
96 results
Inequality on the frontline: A multi-country study on gender differences in mental health among healthcare workers during the COVID-19 pandemic
-
- Journal:
- Cambridge Prisms: Global Mental Health / Volume 11 / 2024
- Published online by Cambridge University Press:
- 04 March 2024, e34
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Night-time/daytime Protein S100B serum levels in paranoid schizophrenic patients
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S445-S446
-
- Article
-
- You have access
- Open access
- Export citation
Do attention-deficit/hyperactivity symptoms influence treatment outcome in gambling disorder?
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S58-S59
-
- Article
-
- You have access
- Open access
- Export citation
“Asking for help, quite a challenge”. Time from onset of symptoms to consultation with a psychiatrist
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S469-S470
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
One of the biggest challenges for primary care professionals is to know when it is appropriate to request a consultation with a psychiatrist. A complete medical history should be performed to detect anxious-depressive symptoms, as well as to determine the intensity, the trigger, time of evolution, and the functional repercussion (1). It is also important that the patient is able to express his or her symptoms and ask for help. The concept of “Alexitimia” refers to the difficulty of expressing feelings verbally, and is a frequent symptom in depressive patients (2).
In mild cases and with little repercussion, the physician himself can initiate treatment and follow up (3). However, on other occasions, it will be advisable to request a consultation with psychiatry.
ObjectivesThe main objective is to observe the time that elapses from the onset of symptoms until consultation with the Mental Health team is finally requested. Some preliminary results can already be obtained from this data collection.
MethodsWe have decided to carry out a descriptive study, collecting different variables from patients attending a first Psychiatry consultation.
ResultsIn a total sample of 208 patients, the majority (67%) were between 31 and 60 years old. Following the DSM-V criteria (4), patients were classified into groups according to their disorder: Adaptive, depressive, or other. These data were cross-referenced (Figure 1).
Subsequently, the time elapsed from the onset of symptoms (referred by the patients) was collected, until the referral to Psychiatry was processed. In order to make a comparison, average time (in days) was calculated for the different groups according to their age and diagnosis.
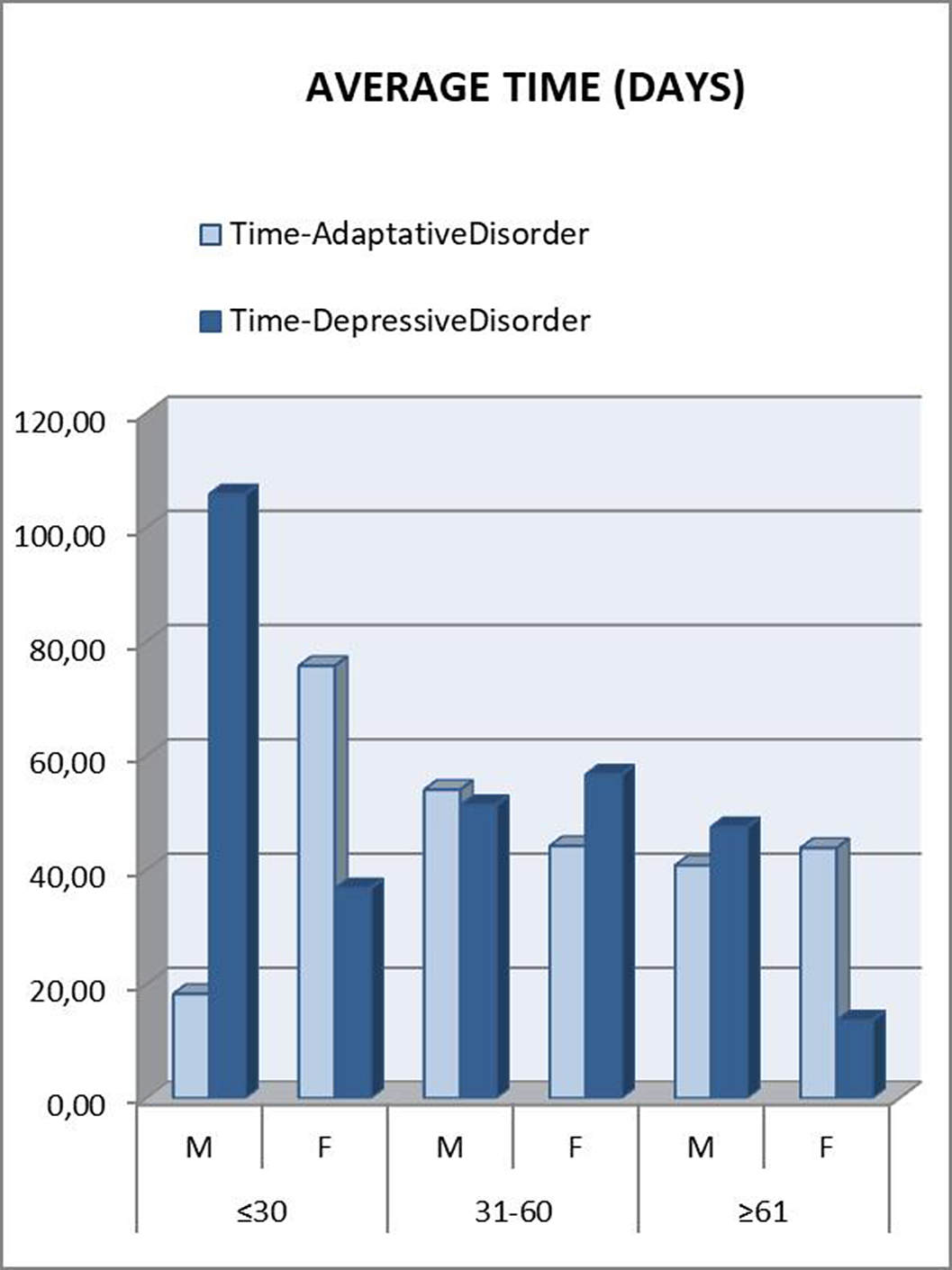
Those patients under 30 years were referred to psychiatry later. A downward trend was seen as the age range increased. In the “younger than 30” and “between 31 and 60” groups, patients who met criteria for Depressive Disorder took longer to be referred, which was striking considering that they are usually considered as more severe patients (Figure 2). This can be attributed to a greater difficulty in expressing their emotions (alexithymia), as another depressive symptom. Disaggregating these data by gender, the patients who clearly took the longest to be referred were men under 30 years old with a final diagnosis of Depressive Disorder (Figure 3). This gender difference is consistent with the social impact of alexithymia according to some articles (5).
Image:
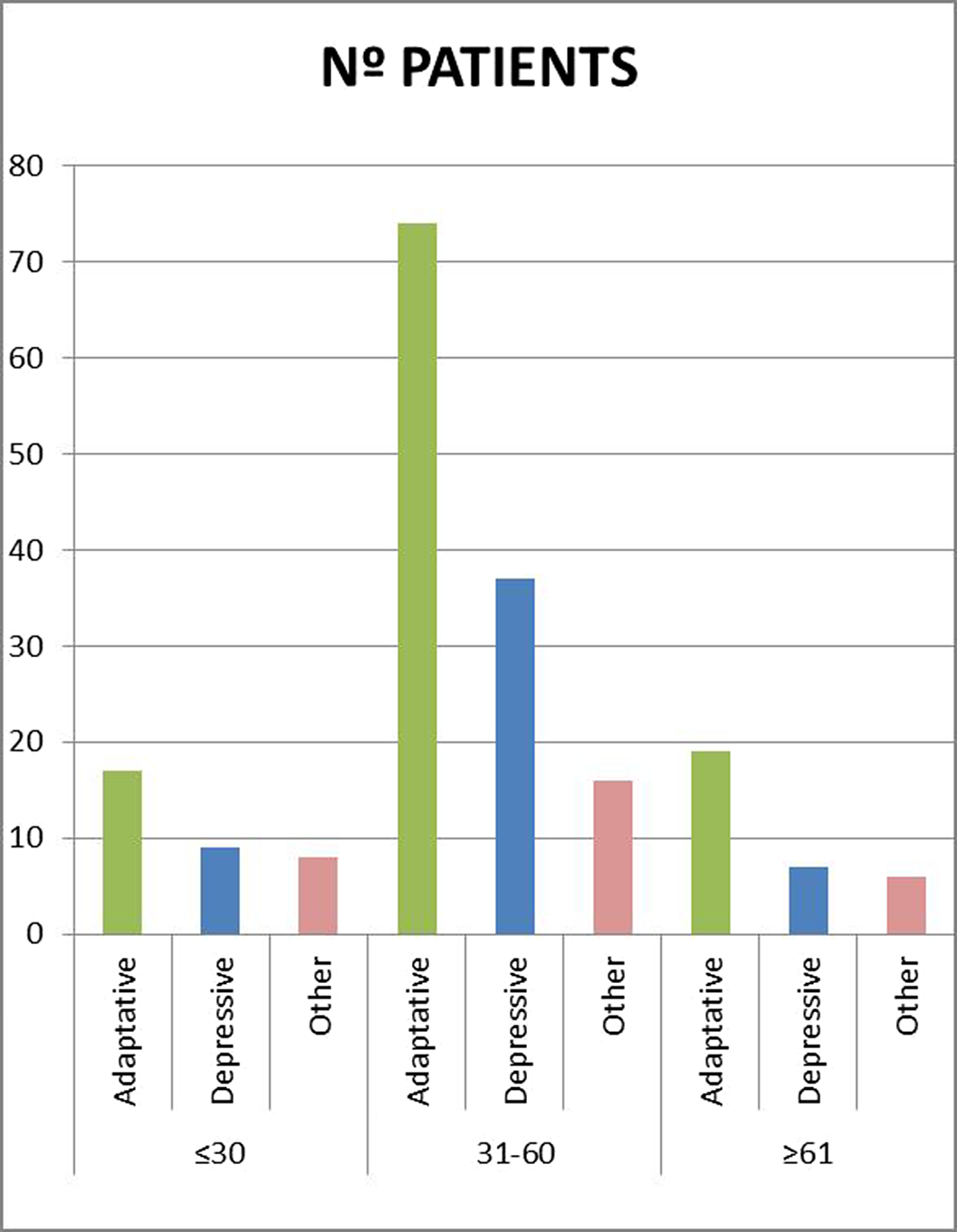
Image 2:
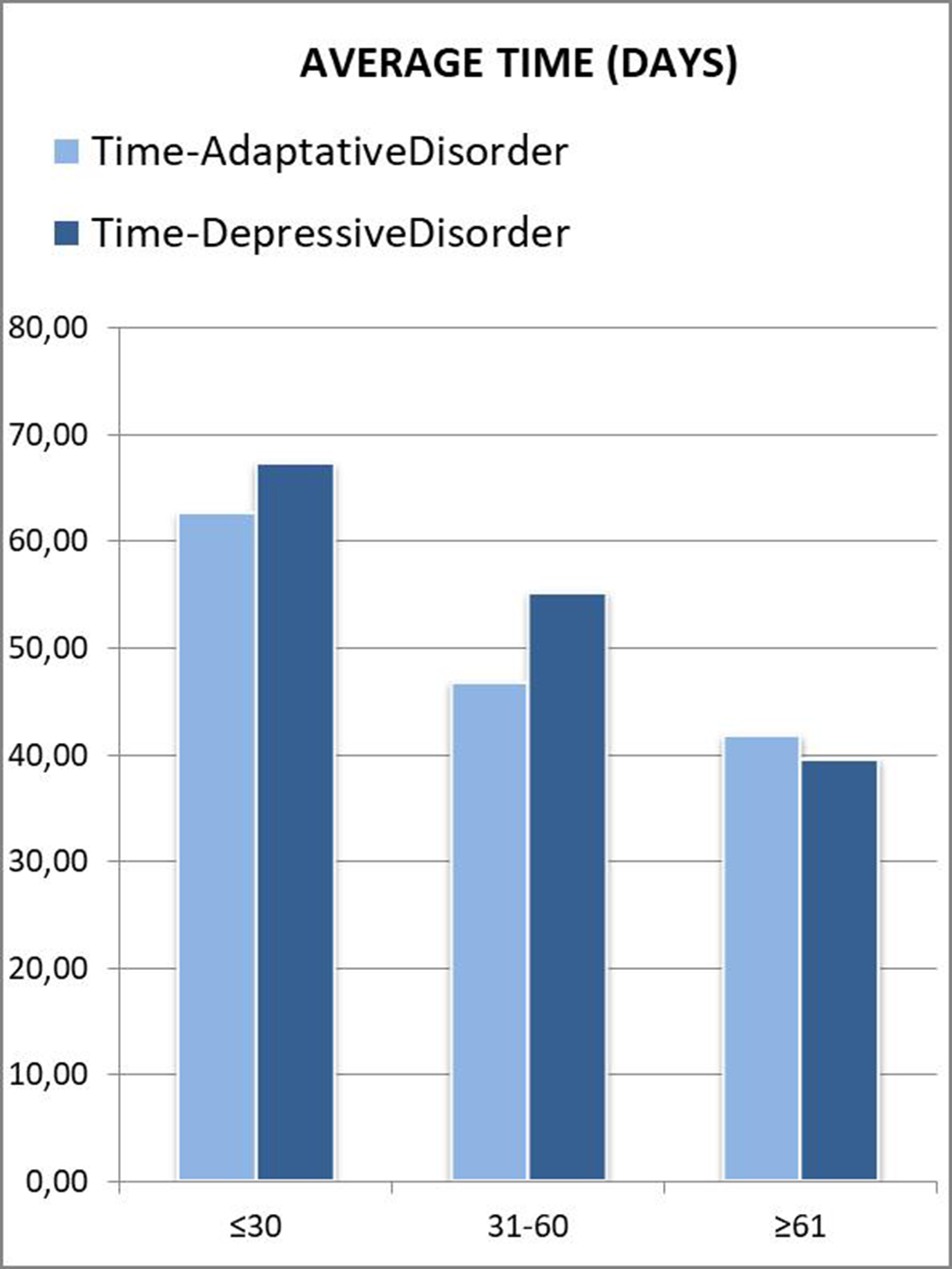
Image 3:
 Conclusions
ConclusionsIt is important that primary care physicians know how to take a complete history in those patients with symptoms of anxiety and depression.
In many cases, patients themselves have difficulties expressing their emotions and feelings (alexithymia), which may be another symptom of their discomfort.
This may lead to a delay in the time until referral to a psychiatry is requested, and therefore a worsening of symptoms.
Disclosure of InterestNone Declared



Association between adverse childhood experiences and the number of suicide attempts in lifetime
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S561-S562
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Adverse childhood experiences (ACEs), defined as abuse, neglect, or a dysfunctional household in childhood, have been associated with suicidality (Fjeldsted et al., 2020). Every type of ACE has a direct impact on suicide ideation, self-harm and/or suicide attempt (Angelakis et al., 2019).
ObjectivesWe aim to quantify the association between types of ACEs (including emotional, physical, sexual abuse, and emotional and physical neglect) and the number of suicide attempts in lifetime.
MethodsWe included 748 patients who attempted suicide at least once. They were asked to complete the Columbia-Suicide Severity Rating Scale (CSSRS), and the Childhood Trauma Questionnaire-Short Form (CTQ-SF). Logistic regression models were run to assess the association between each ACE type and the number of suicide attempts.
ResultsPoisson univariate regression analyses show a linear trend in the relationship between having a higher number of suicide attempts and having suffered every ACE type in childhood (p<0.05). Our results show a lower percentage of previous suicide attempts among participants without ACEs, and an increasing tendency among patients with various types of ACEs. The rate of ACEs types is significantly higher in the group with previous suicide attempts than in the first-attempt group (p=0.000).
Image:
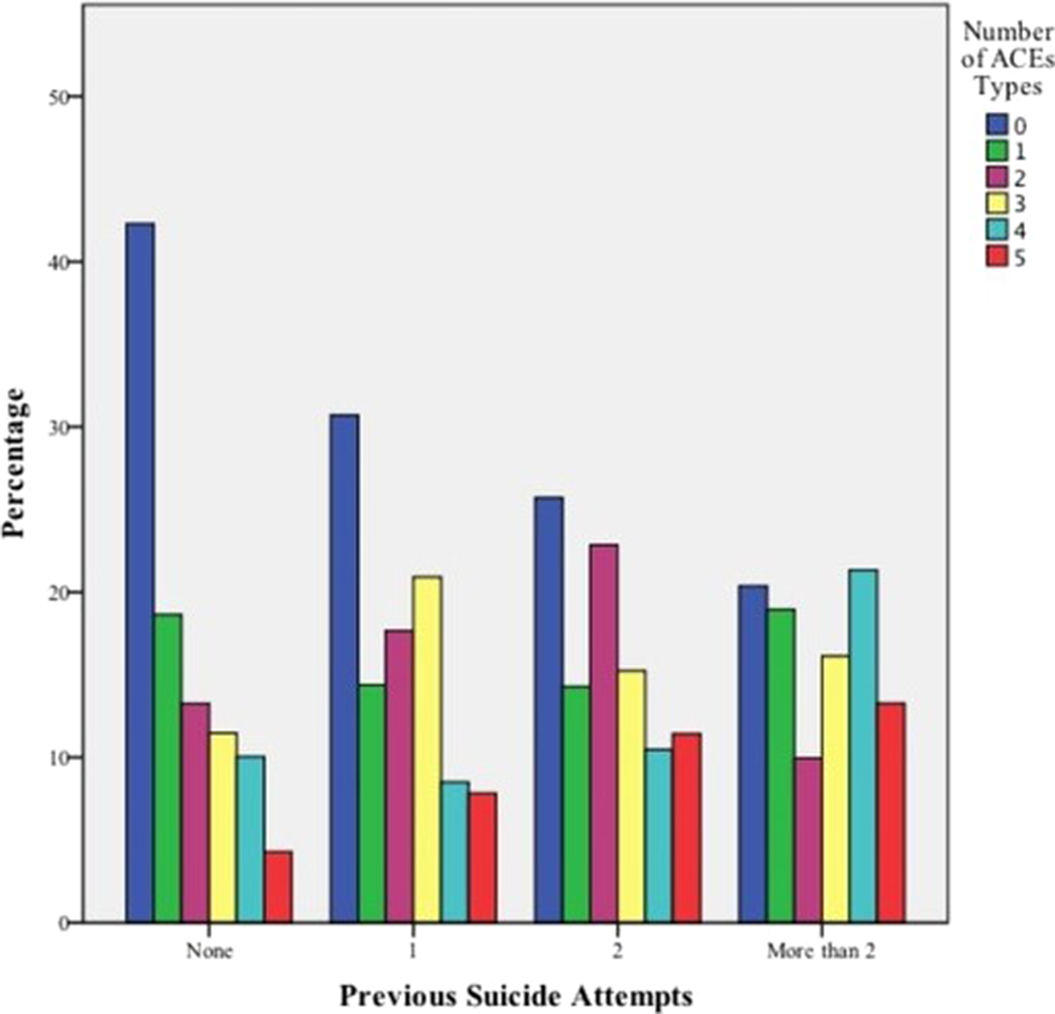
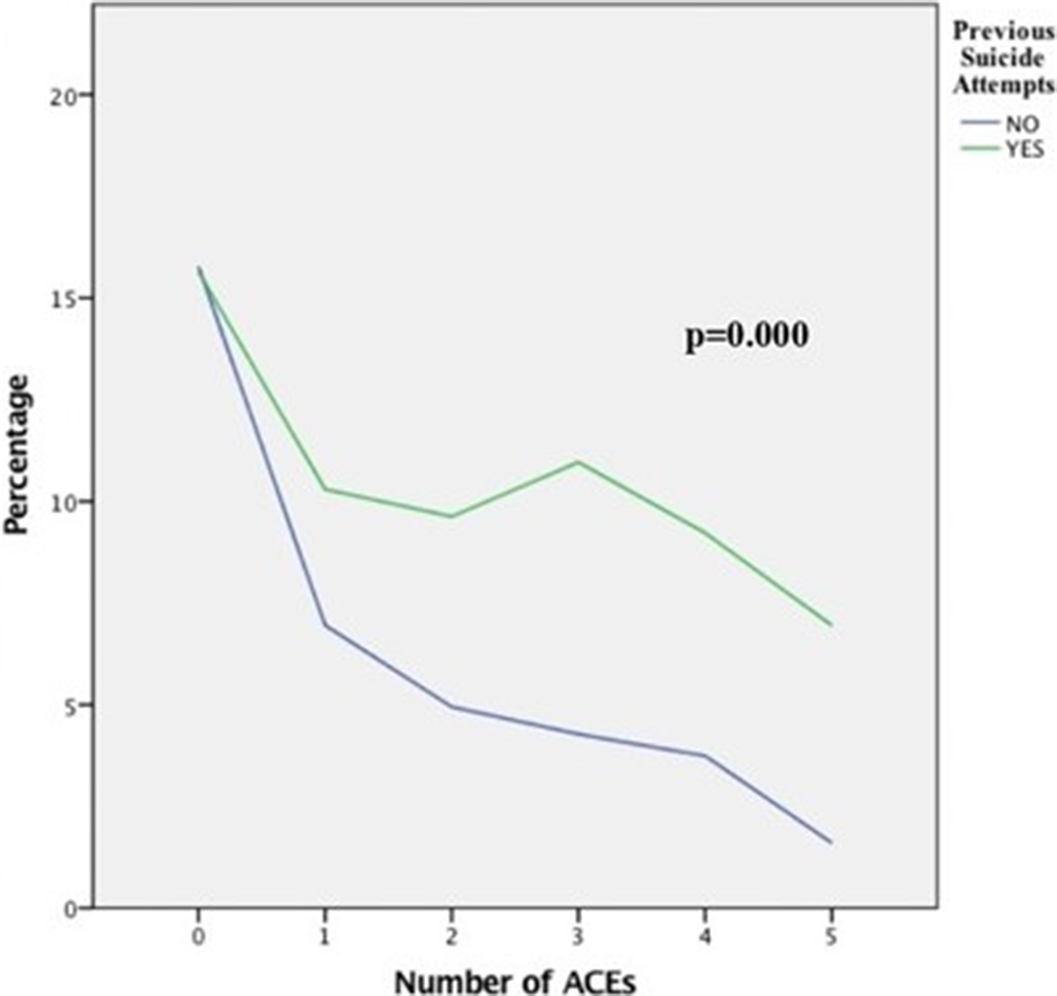
Image 2:
ConclusionsThis study contributes to clarify the role of childhood trauma in the number of suicide attempts in lifetime. This has important implications for reducing suicide rates, and preventing future re-attempts. Further studies analysing every construct of childhood trauma may contribute to the detection of suicidal behaviour.
FundingsThis work was supported by the Instituto de Salud Carlos III (grant number: PI19/00941 SURVIVE) and co-funded by the European Union (grant numbers: COV20/00988, PI17/00768), the European Union’s Horizon 2020 research and innovation programme Societal Challenges (grant number: 101016127), and the Fundación Española de Psiquiatría y Salud Mental
AcknowledgementsSURVIVE project (PI19/00941)
KeywordsSuicide attempt, Adverse Childhood Experiences
ReferencesAngelakis, I., Gillespie, E. L., & Panagioti, M. (2019). Childhood maltreatment and adult suicidality: A comprehensive systematic review with meta-analysis. Psychological Medicine, 49(7), 1057-1078. https://doi.org/10.1017/S0033291718003823
Fjeldsted, R., Teasdale, T. W., & Bach, B. (2020). Childhood trauma, stressful life events, and suicidality in Danish psychiatric outpatients. Nordic Journal of Psychiatry, 74(4), 280-286. https://doi.org/10.1080/08039488.2019.1702096
Disclosure of InterestNone Declared


DOCTOR, I’M PREGNANT. Psychopharmacological treatment of depression in pregnant women. A clinical case of a pregnant woman and major depressive disorder
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S1011
-
- Article
-
- You have access
- Open access
- Export citation
Efficacy of maintenance electroconvulsive therapy in recurrent depression: a case series
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S832
-
- Article
-
- You have access
- Open access
- Export citation
UNTIL IT BURSTS OR ALL OF US BURST. A SCHIZOTYPICAL CASE.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S967
-
- Article
-
- You have access
- Open access
- Export citation
Delirious episode secondary to rotigotine: the psychotic patch
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S626
-
- Article
-
- You have access
- Open access
- Export citation
Bipolar disorder and substance use: Risk factors and prognosis
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S704
-
- Article
-
- You have access
- Open access
- Export citation
I don’t know where I’m going or where I come from. Self-disorders in schizophrenia.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S1069-S1070
-
- Article
-
- You have access
- Open access
- Export citation
Relationship between CAINS negative symptoms and cognition, psychosocial functioning and quality of life in patients with a first psychotic episode of schizophrenia
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S641-S642
-
- Article
-
- You have access
- Open access
- Export citation
Conversive and Factitious disorders: Differential diagnosis based on a case report
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S687
-
- Article
-
- You have access
- Open access
- Export citation
PEAKS AND VALLEYS: BIPOLAR DISORDER, RAPID CYCLERS AND ENERGY DRINKS CONSUMPTION
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S702-S703
-
- Article
-
- You have access
- Open access
- Export citation
Relationship between Signals Regulating Energy Homeostasis and Neuropsychological and Clinical Features in Gambling Disorder: A Case-Control Study
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S328
-
- Article
-
- You have access
- Open access
- Export citation
Late diagnosis of attention deficit hyperactivity disorder and cocaine abuse
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S335-S336
-
- Article
-
- You have access
- Open access
- Export citation
Memory complaints and quality of life in a patient with mild cognitive impairment
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S937-S938
-
- Article
-
- You have access
- Open access
- Export citation
“The cat and the calcium”. A case of delirium secondary to hypercalcaemia.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S946-S947
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Interconsultation with the psychiatry service is frequently requested from other specialties for the assessment and treatment of patients who present neuropsychiatric symptoms secondary to organic alterations. On the other hand (and in relation to this case), within the possible causes for the elevation of calcaemia figures, the most frequent are hyperparathyroidism and neoplasms, representing between these two entities 90% of cases (1).
Among the organic mental disorders, Delirium stands out, with an approximate prevalence between 1 and 2% (general population), which increases in hospitalized and elderly patients (2).
ObjectivesPresentation of a clinical case about a patient with delirium secondary to hypercalcemia, with hallucinations and behavioral disturbance.
MethodsBibliographic review including the latest articles in Pubmed about delirium (causes and treatment) and hypercalcaemia secondary to neoplasms.
ResultsWe present a 52-year-old male patient, who went to the emergency room accompanied by his wife, due to behavioral alteration. Two days before, he had been evaluated by Neurology, after a first epileptic crisis (with no previous history) that resolved spontaneously. At that time, it was decided not to start antiepileptic treatment.
The patient reported that he had left his house at midnight, looking for a cat. As he explained, this cat had appeared in his house and had left his entire bed full of insects. His wife denied that this had really happened, and when she told the patient to go to the emergency room, he had become very upset.
As background, the patient used to consume alcohol regularly, so the first hypothesis was that this was a withdrawal syndrome. However, although the consumption was daily, in recent months it was not very high, and at that time no other symptoms compatible with alcohol withdrawal were observed (tremor, tachycardia, sweating, hypertension…).
We requested a general blood test and a brain scan. The only relevant finding was hypercalcaemia 12.9mg/dL (which could also be the origin of the previous seizure). It was decided to start treatment with Diazepam and Tiapride in the emergency room, with serum perfusion, and keep under observation. After several hours, the patient felt better, the hallucinations disappeared, and calcium had dropped to 10.2mg/dL. A preferential consultation was scheduled, due to suspicion that the hypercalcaemia could be secondary to a tumor process.
Image:
 Conclusions
ConclusionsIt is important to rule out an organic alteration in those patients who present acute psychiatric symptoms. Hypercalcaemia is frequently associated with tumor processes (1) due to secretion of PTH-like peptide (4), so a complete study should be carried out in these cases.
Delirium has a prevalence between 1 and 2% in the general population (2).
Psychopharmacological treatment is used symptomatically, with antipsychotics (3). For the episode to fully resolve, the underlying cause must be treated.
Disclosure of InterestNone Declared

“Keeping an eye on amylase”. Side effects of antidepressants
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S831
-
- Article
-
- You have access
- Open access
- Export citation
Trends in the incidence of hospital-treated suicide attempts during the COVID-19 pandemic in Oviedo, Spain
-
- Journal:
- European Psychiatry / Volume 66 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 03 February 2023, e23
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
