
17 results
Identifying the relationship between hospital rurality and antibiotic overuse
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s34-s35
-
- Article
-
- You have access
- Open access
- Export citation
-
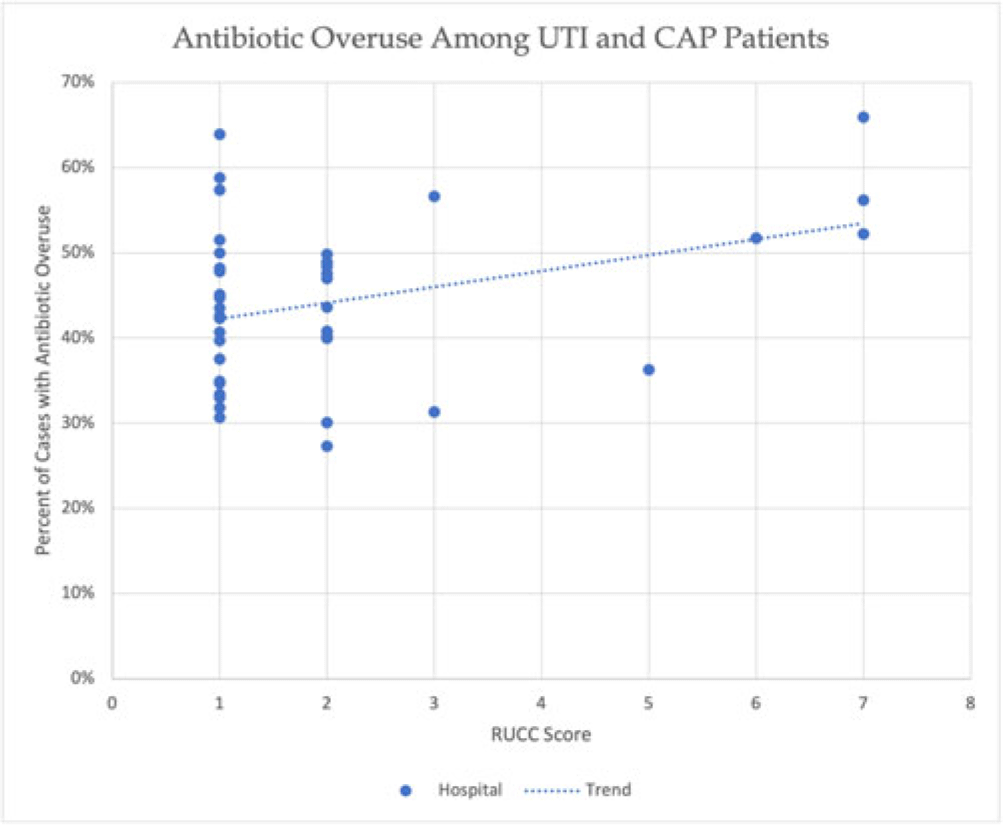
Background: Antibiotic overuse and the resulting patient outcomes span all hospitals. However, although antibiotic stewardship can improve antibiotic use, effective stewardship programs require expertise and an infrastructure that are not present in all hospitals. Rural hospitals have less access to resources, infectious disease expertise, and participation in academic research. Thus, we compared antibiotic overuse at discharge between rural and nonrural hospitals for patients diagnosed with community-associated pneumonia (CAP) or urinary tract infection (UTI)—the 2 most common hospital infections. Methods: To determine whether antibiotic overuse at discharge was higher among rural versus nonrural hospitals, we analyzed data from a 41-hospital prospective cohort of patients treated for CAP or UTI between July 1, 2017, and July 30, 2019, in Michigan. Antibiotic overuse was defined as treatment that was unnecessary (ie, patient did not have an infection), excessive (ie, duration >4 days for CAP), or included suboptimal fluoroquinolone use (ie, safer alternative available). Overuse was determined based on patient risk factors, symptoms, allergies, diagnostic results, and time to stability. Hospital rurality was defined using the Rural–Urban Continuum Codes (RUCC) score. We defined rural as a score ≥4 and very rural as a score of 7–9. We used t tests to compare the mean percentage of patients with antibiotic overuse at discharge between nonrural and rural (and very rural) hospitals. Results: Across 41 hospitals, we included 23,449 patients with CAP or UTI. There were 5 rural (and 3 very rural) hospitals with 2,039 (and 1,082) patients. Antibiotic overuse at discharge was present in 43.1% of patient cases in nonrural hospitals, 52.5% in rural hospitals (P = .04 vs nonrural) and 58.1% in very rural hospitals (P = .007 vs nonrural). Compared to nonrural hospitals, the mean percentage of cases with antibiotic overuse at discharge in rural hospitals was 9.4% higher (15.1% higher in very rural hospitals). Results were similar in a subgroup analysis of only patients with UTI (47.0% in rural vs 37.5% in nonrural, mean difference, 9.5%; P = .03) but were not statistically significant in patients with CAP (53.8% vs 48.0%, respectively; mean difference, 5.8%; P = 0.23). Conclusions: In this retrospective study, rural hospitals—especially very rural hospitals, had higher rates of antibiotic overuse at discharge than nonrural hospitals. Our findings suggest that antibiotic stewardship interventions tailored toward the unique differences in infrastructure, resources, and needs of rural hospitals are essential to community health.
Disclosures: None

Three-day antibiotic duration in patients with pneumonia: A sixty-eight–hospital cohort
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s22
-
- Article
-
- You have access
- Open access
- Export citation
-
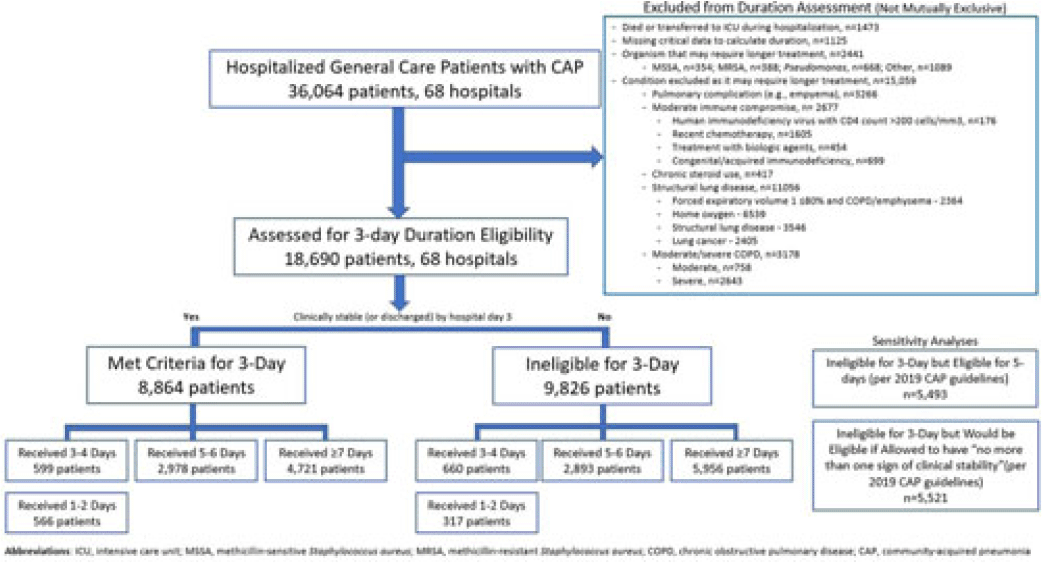
Background: Since 2019, community-acquired pneumonia (CAP) guidelines have recommended hospitalized patients be treated until clinical “stability and for no less than 5 days.” However, randomized trials have reported that, in patients who stabilize by hospital day 3, very short antibiotic durations (eg, 3 days) are noninferior to longer durations. How these trial results relate to real-world practice is unknown. Methods: Using a 68-hospital cohort study of hospitalized, general-care adults with CAP, we aimed to (1) quantify the percentage of patients who—according to trial criteria—qualify for a 3-day antibiotic duration, (2) quantify the percentage who actually received a 3-day duration, and (3) assess 30-day outcomes. Patients were considered to have CAP if they had a pneumonia discharge diagnosis and met clinical criteria for CAP. Patients with concomitant infections (including COVID-19), admission to intensive care, or severe immunocompromise were not included. Results: Between February 23, 2017, and August 3, 2022, 36,064 patients with CAP were included. Of those, 48.2% (9,826 of 36,064) were excluded due to a condition or organism ineligible for the 3-day treatment (Fig. 1). Of the 18,690 patients remaining, 52.6% (9,826) were unstable on day 3 and thus were ineligible for the 3-day treatment. Therefore, of all 36,064 patients, only 8,864 (24.6%) would be eligible under trial criteria for a 3-day treatment. Notably, 5,493 (55.9%) of 9,826 patients unstable on day 3 would be eligible for 5 days of treatment under national guidelines. In practice, use of 3–4-day treatment was rare, occurring in 599 (6.8%) of 8,864 patients eligible for a 3-day treatment versus 660 (6.7%) of 9,826 patients unstable on day 3 (P = .945). Use of 3–4-day treatment increased over time and comorbidities that could mimic CAP or a negative procalcitonin were more common in patients who received a 3–4-day treatment whereas specific symptoms of CAP were less common (Fig. 2). After adjustments, patients eligible for a 3-day duration who received a 3–4 day treatment versus a ≥5-day treatment had higher 30-day mortality (aOR, 1.87; 95% CI, 1.32–2.64) and readmission (aOR, 1.35; 95% CI, 1.17–1.56). Conclusions: Across 68 hospitals, <25% of patients hospitalized with CAP would be eligible for a 3-day antibiotic treatment. Though increasing over time, there was little use of 3–4-day treatments and, when prescribed, outcomes were worse, potentially due to CAP misdiagnosis. Given the small number of patients eligible for 3-day treatment, and the potential harm with too-short durations, it may be prudent to focus on increasing the use of 5-day treatments.
Disclosures: None

Prevalence of and risk factors for bacteremic UTIs in hospitalized adults without definitive signs or symptoms of UTI
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s27-s28
-
- Article
-
- You have access
- Open access
- Export citation
-
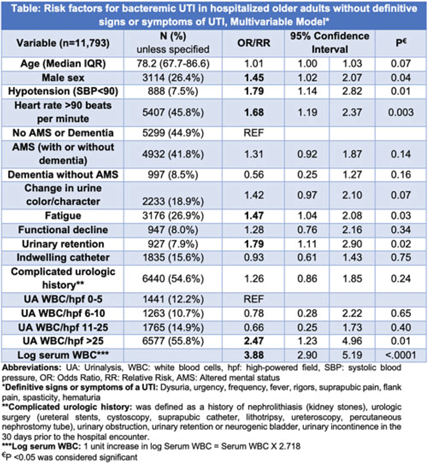
Background: IDSA guidelines recommend withholding treatment in patients with asymptomatic bacteriuria in the absence of systemic signs of infection. However, some patients with bacteriuria may not be able to express symptoms either due to presence of indwelling catheter, underlying complicated urologic anatomy, dementia, or altered mental status (AMS). Clinicians frequently treat bacteriuria in this population with antimicrobial therapy due to concern for sepsis. To determine treatment need, we aimed to review prevalence and risk factors for bacteremic urinary tract infection (UTI) in a cohort of hospitalized inpatients without definitive signs and symptoms of a UTI. Methods: This retrospective cohort study of inpatients with a positive urine culture who presented without definitive signs or symptoms of a UTI was conducted between July 1, 2017, and June 30, 2022, in 68 academic and community hospitals (Michigan Hospital Medicine Safety Consortium). Signs and symptoms were obtained from medical record review 3 days before and after urine-culture collection. Bacteremic UTI was defined as any positive blood culture growing at least 1 organism matching the urine culture. Risk factors for bacteremic UTI were assessed using multivariable logistic regression models with results expressed as odds ratios (ORs) for dichotomous variables and relative risks (RRs) for continuous variables. Results: Of 11,793 patients meeting study criteria, 73.6% were female with a median age of 78.2 years. Overall, 41.8% had AMS, 33.8% had dementia, 15.6% had an indwelling urinary catheter, and 54.6% had complicated urologic history (eg, urologic surgery). Of these, 166 patients (1.4%) developed bacteremic UTI. On adjusted analysis, male sex, hypotension, heart rate >90, urinary retention, fatigue, log of serum leukocytosis [1 log increase in serum WBC = 2.718 × serum white blood cell count (WBC)], and pyuria with >25 WBC per high-powered field (WBC/hpf) on urinalysis were associated with bacteremic UTI (Table). Older age, presence of an indwelling catheter, complicated urologic history, functional decline, AMS, dementia, and change in urine were not associated with higher odds for bacteremic UTI (Table). Of patients with AMS and no definitive signs or symptoms of a UTI, only 89 (1.8%) of 4,932 developed a bacteremic UTI. Conclusions: Bacteremic UTI is relatively rare in hospitalized inpatients presenting with bacteriuria without symptoms of UTI. Predictors of bacteremic UTI included male sex, hypotension, tachycardia, urinary retention, fatigue, serum leukocytosis, and higher levels of pyuria (>25 WBC/hpf) on urinalysis. Our findings provide stewards a framework to risk stratify inpatients of older age who present with positive urine cultures but without (or are unable to express) signs or symptoms of UTI.
Disclosures: None

Risk Factors and outcomes associated with inappropriate empiric broad-spectrum antibiotic use in hospitalized patients with community-acquired pneumonia
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s31-s32
-
- Article
-
- You have access
- Open access
- Export citation
-
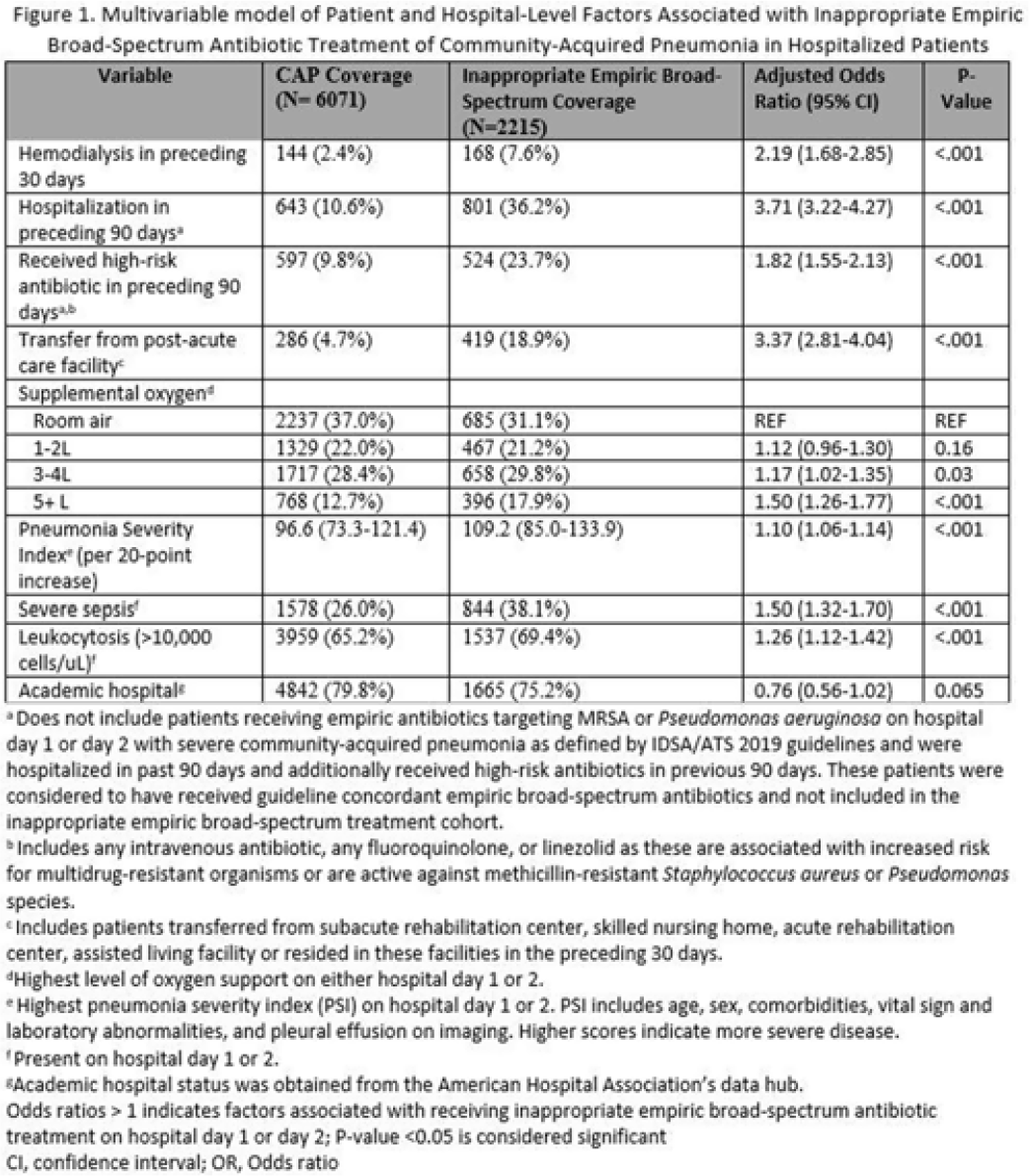
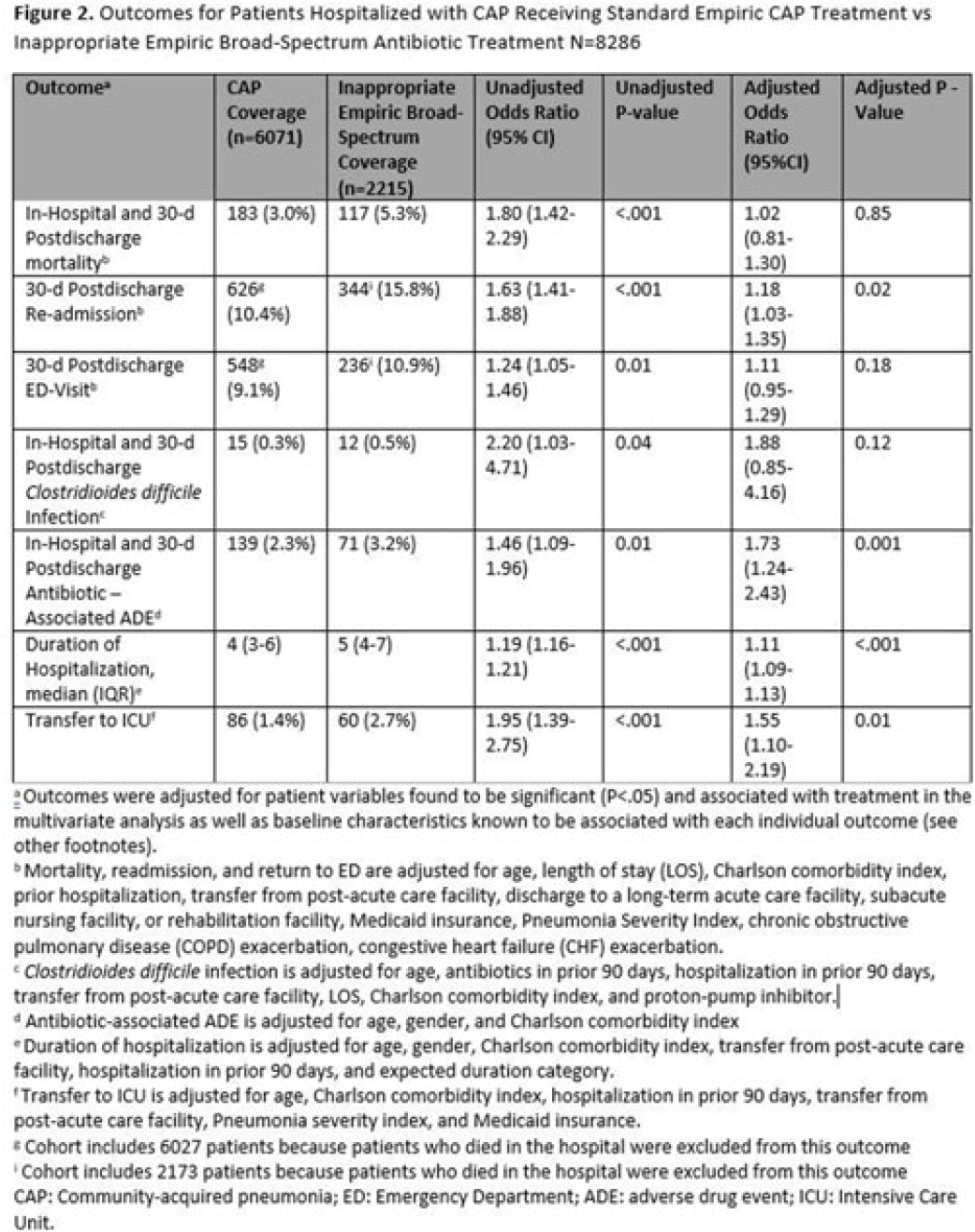
Background: Inappropriate broad-spectrum antibiotic use targeting methicillin-resistant Staphylococcus aureus (MRSA) and Pseudomonas aeruginosa can result in increased adverse events, antibiotic resistance, and Clostridioides difficile infection. In 2019, revised ATS/IDSA community-acquired pneumonia (CAP) guidelines removed healthcare-associated pneumonia (HCAP) as a clinical entity and modified patient factors warranting empiric broad-spectrum antibiotic (BSA) use. As a result, most patients hospitalized with CAP should receive empiric antibiotics targeting standard CAP pathogens. Based on revised guidelines, we evaluated predictors and outcomes associated with inappropriate BSA use among hospitalized patients with CAP. Methods: Between November 2019 and July 2022, trained abstractors collected data on non-ICU adult medical patients admitted with CAP at 67 Michigan hospitals who received either an inappropriate empiric BSA on hospital day 1 or 2 or a standard CAP regimen. Inappropriate empiric BSA use was defined as use of an anti-MRSA or anti-pseudomonal antibiotic in a patient eligible for standard CAP coverage per IDSA guidelines. Patients with immune compromise, moderate or severe chronic obstructive pulmonary disease (COPD), pulmonary complication, or guideline-concordant treatment with BSA were excluded. Data collected included comorbidities, antibiotic use and hospitalizations in the preceding 90 days, cultures in the preceding year, signs or symptoms of pneumonia, hospital characteristics, and 30-day postdischarge patient outcomes. Data were collected through chart review and patient phone calls. Predictors of inappropriate empiric BSA were evaluated using logistic general estimating equation (GEE) models, accounting for hospital-level clustering. We assessed the effect of inappropriate empiric BSA (vs standard CAP therapy) on 30-day patient outcomes using logistic GEE models controlling for predictors associated with the outcome and probability of treatment. Results: Of 8,286 included patients with CAP, 2,215 (26.7%) were empirically treated with inappropriate BSA. The median BSA treatment was 3 days (IQR, 2.5). After adjustments, factors associated with inappropriate empiric BSA treatment included hospitalization or treatment with high-risk antibiotics in preceding 90 days, transfer from a postacute care facility, hemodialysis, support with ≥3 L supplemental oxygen, severe sepsis, leukocytosis, and higher pneumonia severity index (Fig. 1). After adjustments, patients with inappropriate empiric BSA treatment had higher readmissions 30 days after discharge, more transfers to the intensive care unit, more antibiotic-associated adverse events, and longer hospitalizations (Fig. 2). Conclusions: Patients hospitalized with CAP often received inappropriate BSA as empiric coverage, and this inappropriate antibiotic selection was associated with worse patient outcomes. To improve patient outcomes, stewardship efforts should focus on reducing inappropriate BSA use in patients hospitalized for CAP with historic HCAP risk factors or severe CAP without other guideline-directed indications for BSA.
Financial support. H.M.S. initiative is underwritten by Blue Cross and Blue Shield of Michigan.
Disclosures: None


Pharmacist gender and physician acceptance of antibiotic stewardship recommendations: An analysis of the reducing overuse of antibiotics at discharge home intervention
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 4 / April 2023
- Published online by Cambridge University Press:
- 07 June 2022, pp. 570-577
- Print publication:
- April 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The effect of gender bias on acceptance of antibiotic stewardship recommendations by clinical pharmacists
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s67-s68
-
- Article
-
- You have access
- Open access
- Export citation
-
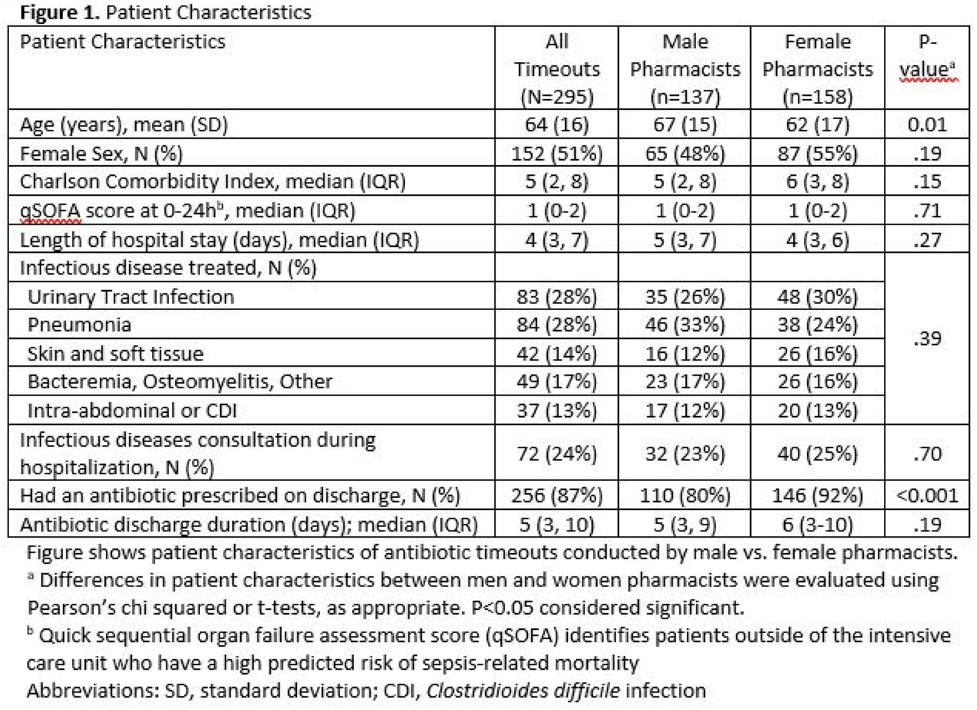
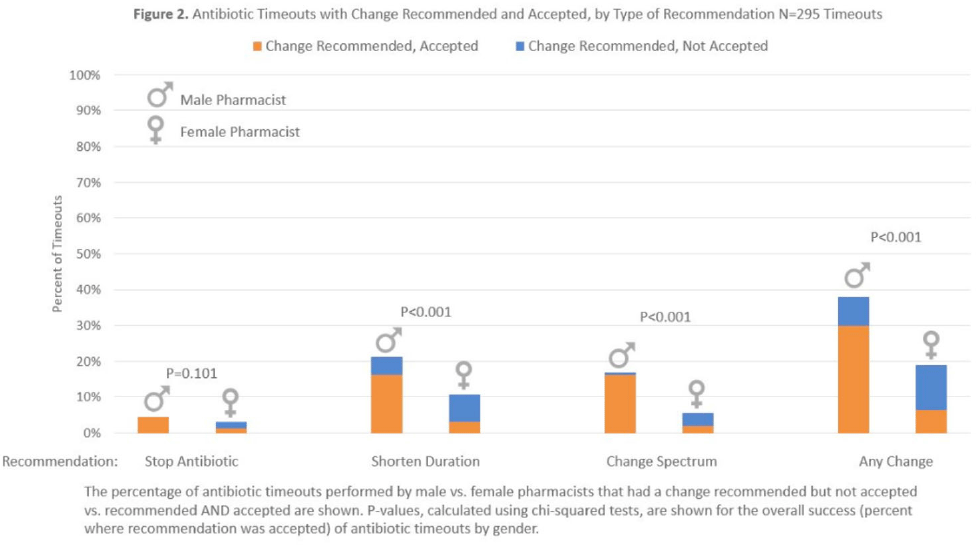
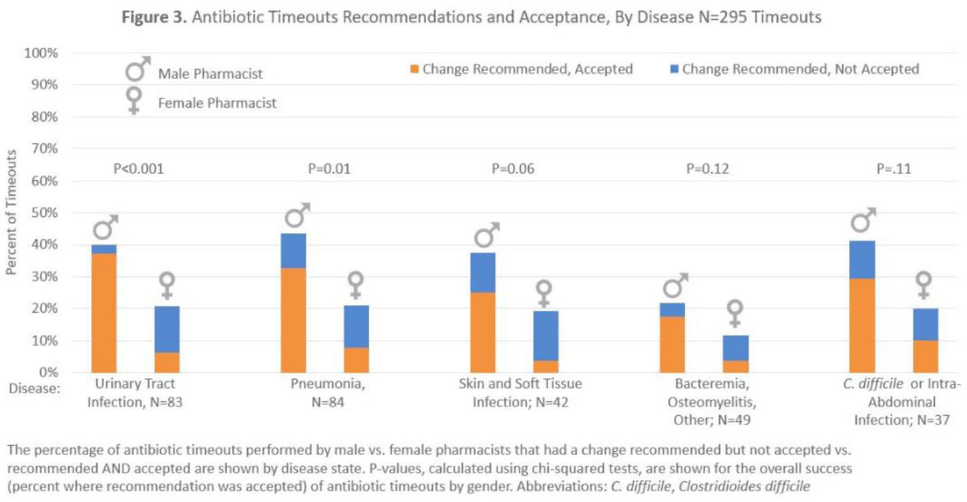
Background: Clinical pharmacists are a critical part of antibiotic stewardship. Stewardship often relies on relationships and persuasion, which may be affected by gender bias. Thus, we aimed to assess the association of sex with the acceptance of antibiotic stewardship recommendations. Methods: Between May and October 2019, medicine pharmacists at single hospital reviewed patients on antibiotics and–when a discharge was anticipated–led an antibiotic discussion (or “timeout”) prior to discharge. To explore differences in antibiotic timeout effectiveness by gender, we assessed the association of pharmacist sex with suggestion and acceptance of antibiotic changes using logistic regression controlling for patient characteristics. We also assessed whether hospitalist sex was associated with or moderated the effect of pharmacist sex on acceptance of timeout recommendations. Results: Between May 1, 2019, and October 31, 2019, pharmacists conducted 295 timeouts (patient characteristics in Fig. 1). Overall, 54% of timeouts were conducted by 12 female pharmacists and the remaining 46% were conducted by 8 male pharmacists. Overall, 82 (29%) of 295 timeouts resulted in a pharmacist recommending an antibiotic change, and male pharmacists were more likely to recommend a change: 52 (38%) of 137 versus 30 (19%) 158 (P Conclusions: In this discharge antibiotic intervention, timeouts conducted by women were less likely to result in an antibiotic change than those conducted by men. The difference in effectiveness resulted both from female pharmacists being less likely to recommend a change and from hospitalists being less likely to accept recommendations from a female pharmacist. These findings suggest that gender bias may play a role acceptance of antibiotic stewardship recommendations, which could affect antibiotic use, pharmacist job satisfaction, and patient outcomes.
Funding: None
Disclosures: None



Risk of bacterial bloodstream infection does not vary by central-line type during neutropenic periods in pediatric acute myeloid leukemia
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 2 / February 2023
- Published online by Cambridge University Press:
- 25 April 2022, pp. 222-229
- Print publication:
- February 2023
-
- Article
- Export citation
Duties, resources, and burnout of antibiotic stewards during the coronavirus disease 2019 (COVID-19) pandemic
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 05 November 2021, e39
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Antibiotic overuse after discharge from medical short-stay units
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 11 / November 2022
- Published online by Cambridge University Press:
- 24 August 2021, pp. 1689-1692
- Print publication:
- November 2022
-
- Article
- Export citation
Do antimicrobial and antithrombogenic peripherally inserted central catheter (PICC) materials prevent catheter complications? An analysis of 42,562 hospitalized medical patients
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 4 / April 2022
- Published online by Cambridge University Press:
- 28 April 2021, pp. 427-434
- Print publication:
- April 2022
-
- Article
- Export citation
Influence of Infectious Disease Physician Approval on Appropriateness of PICC Use and Outcomes
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s485-s487
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Misdiagnosis of Urinary Tract Infection Linked to Misdiagnosis of Pneumonia: A Multihospital Cohort Study
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s488-s489
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Home Health Service Provision After Hurricane Harvey
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 14 / Issue 1 / February 2020
- Published online by Cambridge University Press:
- 20 June 2019, pp. 56-62
-
- Article
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Philosophy
- Published online:
- 05 August 2015
- Print publication:
- 27 April 2015, pp ix-xxx
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- Clinical Gynecology
- Published online:
- 05 April 2015
- Print publication:
- 23 April 2015, pp viii-xiv
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- Neuropathic Pain
- Published online:
- 05 December 2013
- Print publication:
- 07 November 2013, pp vii-x
-
- Chapter
- Export citation
Use of vitamin D supplements during infancy in an international feeding trial
-
- Journal:
- Public Health Nutrition / Volume 17 / Issue 4 / April 2014
- Published online by Cambridge University Press:
- 24 June 2013, pp. 810-822
-
- Article
-
- You have access
- HTML
- Export citation
