
32 results
Factors associated with SARS-CoV-2 and community-onset invasive Staphylococcus aureus coinfection, 2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s84-s85
-
- Article
-
- You have access
- Open access
- Export citation
-
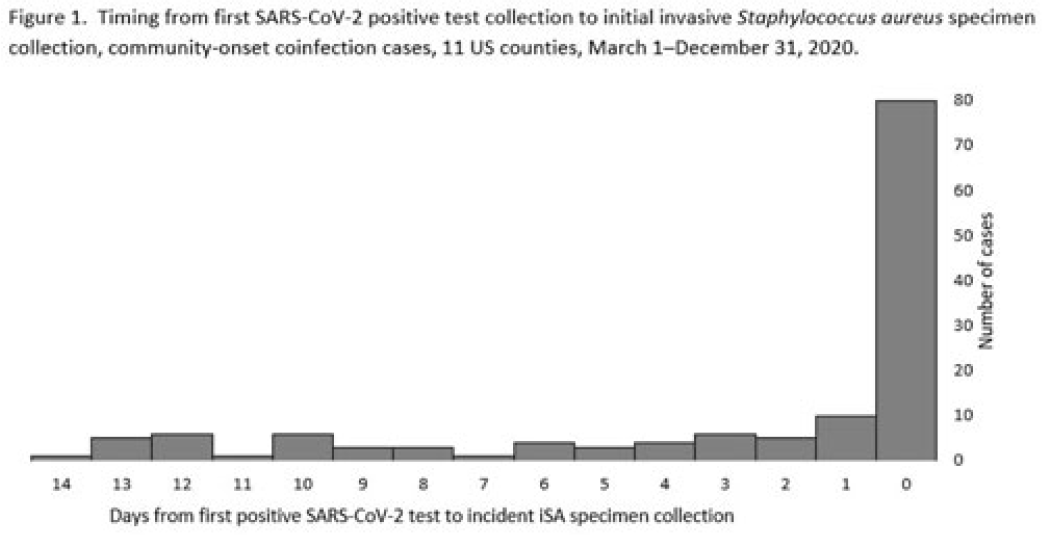
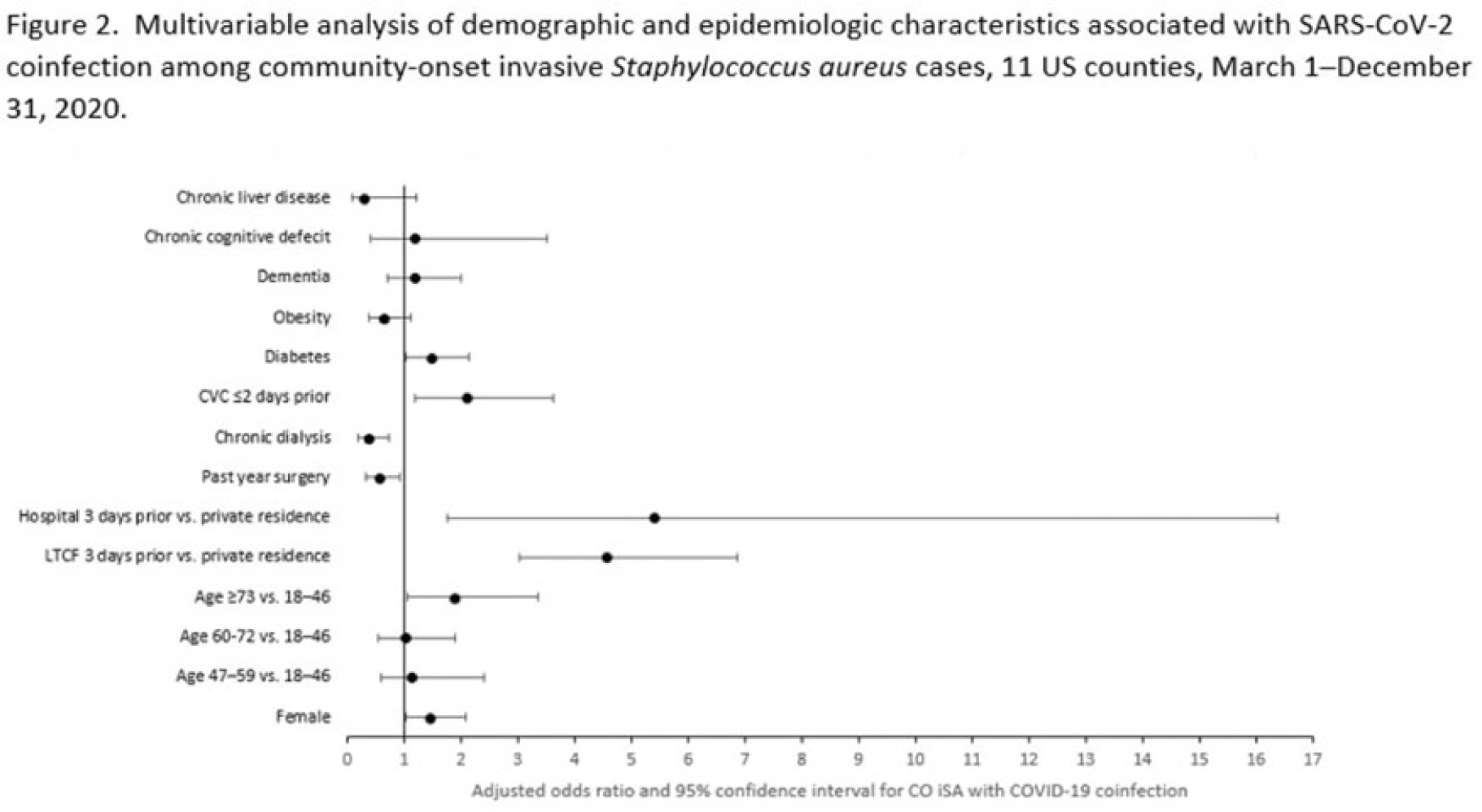
Background: Previous analyses describing the relationship between SARS-CoV-2 infection and Staphylococcus aureus have focused on hospital-onset S. aureus infections occurring during COVID-19 hospitalizations. Because most invasive S. aureus (iSA) infections are community-onset (CO), we characterized CO iSA cases with a recent positive SARS-CoV-2 test (coinfection). Methods: We analyzed CDC Emerging Infections Program active, population- and laboratory-based iSA surveillance data among adults during March 1–December 31, 2020, from 11 counties in 7 states. The iSA cases (S. aureus isolation from a normally sterile site in a surveillance area resident) were considered CO if culture was obtained <3 days after hospital admission. Coinfection was defined as first positive SARS-CoV-2 test ≤14 days before the initial iSA culture. We explored factors independently associated with SARS-CoV-2 coinfection versus no prior positive SARS-CoV-2 test among CO iSA cases through a multivariable logistic regression model (using demographic, healthcare exposure, and underlying condition variables with P<0.25 in univariate analysis) and examined differences in outcomes through descriptive analysis. Results: Overall, 3,908 CO iSA cases were reported, including 138 SARS-CoV-2 coinfections (3.5%); 58.0% of coinfections had iSA culture and the first positive SARS-CoV-2 test on the same day (Fig. 1). In univariate analysis, neither methicillin resistance (44.2% with coinfection vs 36.5% without; P = .06) nor race and ethnicity differed significantly between iSA cases with and without SARS-CoV-2 coinfection (P = .93 for any association between race and ethnicity and coinfection), although iSA cases with coinfection were older (median age, 72 vs 60 years , P<0.01) and more often female (46.7% vs 36.3%, P=0.01). In multivariable analysis, significant associations with SARS-CoV-2 coinfection included older age, female sex, previous location in a long-term care facility (LTCF) or hospital, presence of a central venous catheter (CVC), and diabetes (Figure 2). Two-thirds of co-infection cases had ≥1 of the following characteristics: age > 73 years, LTCF residence 3 days before iSA culture, and/or CVC present any time during the 2 days before iSA culture. More often, iSA cases with SARS-CoV-2 coinfection were admitted to the intensive care unit ≤2 days after iSA culture (37.7% vs 23.3%, P<0.01) and died (33.3% vs 11.3%, P<0.01). Conclusions: CO iSA patients with SARS-CoV-2 coinfection represent a small proportion of CO iSA cases and mostly involve a limited number of factors related to likelihood of acquiring SARS-CoV-2 and iSA. Although CO iSA patients with SARS-CoV-2 coinfection had more severe outcomes, additional research is needed to understand how much of this difference is related to differences in patient characteristics.
Disclosures: None


Social motivation in infancy is associated with familial recurrence of ASD
-
- Journal:
- Development and Psychopathology / Volume 36 / Issue 1 / February 2024
- Published online by Cambridge University Press:
- 03 October 2022, pp. 101-111
-
- Article
- Export citation
Increases in methicillin-sensitive Staphylococcus aureus bloodstream infection incidence, 2016–2019
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s63-s64
-
- Article
-
- You have access
- Open access
- Export citation
-
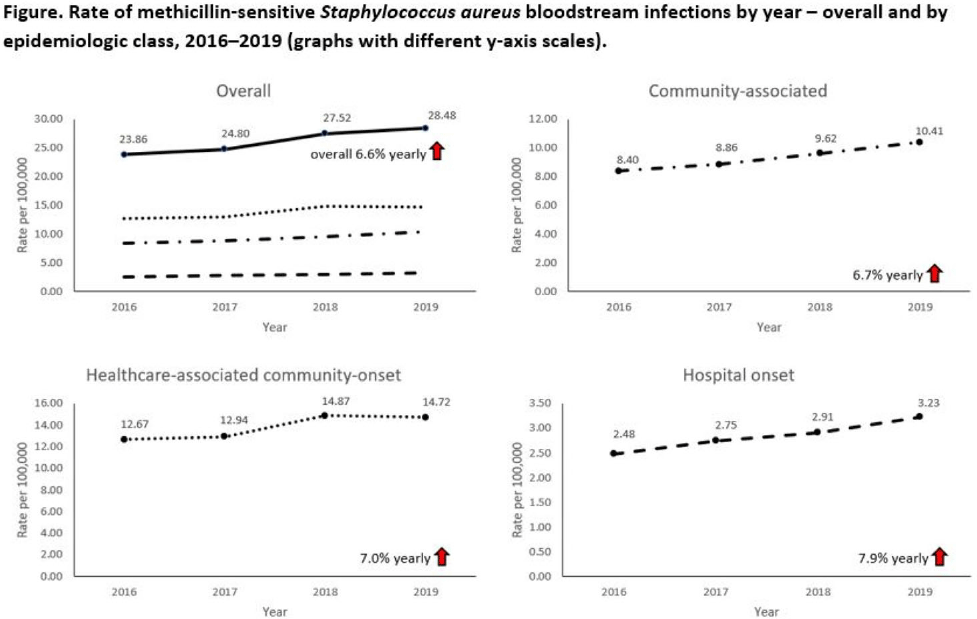
Background: Incidence of methicillin-sensitive Staphylococcus aureus (MSSA) bloodstream infections (BSIs) in the United States during 2012–2017 has been reported to have been stable for hospital-onset BSIs and to have increased 3.9% per year for community-onset BSIs. We sought to determine whether these trends continued in more recent years and whether there were further differences within subgroups of community-onset BSIs. Methods: We analyzed CDC Emerging Infections Program active, population- and laboratory-based surveillance data during 2016–2019 for MSSA BSIs from 8 counties in 5 states. BSI cases were defined as isolation of MSSA from blood in a surveillance area resident. Cases were considered hospital onset (HO) if culture was obtained >3 days after hospital admission and healthcare-associated community-onset (HACO) if culture was obtained on or after day 3 of hospitalization and was associated with dialysis, hospitalization, surgery, or long-term care facility residence within 1 year prior or if a central venous catheter was present ≤2 days prior. Cases were otherwise considered community-associated (CA). Annual rates per 100,000 census population were calculated for each epidemiologic classification; rates of HACO cases among chronic dialysis patients per 100,000 dialysis patients were calculated using US Renal Data System data. Annual increases were modeled using negative binomial or Poisson regression and accounting for changes in the overall population age group, and sex. Descriptive analyses were performed. Results: Overall, 8,344 MSSA BSI cases were reported. From 2016–2019 total MSSA BSI rates increased from 23.9 per 100,000 to 28.5 per 100,000 (6.6% per year; P < .01). MSSA BSI rates also increased significantly among all epidemiologic classes. HO cases increased from 2.5 per 100,000 to 3.2 per 100,000 (7.9% per year; P = .01). HACO cases increased from 12.7 per 100,000 to 14.7 per 100,000 (7.0% per year; P = .01). CA cases increased from 8.4 per 100,000 to 10.4 per 100,000 (6.7% per year; P < .01) (Fig. 1). Significant increases in MSSA BSI rates were also observed for nondialysis HACO cases (9.3 per 100,000 to 11.1 per 100,000; 7.8% per year; P < .01) but not dialysis HACO cases (1,823.2 per 100,000 to 1,857.4 per 100,000; 1.4% per year; P = .59). Healthcare risk factors for HACO cases were hospitalization in the previous year (82%), surgery (31%), dialysis (27%), and long-term care facility residence (19%). Conclusions: MSSA BSI rates increased from 2016–2019 overall, among all epidemiologic classes, and among nondialysis HACO cases. Efforts to prevent MSSA BSIs among individuals with healthcare risk factors, particularly those related to hospitalization, might have an impact on MSSA BSI rates.
Funding: None
Disclosures: None

Association of severe mental illness with stroke outcomes and process-of-care quality indicators: nationwide cohort study
-
- Journal:
- The British Journal of Psychiatry / Volume 221 / Issue 1 / July 2022
- Published online by Cambridge University Press:
- 19 August 2021, pp. 394-401
- Print publication:
- July 2022
-
- Article
-
- You have access
- HTML
- Export citation
Chapter 12 - Abolition
- from Part III - Activism
-
-
- Book:
- Frederick Douglass in Context
- Published online:
- 16 June 2021
- Print publication:
- 08 July 2021, pp 149-161
-
- Chapter
- Export citation
17 - Mary Ellen Pleasant, Nineteenth-Century Massachusetts and California (US)
- from Part III - Envisaging Emancipation during Second Slavery
-
-
- Book:
- As If She Were Free
- Published online:
- 24 September 2020
- Print publication:
- 08 October 2020, pp 312-330
-
- Chapter
- Export citation
Molecular Typing of Invasive Staphylococcus aureus from the Emerging Infections Program (EIP) Using Whole-Genome Sequencing
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s71-s72
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Characteristics Associated With Invasive Staphylococcus aureus Infection Rates in Nursing Homes, Emerging Infections Program
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s60-s61
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Antimicrobial Nonsusceptibility Among Invasive MRSA USA300 Strains by Healthcare Exposure, Three Sites, 2005–2016
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s120-s121
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Post-operative discharge education for parent caregivers of children with congenital heart disease: a needs assessment
-
- Journal:
- Cardiology in the Young / Volume 30 / Issue 12 / December 2020
- Published online by Cambridge University Press:
- 22 September 2020, pp. 1788-1796
-
- Article
- Export citation
Test–Retest Reliability of Concussion Baseline Assessments in United States Service Academy Cadets: A Report from the National Collegiate Athletic Association (NCAA)–Department of Defense (DoD) CARE Consortium
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 27 / Issue 1 / January 2021
- Published online by Cambridge University Press:
- 16 June 2020, pp. 23-34
-
- Article
- Export citation
Incidence of ischaemic heart disease and stroke among people with psychiatric disorders: retrospective cohort study
-
- Journal:
- The British Journal of Psychiatry / Volume 217 / Issue 2 / August 2020
- Published online by Cambridge University Press:
- 22 November 2019, pp. 442-449
- Print publication:
- August 2020
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
2 - Social Computing Systems and Ethical Considerations
-
-
- Book:
- Social Computing and the Law
- Published online:
- 28 September 2018
- Print publication:
- 11 October 2018, pp 14-24
-
- Chapter
- Export citation
Individual placement and support for vocational recovery in first-episode psychosis: randomised controlled trial
-
- Journal:
- The British Journal of Psychiatry / Volume 214 / Issue 2 / February 2019
- Published online by Cambridge University Press:
- 25 September 2018, pp. 76-82
- Print publication:
- February 2019
-
- Article
-
- You have access
- HTML
- Export citation
Challenges to Safe Injection Practices in Ambulatory Care
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 38 / Issue 5 / May 2017
- Published online by Cambridge University Press:
- 27 February 2017, pp. 614-616
- Print publication:
- May 2017
-
- Article
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Philosophy
- Published online:
- 05 August 2015
- Print publication:
- 27 April 2015, pp ix-xxx
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- Atlas of Surgical Techniques in Trauma
- Published online:
- 05 April 2015
- Print publication:
- 05 March 2015, pp ix-x
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- Case Studies in Pain Management
- Published online:
- 05 October 2014
- Print publication:
- 16 October 2014, pp xi-xv
-
- Chapter
- Export citation
Contributors
-
-
- Book:
- South and Southeast Asian Psycholinguistics
- Published online:
- 05 December 2013
- Print publication:
- 28 November 2013, pp xvii-xx
-
- Chapter
- Export citation
Therapy Contamination as a Measure of Therapist Treatment Adherence in a Trial of Cognitive Behaviour Therapy versus Befriending for Psychosis
-
- Journal:
- Behavioural and Cognitive Psychotherapy / Volume 43 / Issue 3 / May 2015
- Published online by Cambridge University Press:
- 29 October 2013, pp. 314-327
- Print publication:
- May 2015
-
- Article
- Export citation
