
15 results
Mixed-methods process evaluation of a respiratory-culture diagnostic stewardship intervention
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 2 / February 2023
- Published online by Cambridge University Press:
- 03 January 2023, pp. 191-199
- Print publication:
- February 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Characteristics of healthcare personnel who reported concerns related to PPE use during care of COVID-19 patients
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s8-s9
-
- Article
-
- You have access
- Open access
- Export citation
-
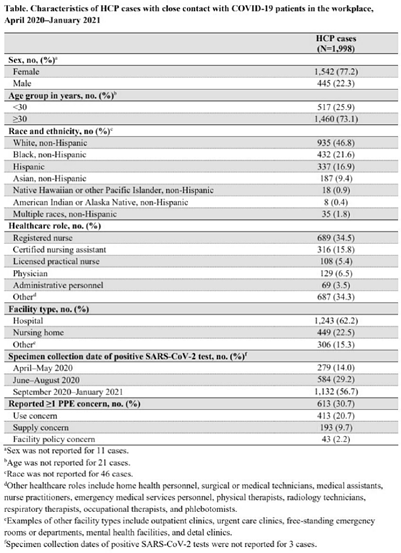
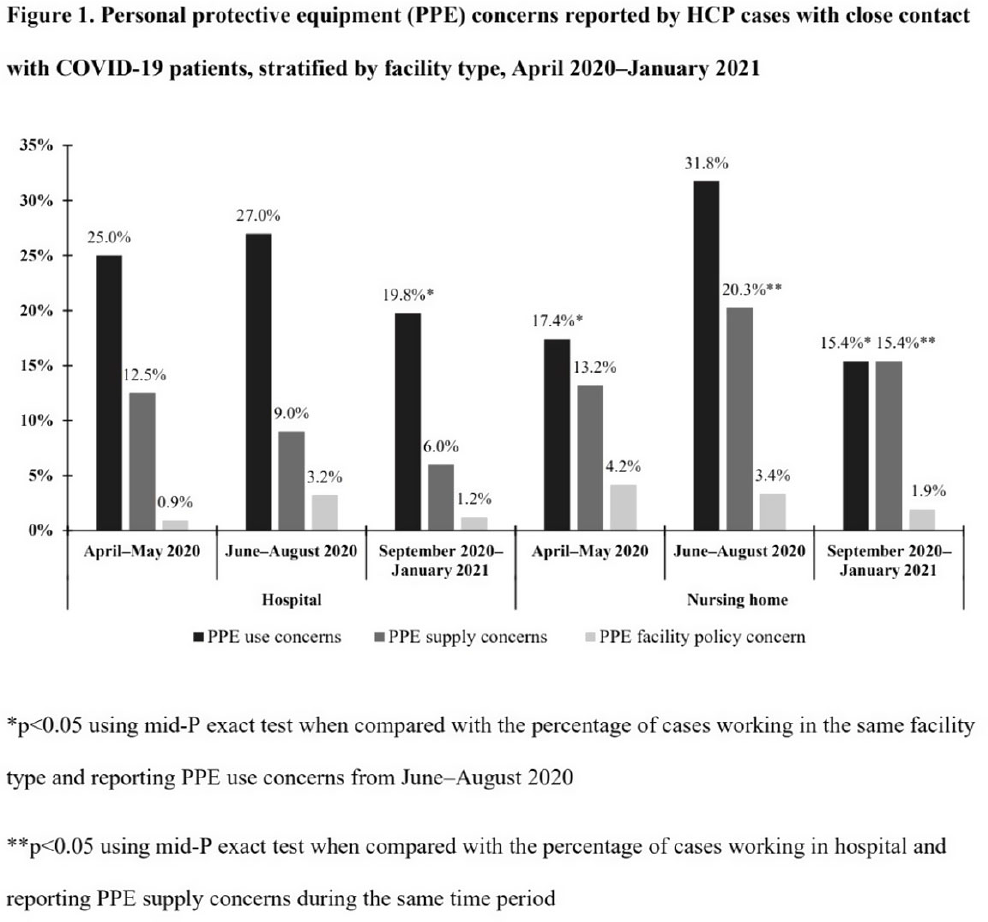
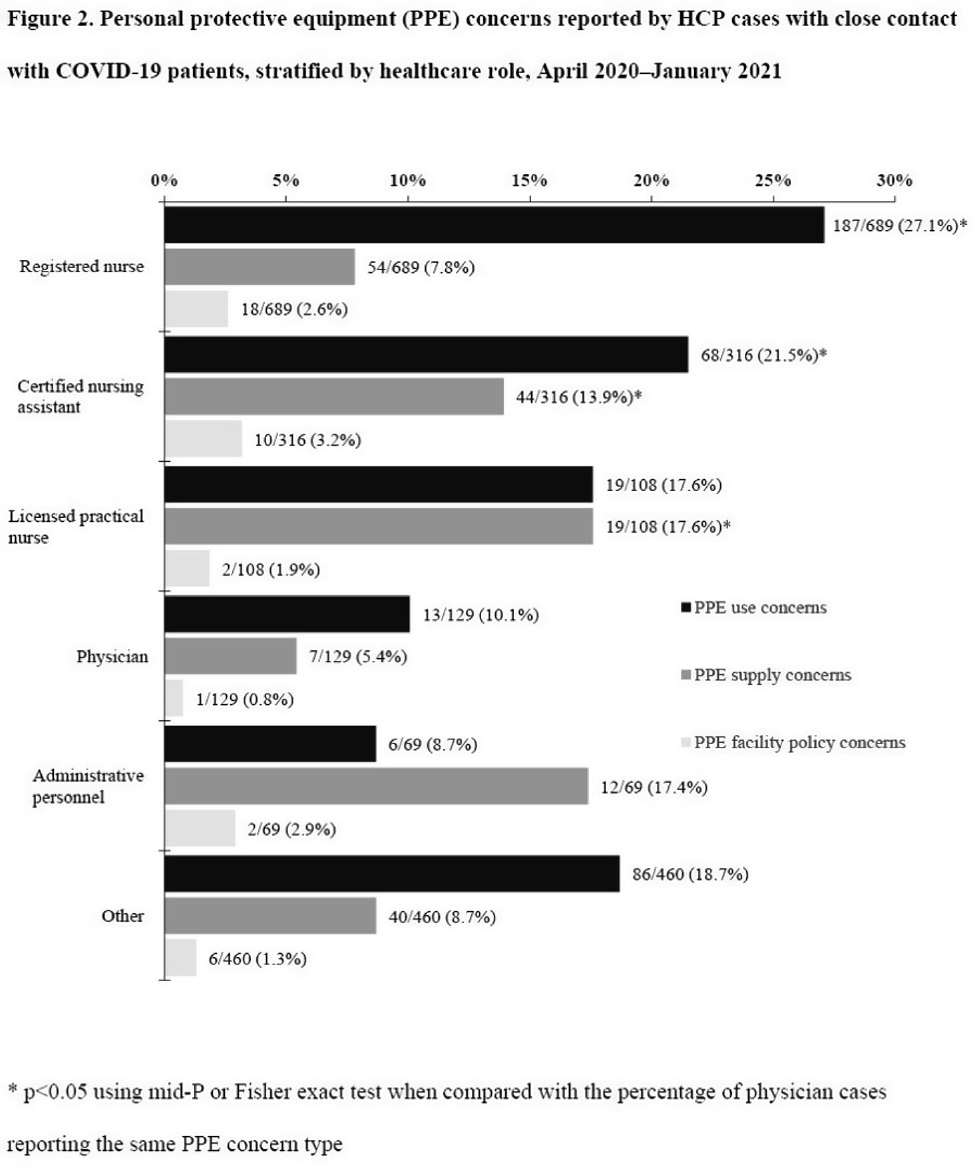
Background: Healthcare facilities have experienced many challenges during the COVID-19 pandemic, including limited personal protective equipment (PPE) supplies. Healthcare personnel (HCP) rely on PPE, vaccines, and other infection control measures to prevent SARS-CoV-2 infections. We describe PPE concerns reported by HCP who had close contact with COVID-19 patients in the workplace and tested positive for SARS-CoV-2. Method: The CDC collaborated with Emerging Infections Program (EIP) sites in 10 states to conduct surveillance for SARS-CoV-2 infections in HCP. EIP staff interviewed HCP with positive SARS-CoV-2 viral tests (ie, cases) to collect data on demographics, healthcare roles, exposures, PPE use, and concerns about their PPE use during COVID-19 patient care in the 14 days before the HCP’s SARS-CoV-2 positive test. PPE concerns were qualitatively coded as being related to supply (eg, low quality, shortages); use (eg, extended use, reuse, lack of fit test); or facility policy (eg, lack of guidance). We calculated and compared the percentages of cases reporting each concern type during the initial phase of the pandemic (April–May 2020), during the first US peak of daily COVID-19 cases (June–August 2020), and during the second US peak (September 2020–January 2021). We compared percentages using mid-P or Fisher exact tests (α = 0.05). Results: Among 1,998 HCP cases occurring during April 2020–January 2021 who had close contact with COVID-19 patients, 613 (30.7%) reported ≥1 PPE concern (Table 1). The percentage of cases reporting supply or use concerns was higher during the first peak period than the second peak period (supply concerns: 12.5% vs 7.5%; use concerns: 25.5% vs 18.2%; p Conclusions: Although lower percentages of HCP cases overall reported PPE concerns after the first US peak, our results highlight the importance of developing capacity to produce and distribute PPE during times of increased demand. The difference we observed among selected groups of cases may indicate that PPE access and use were more challenging for some, such as nonphysicians and nursing home HCP. These findings underscore the need to ensure that PPE is accessible and used correctly by HCP for whom use is recommended.
Funding: None
Disclosures: None



Indications for and Utility of Tracheal Aspirate Cultures for the Diagnosis of VAI
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s60-s61
-
- Article
-
- You have access
- Open access
- Export citation
-
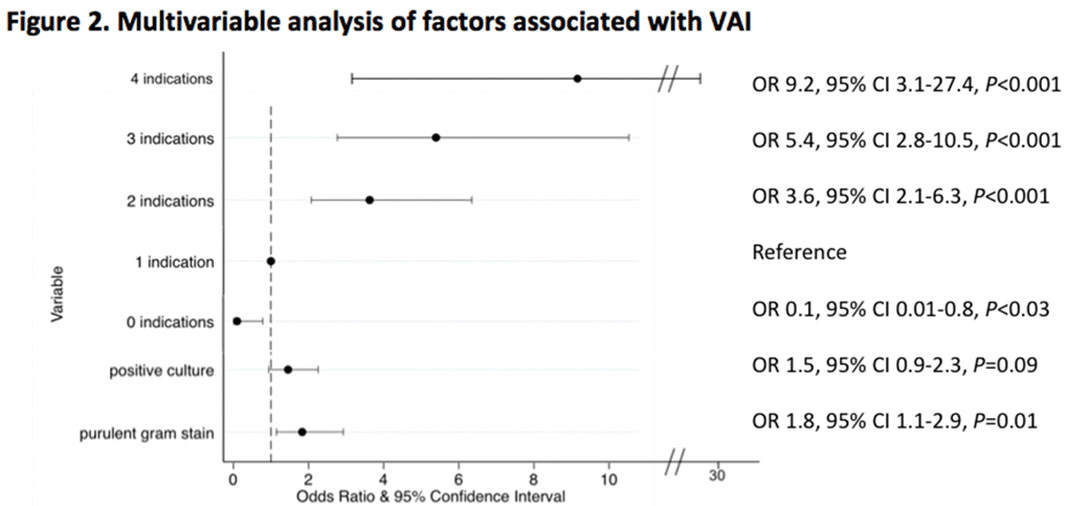
Background: Tracheal aspirate bacterial cultures are routinely collected in mechanically ventilated children for the evaluation of ventilator-associated infections (VAIs). However, frequent bacterial colonization of endotracheal and tracheostomy tubes contribute to the marginal performance characteristics of the test for diagnosing VAI. Published literature characterizing drivers of culture collection and the predictive value of positive cultures are limited. Methods: This single-center, retrospective cohort study included children admitted to the pediatric intensive care unit who were receiving mechanical ventilation for at least 48 hours and had 1 or more semiquantitative tracheal aspirate cultures collected between September 1, 2019, and August 31, 2020. Indications for culture collection were determined through medical record review and included fever, hypothermia, tracheal secretion changes, radiographic pneumonia, increased oxygen requirement, and/or increased positive end-expiratory pressure (PEEP). A positive culture was defined as moderate or heavy growth of a noncommensal bacterial organism. A purulent Gram stain was defined as detection of moderate or many white blood cells. Diagnosis of VAI was based on treating-clinician documentation and was ascertained through medical record review. Logistic regression accounting for clustering by patient was performed to estimate the association between indications for culture collection and (1) culture positivity, (2) purulent Gram stain, and (3) diagnosis of VAI. Results: In total, 625 tracheal aspirate cultures were performed in 261 unique patients. Common indications for culture collection included isolated fever or hypothermia (n = 124, 20%), fever with an increase in oxygen requirement or PEEP (n = 71, 11%), isolated increase in oxygen requirement or PEEP (n = 67, 11%), or isolated secretion change (n = 54, 9%) (Figure 1). Overall, 230 cultures (37%) were positive and 218 (35%) Gram stains were purulent. There were no associations between culture indications and a positive culture. Presence of isolated fever was negatively associated with a purulent Gram stain (odds ratio [OR], 0.49; 95% CI, 0.30–0.81; P = .005); otherwise, there were no associations between indication and purulent Gram stain. Finally, in a multivariable model, odds of VAI diagnosis increased with both the number of indications for culture collection and purulent Gram stain, but not with positive culture (Figure 2). Conclusions: Number and type of clinical signs were not associated with tracheal aspirate culture positivity or purulence on Gram stain, but they were associated with a clinical diagnosis of VAI. These findings suggest that positive tracheal aspirate cultures may not aid clinicians in the diagnosis of VAI, and they highlight the opportunity for improved diagnostic stewardship.
Funding: No
Disclosures: None
Figure 1.
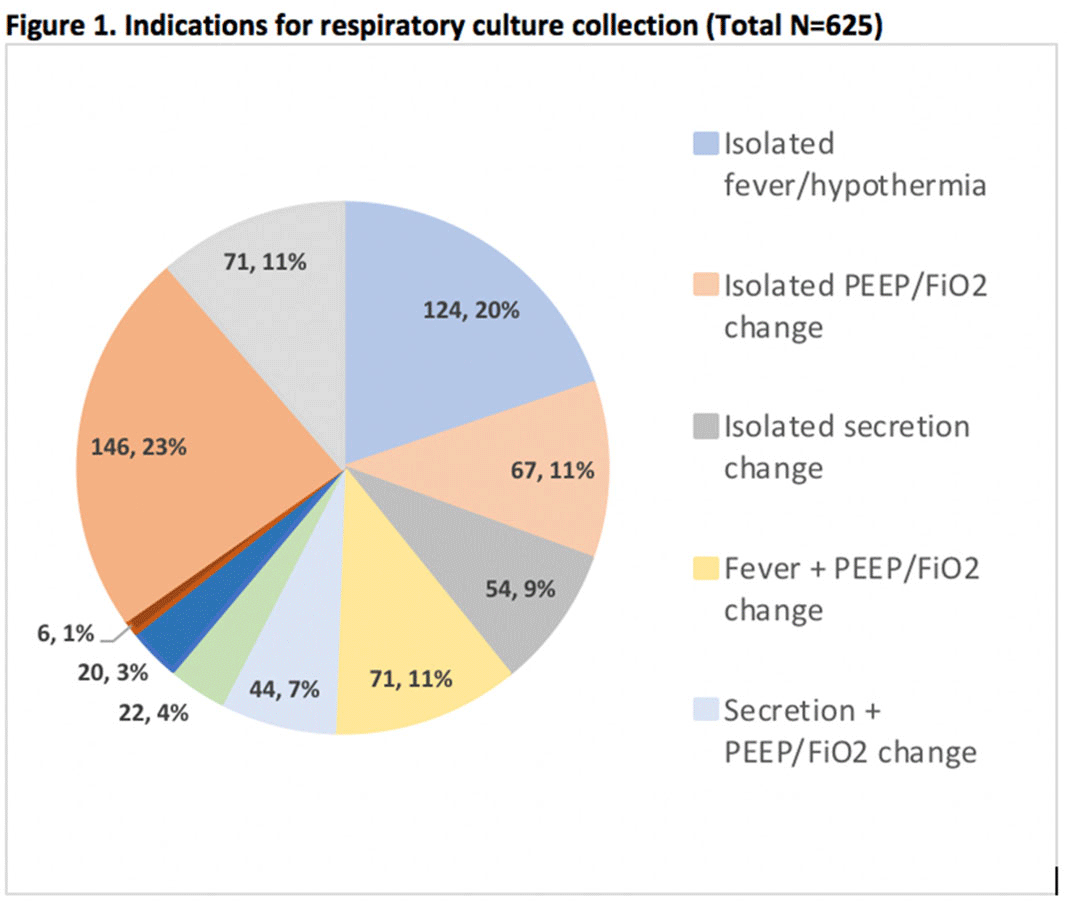
Figure 2.


The provision of ultra-processed foods and their contribution to sodium availability in Australian long day care centres
-
- Journal:
- Public Health Nutrition / Volume 21 / Issue 1 / January 2018
- Published online by Cambridge University Press:
- 29 June 2017, pp. 134-141
-
- Article
-
- You have access
- HTML
- Export citation
Inpatient Urine Cultures Are Frequently Performed Without Urinalysis or Microscopy: Findings From a Large Academic Medical Center
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 38 / Issue 4 / April 2017
- Published online by Cambridge University Press:
- 05 January 2017, pp. 455-460
- Print publication:
- April 2017
-
- Article
- Export citation
A Central Line Care Maintenance Bundle for the Prevention of Central Line–Associated Bloodstream Infection in Non–Intensive Care Unit Settings
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 37 / Issue 6 / June 2016
- Published online by Cambridge University Press:
- 21 March 2016, pp. 692-698
- Print publication:
- June 2016
-
- Article
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Philosophy
- Published online:
- 05 August 2015
- Print publication:
- 27 April 2015, pp ix-xxx
-
- Chapter
- Export citation
Time for a Revolution: Smart Energy and Microgrid Use in Disaster Response
-
- Journal:
- Disaster Medicine and Public Health Preparedness / Volume 8 / Issue 3 / June 2014
- Published online by Cambridge University Press:
- 11 June 2014, pp. 252-259
-
- Article
- Export citation
Royal College examination fees surplus
-
- Journal:
- The Psychiatrist / Volume 36 / Issue 7 / July 2012
- Published online by Cambridge University Press:
- 02 January 2018, pp. 273-274
- Print publication:
- July 2012
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Borderline personality features in childhood: A short-term longitudinal study
-
- Journal:
- Development and Psychopathology / Volume 17 / Issue 4 / December 2005
- Published online by Cambridge University Press:
- 12 December 2005, pp. 1051-1070
-
- Article
- Export citation
10 - Estimating age-at-death distributions from skeletal samples: a multivariate latent-trait approach
-
-
- Book:
- Paleodemography
- Published online:
- 28 August 2009
- Print publication:
- 03 January 2002, pp 193-221
-
- Chapter
- Export citation
7 - Mortality models for paleodemography
-
-
- Book:
- Paleodemography
- Published online:
- 28 August 2009
- Print publication:
- 03 January 2002, pp 129-168
-
- Chapter
- Export citation
Arthur Stanley Eddington Memorial Lectureship
-
- Journal:
- Philosophy / Volume 21 / Issue 80 / November 1946
- Published online by Cambridge University Press:
- 25 February 2009, p. 287
- Print publication:
- November 1946
-
- Article
-
- You have access
- Export citation
II. Some Aspects of the History of the Chantries during the Reign of Edward III
-
- Journal:
- Cambridge Historical Journal / Volume 4 / Issue 1 / 1932
- Published online by Cambridge University Press:
- 20 December 2011, pp. 26-50
- Print publication:
- 1932
-
- Article
- Export citation
II. The Appropriation of Parish Churches during the reign of Edward III1
-
- Journal:
- Cambridge Historical Journal / Volume 3 / Issue 1 / 1929
- Published online by Cambridge University Press:
- 20 December 2011, pp. 15-22
- Print publication:
- 1929
-
- Article
- Export citation
