



Recent editorials in the BJPsych Reference Zhang, Zhou, Liu and Hashimoto1–Reference Kesner and Horáček3 concerning the effects of COVID-19 on psychiatry were written at the outset of the pandemic. It would perhaps have been impossible for their authors to have predicted what has been by far the most devastating effect of the pandemic on psychiatric care: suspension or reduction of normal service provision. This has included minimisation of face-to-face care and, crucially, limited provision of one of the most effective psychiatric treatments, electroconvulsive therapy (ECT).
ECT typically involves aerosol-generating procedures (AGPs), including bag-mask ventilation, suction of secretions and, less commonly, laryngeal mask or endotracheal airway insertion and removal.Reference Purushothaman, Fung, Reinders, Garrett-Walcott, Buda and Moudgil4 It was apparent early on in the pandemic that ECT might pose a risk of viral transmission between patients and healthcare professionals, and that alterations to practice might be needed to ensure safety. However, it quickly became apparent that provision of ECT was rapidly diminishing in most areas and even grinding to a halt in some. Anecdotally, anaesthesia staff had been redeployed in many localities but, although anticipated, significant levels of staff sickness and shielding were yet to be encountered.
We present the findings of a survey conducted at two time points during the pandemic. The aim of the study was to establish the nature, extent and effects of any disruption to ECT services, with a view to establishing how obstacles to full service provision might be overcome in due course.
The survey was conducted by the ECT Accreditation Service (ECTAS), the department of the Royal College of Psychiatrists responsible for the setting and monitoring of clinical standards in the delivery of ECT services across three regions of the UK (England, Wales and Northern Ireland) as well as in the Republic of Ireland. The survey did not cover ECT clinics in Scotland, where standards are set and monitored by the Scottish ECT Accreditation Network.
Method
Each ECTAS member clinic was sent a link to an online survey via the network's email discussion group during two 1-week periods in April and July 2020. The questionnaire was developed following consultation with clinical experts from ECTAS. Reminders were sent to non-responding clinics 2 days before the closing dates. Because this was a retrospective survey of clinicians and did not influence patient care, ethical approval was not required.
In addition to the questions set out in Table 1, respondents were asked for the total number of patients at their clinic who had had their treatment affected by the pandemic since 16 March 2020, including those who would otherwise have received ECT but had not.
Table 1 Survey responses from ECT clinics in England, Wales, Northern Ireland and the Republic of Ireland
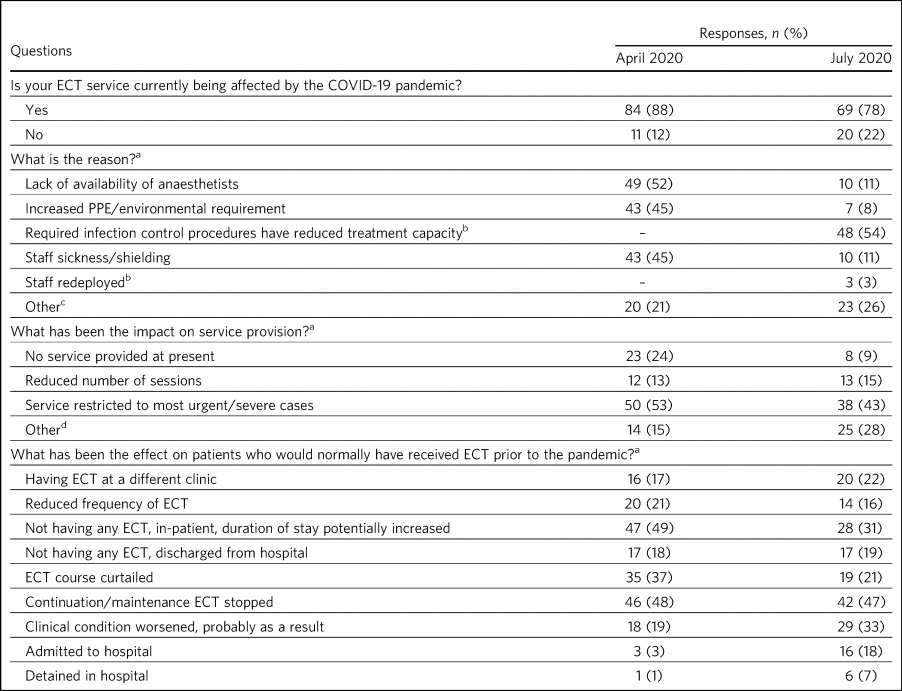
ECT, electroconvulsive therapy; COVID-19, coronavirus disease 2019; PPE, personal protective equipment.
a. Multiple responses were allowed for these questions.
b. These options were not listed in the March 2020 version of the survey.
c. ‘Other’ category included clinic/theatre space or equipment needed by another service, and staff being redeployed to other areas.
d. ‘Other’ category included patients being treated at a neighbouring clinic, and list length reduced to allow time for use of PPE and decontamination of facilities between patients.
Results
We are aware of 108 ECT clinics in existence in the four regions covered by this study; of those, 98 are members of ECTAS and were sent surveys to complete. In total, 95 clinics (97%) submitted responses to the survey in April 2020 and 89 (91%) in July 2020. Thus, our data cover 89% and 82% of all existing clinics at the two time points respectively.
The main findings are summarised in Table 1. Of 95 clinics, 84 (88%) were being adversely affected by the pandemic in April 2020: 50 (53%) were restricting ECT to the most urgent and/or severe cases and 22 (23%) were providing no service at all. By July, of 89 clinics, 69 (78%) were still affected, with 38 (43%) restricting cases and 8 (9%) remaining closed.
Additionally, the 364 patients who had had their treatment affected by the pandemic since 16 March 2020, including those who had had ECT withheld, had risen to 437 by July 2020. One clinic alone had had the treatment of 41 patients affected.
Discussion
Our survey shows that the vast majority of ECT services have been, and continue to be, adversely affected by the COVID-19 pandemic. Obstacles to delivery of ECT have been, and remain, various.
Anaesthetists and operating department practitioners were withdrawn from ECT lists to staff enlarged intensive care units (ICUs), despite most ICUs never having even neared capacity. This affected over half of the clinics at the beginning of the pandemic, with some still experiencing problems by July 2020, when the first peak of COVID-19 infections had long subsided.
Some ECT suites, with no means for adequate ventilation, have been unable to safely host a treatment that potentially involves AGPs. Even those suites that were adequately ventilated or have since been fitted with ventilation systems may continue to operate at reduced patient capacity. Many require patients to fully recover in treatment rooms owing to limited space for safe distancing between patients elsewhere and repurposing of recovery areas for doffing of personal protective equipment (PPE). Even in suites that retain separate recovery areas, the treatment room must be left fallow after any AGP for a set period before cleaning in preparation for the next patient. In some clinics this is as long as 30 min, depending on the frequency of air changes the room.
Treatment rooms require full cleaning between patients, and staff members spend a lot of time donning and doffing PPE. These necessities at best halve patient throughput.Reference Tor, Phu, Koh and Mok5 Some ECT services run from suites without adequate ventilation have instead delivered treatments in general hospital operating theatres,Reference Braithwaite, McKeown, Lawrence and Cramer6 which are subject not only to the restrictions listed above but also necessitate vying for time and facilities with surgical teams. Additionally, poor supply of PPE may have temporarily limited ECT provision in some hospitals.
The resultant loss of productivity has been devastating for many patients. It has led to services variously cancelling all ECT or prioritising only the sickest patients; some clinics have stopped out-patient treatment. Widespread cessation of continuation and maintenance ECT has led to recurrence of severe illness, and delays in initiating acute courses have resulted in worse patient outcomes, particularly in life-threatening illness. Admissions and even formal detentions in hospital have occurred or been lengthened as a consequence.
Recommendations
Looking to the near future, it is imperative that ECT services remain functional even if there is a second wave of COVID-19 infections this winter. Guidance published in September 2020 jointly by four anaesthesia organisations in the UK7 takes a pragmatic approach towards COVID-19 risk stratification that might prove helpful in increasing patient turnover. Crucially, it asserts that in-patients who are regularly tested for the virus and are on wards where COVID-19 patients are not being treated should be considered low risk. Previously only a small minority of out-patients who were shielding at home and regularly tested for the virus had been considered low risk. For treatment of low-risk patients, staff need wear only basic PPE (an apron, gloves and a surgical mask, with consideration of eye protection), usual recovery areas can be used and treatment rooms do not require full cleaning between patients.7
However, patients in medium- and high-risk groups will continue to present for ECT. Some clinics may require improvements in ventilation to facilitate faster throughput of such patients. It is essential that any shut-down clinics be reopened without delay, following liaison between infection control, anaesthesia and ECT staff. Psychiatric staff must work closely with anaesthesia colleagues to develop pathways enabling out-patients to access ECT, including regular fast-track virus testing.
It would be all too easy, with the benefit of hindsight, to criticise decisions made at the outset of the pandemic to redeploy anaesthetists, en masse, in anticipation of a surge in ICU usage of far greater magnitude than ultimately occurred. But it is important that the same situation does not recur and that staff are pulled from delivering ECT only if ICUs have a genuine need for the personnel and careful consideration of the balance of negative outcomes concludes that such action is unavoidable. PPE must be kept available. Lastly, the need to lengthen or widen ECT lists into afternoon sessions or on more days of the week must be seriously considered by healthcare providers, with job planning and prioritisation of staffing for ECT services made to facilitate this.
About the authors
Richard Braithwaite is a consultant psychiatrist with Isle of Wight NHS Trust, at St Mary's Hospital, Newport, Isle of Wight, and vice-chair of the Special Committee on Electroconvulsive Therapy and Related Treatments at the Royal College of Psychiatrists, London, UK. Robert Chaplin is Clinical Lead for Accreditation in the College Centre for Quality Improvement, Royal College of Psychiatrists, London, UK. Vimal Sivasanker is a consultant psychiatrist with Hertfordshire Partnership University NHS Foundation Trust, at Kingsley Green, Radlett, and chair of the Electroconvulsive Therapy Accreditation Service Advisory Group, Royal College of Psychiatrists, London, UK.
Data availability
The data that support the findings of this study are available from the corresponding author on reasonable request.
Acknowledgements
We thank Eve Blanchard and Sinead Rogers of the ECT Accreditation Service for organising and collating the results of the survey and Professor George Kirov for his suggestions regarding this paper.
Author contributions
R.B. analysed the data and wrote the initial draft manuscript. R.C. was involved in designing the study, wrote the draft abstract and revised the manuscript. V.S. was involved in designing the study and revised the manuscript. All authors gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors, but the survey was facilitated by employees of the Royal College of Psychiatrists, London.
Declaration of interest
None.


 Open access
Open access
eLetters
No eLetters have been published for this article.