
4 results
Relevance of RSV in hospitalized adults and the need for continued testing
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s62
-
- Article
-
- You have access
- Open access
- Export citation
-
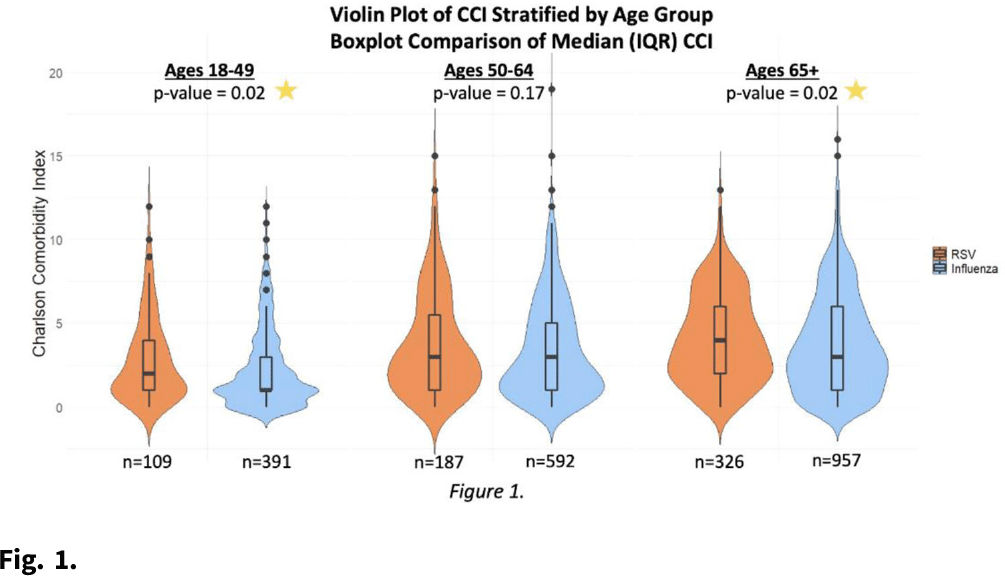
Background: RSV is underrecognized in hospitalized adults. A better understanding of RSV in this population could help prioritize targeted viral-testing resources. Hospitalization and in-hospital outcomes are widely accepted as markers of clinical severity with respect to acute respiratory illness (ARI). We compared characteristics and clinical outcomes between adults hospitalized with ARI from October 2016 through May 2019. Methods: All hospitalized adults (≥ 18 years) who met a standardized case definition of ARI were prospectively enrolled across 3 respiratory seasons from 9 hospitals participating in the US Hospitalized Adult Influenza Vaccine Effectiveness Network (HAIVEN). Demographic data were collected during enrollment interviews, and electronic medical records (EMRs) were reviewed to extract comorbidity data. Throat and nasal swabs collected at enrollment were tested for ARI pathogens using real-time PCR assays at respective HAIVEN research laboratory sites. Characteristics and clinical outcomes of participants were compared using χ2 or nonparametric tests where appropriate. Multivariable logistic regression models were used to test associations between infection status, characteristics, and clinical outcomes, adjusting for age, sex, race, Charlson comorbidity index (CCI), body mass index (BMI), site, season, and days to admission. Results: In total, 10,311 adults were included, 22.3% (n = 2,300) were aged 18–49 years, 33.2% (n = 3,423) were aged 50–64 years, and 44.5% (n = 4,588) were aged ≥65 years. Moreover, 6% of adults tested positive for RSV (n = 622), 18.8% positive for influenza (n = 1,940), and 75.1% negative for both (n = 7,749). Obesity and age ≥65 years were significantly associated with RSV detection when compared with participants negative for both RSV and influenza. Patients aged 18–49 years and ≥65 years with RSV had significantly higher median CCI scores compared to patients with influenza (Fig. 1.). The proportion of adults with CHF or COPD was significantly (p-value Conclusions: Severe RSV illness may differ from severe influenza illness, and those infected with RSV may have different characteristics than those infected with influenza. Hospitalized adults with RSV infection were more likely to have underlying cardiopulmonary comorbidities and higher CCI scores as well as experience an extended length of hospital stay and need for mechanical ventilation. These data highlight the importance of retaining testing for RSV in older adults hospitalized with ARI.
Funding: None
Disclosures: None

Economic Evaluation of Standing Order Programs for Pneumococcal Vaccination of Hospitalized Elderly Patients
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 29 / Issue 5 / May 2008
- Published online by Cambridge University Press:
- 02 January 2015, pp. 385-394
- Print publication:
- May 2008
-
- Article
- Export citation
Overcoming Barriers to Establishing an Inpatient Vaccination Program for Pneumococcus Using Standing Orders
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 26 / Issue 11 / November 2005
- Published online by Cambridge University Press:
- 21 June 2016, pp. 874-881
- Print publication:
- November 2005
-
- Article
- Export citation
Increasing Pneumococcal Vaccination Rates Among Hospitalized Patients
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 24 / Issue 7 / July 2003
- Published online by Cambridge University Press:
- 02 January 2015, pp. 526-531
- Print publication:
- July 2003
-
- Article
- Export citation
