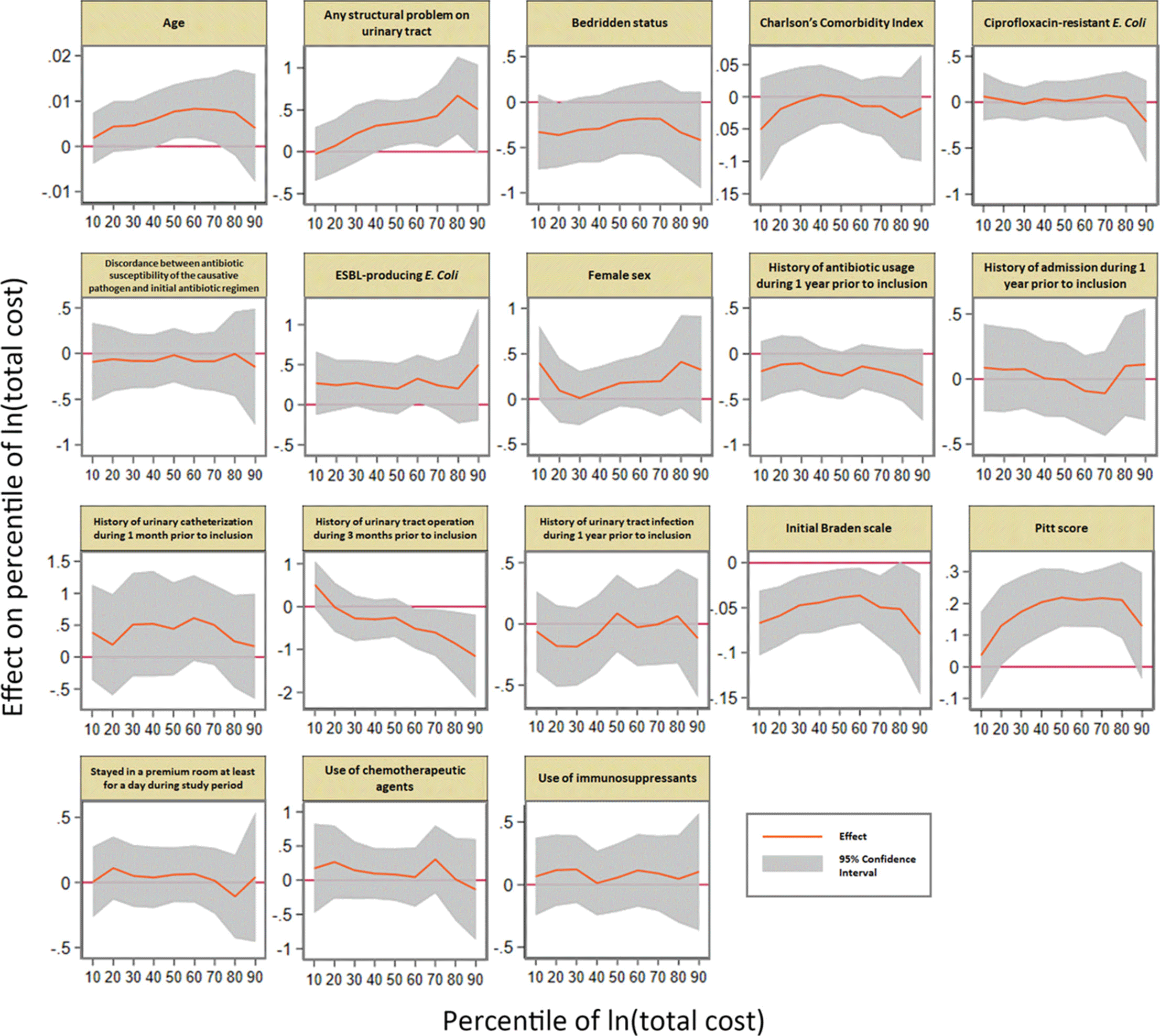
Table 1. 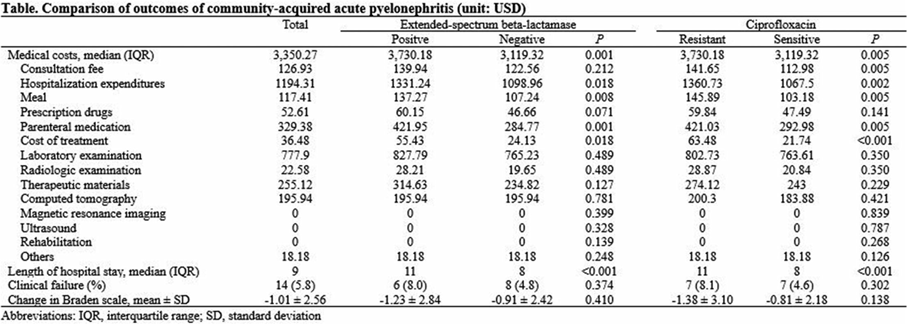
Table 2. 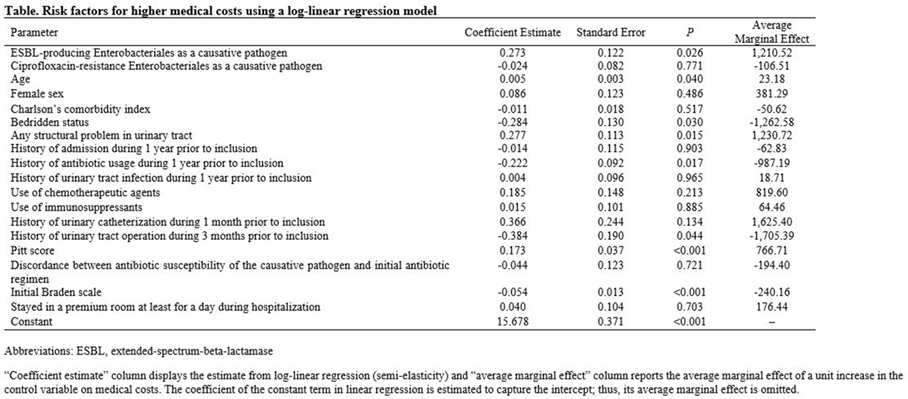



Human resources required for antimicrobial stewardship activities for hospitalized patients in Korea
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 12 / December 2020
- Published online by Cambridge University Press:
- 26 October 2020, pp. 1429-1435
- Print publication:
- December 2020
-
- Article
- Export citation
