
14 results
Double-swab 5% versus single-swab 10% iodophor for reducing methicillin-resistant Staphylococcus aureus with routine chlorhexidine bathing
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 12 / December 2022
- Published online by Cambridge University Press:
- 26 August 2021, pp. 1937-1939
- Print publication:
- December 2022
-
- Article
- Export citation
Results of a Multicenter Diagnostic Stewardship Collaborative to Optimize Blood Culture Use in Critically Ill Children
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s27
-
- Article
-
- You have access
- Open access
- Export citation
-
Group Name: Bright STAR Authorship Group
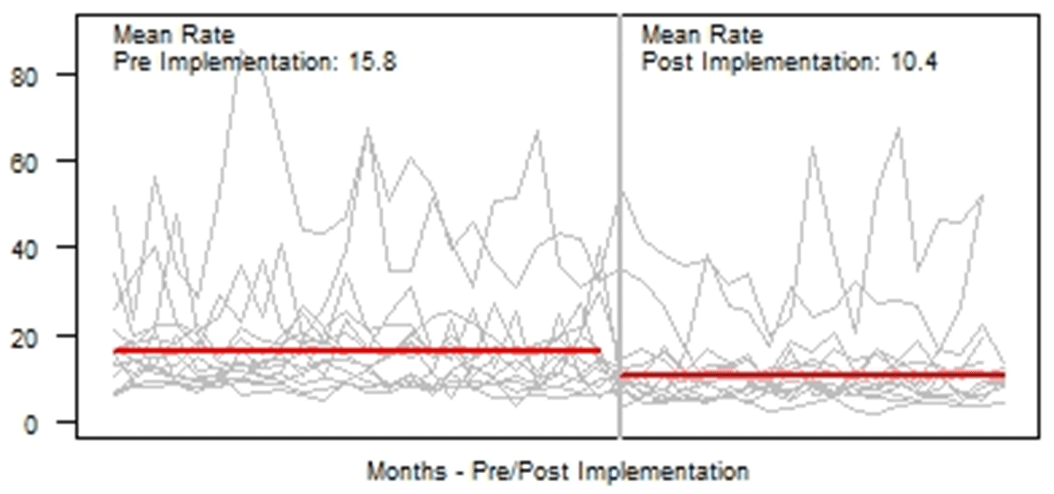
Background: Blood cultures are fundamental in the diagnosis and treatment of sepsis. Culture practices vary widely, and overuse can lead to false-positive results and unnecessary antibiotics. Our objective was to describe the implementation of a multisite quality improvement collaborative to reduce unnecessary blood cultures in pediatric intensive care unit (PICU) patients, and its 18-month impact on blood culture rates and safety metrics. Methods: In 2018, 14 PICUs joined the Blood Culture Improvement Guidelines and Diagnostic Stewardship for Antibiotic Reduction in Critically Ill Children (Bright STAR) Collaborative, designed to understand and improve blood culture practices in critically ill children. Guided by a centralized multidisciplinary study team, sites first reviewed existing evidence for safe reduction of unnecessary blood cultures and assessed local practices and barriers to change. Subsequently, local champions developed and implemented clinical decision-support tools informed by local patient needs to guide new blood-culture practices. The coordinating study team facilitated regular evaluations and discussions of project progress through monthly phone calls, site visits if requested by sites or the study team, and collaborative-wide teleconferences. The study team collected monthly blood culture rates and monitored for possible delays in obtaining blood cultures using a standardized review process as a safety balancing metric. We compared 24 months of baseline data to 18 months of postimplementation using a Poisson regression model accounting for the site-specific patient days and correlation of culture use within a site over time. Results: Across the 14 sites, before implementation, 41,768 blood cultures were collected over 259,701 PICU patient days. The mean preimplementation site-specific blood culture rate was 15.7 cultures per 100 patient days (rate range, 9.6–48.2 cultures per 100 patient days). After implementation, 22,397 blood cultures were collected over 208,171 PICU patient days. The mean postimplementation rate was 10.4 cultures per 100 patient days (rate range, 4.7–28.3 cultures per 100 patient days), which was 33.6% lower than the preimplementation (relative rate 0.66; 95% CI, 0.65–0.68 p <0.01). In 18 months post-implementation, sites reviewed 793 positive blood cultures, and identified only one suspected delay in culture collection possibly attributable to the site’s blood culture reduction program. Conclusions: Multidisciplinary quality improvement teams safely facilitated a 33.6% average reduction in blood culture use in critically ill children at 14 hospitals. Future collaborative work will determine the impact of blood culture diagnostic stewardship on antibiotic use and other important patient safety outcomes.
Funding: No
Disclosures: None
Figure 1.

Alcohol-impregnated caps and ambulatory central-line–associated bloodstream infections (CLABSIs): A randomized clinical trial
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 4 / April 2021
- Published online by Cambridge University Press:
- 12 October 2020, pp. 431-439
- Print publication:
- April 2021
-
- Article
- Export citation
Universal Decolonization Reduces MDRO Burden on High-Touch Objects in Nursing Home Resident Rooms and Common Areas
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s54-s55
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Impact of Roommates on MDRO Spread in Nursing Homes
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s66-s67
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Decreased Hospitalizations and Costs From Infection in Sixteen Nursing Homes in the SHIELD OC Regional Decolonization Initiative
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s7-s8
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Bright STAR Collaborative Consensus Guidelines for Blood Culture Use in Critically Ill Children
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s22-s23
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
A Prospective, Holistic, Multicenter Approach to Tracking and Understanding Bloodstream Infections in Pediatric Hematology-Oncology Patients
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 38 / Issue 6 / June 2017
- Published online by Cambridge University Press:
- 12 April 2017, pp. 690-696
- Print publication:
- June 2017
-
- Article
-
- You have access
- HTML
- Export citation
Prevalence of and Factors Associated With Multidrug Resistant Organism (MDRO) Colonization in 3 Nursing Homes
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 37 / Issue 12 / December 2016
- Published online by Cambridge University Press:
- 27 September 2016, pp. 1485-1488
- Print publication:
- December 2016
-
- Article
- Export citation
Contributors
-
-
- Book:
- The Cambridge Dictionary of Philosophy
- Published online:
- 05 August 2015
- Print publication:
- 27 April 2015, pp ix-xxx
-
- Chapter
- Export citation
Evaluating Application of the National Healthcare Safety Network Central Line—Associated Bloodstream Infection Surveillance Definition: A Survey of Pediatric Intensive Care and Hematology/Oncology Units
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 34 / Issue 7 / July 2013
- Published online by Cambridge University Press:
- 02 January 2015, pp. 663-670
- Print publication:
- July 2013
-
- Article
- Export citation
Surveillance of Hospital-Acquired Central Line–Associated Bloodstream Infections in Pediatric Hematology-Oncology Patients Lessons Learned, Challenges Ahead
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 34 / Issue 3 / March 2013
- Published online by Cambridge University Press:
- 02 January 2015, pp. 315-320
- Print publication:
- March 2013
-
- Article
- Export citation
Epidemiology of Central Line-Associated Bloodstream Infections in the Pediatric Intensive Care Unit
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 32 / Issue 12 / December 2011
- Published online by Cambridge University Press:
- 02 January 2015, pp. 1200-1208
- Print publication:
- December 2011
-
- Article
- Export citation
Increased Catheter-Related Bloodstream Infection Rates After the Introduction of a New Mechanical Valve Intravenous Access Port
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 27 / Issue 1 / January 2006
- Published online by Cambridge University Press:
- 21 June 2016, pp. 67-70
- Print publication:
- January 2006
-
- Article
- Export citation
