



Introduction
There is general agreement that climate change will increase the frequency of extreme weather events (Morganstein & Ursano, Reference Morganstein and Ursano2020). Older persons may be particularly vulnerable to experiencing adverse health consequences from these (Gamble et al., Reference Gamble, Hurley, Schultz, Jaglom, Krishnan and Harris2013; Kwan & Walsh, Reference Kwan and Walsh2017; Leyva, Beaman, & Davidson, Reference Leyva, Beaman and Davidson2017; Parker et al., Reference Parker, Lie, Siskind, Martin-Khan, Raphael and Crompton2016; Walsh, Gibson, & Brown, Reference Walsh, Gibson and Brown2016). In June of 2013 a major river flood took place in Calgary – a city in southern Alberta with a population of approximately 1,300,000 located in the eastern foothills of the Canadian Rocky Mountains at the confluence of the Bow and Elbow Rivers (Calgary Economic Development, n.d.) – with water cresting between June 20 and 21. Environment Canada issued flood warnings early on June 20, while Calgary Emergency Management Agency (CEMA) declared a local state of emergency by mid-morning (Vroegop, Reference Vroegop2014). The disaster resulted in the partial or full evacuation of 26 neighbourhoods or communities in the vicinity of the Bow and Elbow Rivers and the entire downtown. These evacuations affected approximately 80,000 persons (Vroegop, Reference Vroegop2014), reflecting the disproportionate impact on those whose homes and businesses were in areas that flooded or were at risk of flooding. The 2013 flood was the second costliest natural disaster in Canadian history (Mamuji & Rozdilsky, Reference Mamuji and Rozdilsky2019), but there was only one reported fatality in Calgary (Teufel et al., Reference Teufel, Diro, Whan, Milrad, Jeong and Ganji2017; Vroegop, Reference Vroegop2014). The 2013 flood was a non-catastrophic natural disaster, as it caused minimal fatalities, localized but substantial property damage, and major economic disruption (Caldera, Wirasinghe, & Zanzotto, Reference Caldera, Wirasinghe and Zanzotto2016).
Relatively few longitudinal studies have reported on the health and well-being impacts of natural disasters on older adults. Much of the research done to date has focused on exposure to catastrophic events such as earthquakes and hurricanes (Heid, Pruchno, Cartwright, & Wilson-Genderson, Reference Heid, Pruchno, Cartwright and Wilson-Genderson2017; Pietrzak, Van Ness, Fried, Galea, & Norris, Reference Pietrzak, Van Ness, Fried, Galea and Norris2013) although the impact of floods has also been examined (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013; Zhen, Quan, & Zhou, Reference Zhen, Quan and Zhou2018). Older adults personally impacted by natural disasters of any type have been reported to experience more symptoms of post-traumatic stress disorder (PTSD) (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013; Heid et al., Reference Heid, Pruchno, Cartwright and Wilson-Genderson2017; Leyva et al., Reference Leyva, Beaman and Davidson2017; Morganstein & Ursano, Reference Morganstein and Ursano2020) and a statistically significant but relatively small increase in measures of both anxiety (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013; Leyva et al., Reference Leyva, Beaman and Davidson2017) and a depressed mood (Leyva et al., Reference Leyva, Beaman and Davidson2017). Exposure to flooding has been directly and indirectly (as a result of distress reactions and/or psychiatric disorders post-event) associated with sleep problems (Morganstein & Ursano, Reference Morganstein and Ursano2020; Zhen et al., Reference Zhen, Quan and Zhou2018). Sleep aid prescription rates were examined in the aftermath of the 2013 flood with no significant increase detected in Calgary (Sahni et al., Reference Sahni, Scott, Beliveau, Varughese, Dover and Talbot2016). Although life satisfaction can decrease after flooding, the general health of older adults appears unaffected (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013).
Older adults also exhibit resiliency to floods (Brockie & Miller, Reference Brockie and Miller2017; Leyva et al., Reference Leyva, Beaman and Davidson2017). Both social support (i.e., having access to supportive networks) (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013; Brockie & Miller, Reference Brockie and Miller2017; Heid et al., Reference Heid, Pruchno, Cartwright and Wilson-Genderson2017; Leyva et al., Reference Leyva, Beaman and Davidson2017) and income (Kwan & Walsh, Reference Kwan and Walsh2017; Walsh et al., Reference Walsh, Gibson and Brown2016; Wang & Yarnal, Reference Wang and Yarnal2012) can modulate this resiliency. Bei et al. (Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013) found that social support from individuals known to the person tended to be associated with better outcomes than when support was obtained from government or community agencies, which possibly either indicates greater need on the part of those requiring assistance from government and community agencies or gaps in the services provided to people not well supported by family and friends. Heid et al. (Reference Heid, Pruchno, Cartwright and Wilson-Genderson2017) found that social cohesion and trust within neighbourhoods, as a measure of collective efficacy, protected against PTSD following a flood event compared with social support offered by family and friends.
The Calgary flood occurred during the baseline data collection (July 2012 – June 2015) from Calgary participants in the Canadian Longitudinal Study on Aging (CLSA) (Raina et al., Reference Raina, Wolfson, Kirkland, Griffith, Balion and Cossette2019). This timing offered a unique opportunity to explore the impact of exposure to a non-catastrophic natural disaster (Caldera et al., Reference Caldera, Wirasinghe and Zanzotto2016), on middle-aged and older persons by utilizing the comprehensive, yet not specifically designed for this purpose, data collected on CLSA participants. The timing would also provide the possibility of evaluating non-obvious (i.e., something other than temporary cessation of data collection during local states of emergency) effects of an external event such as a major flood on data collected in a longitudinal study. The goal of this study was to determine whether there was a detectable signal of the event at a group level using a pre-/post-flood design (please note that individual study participants were not seen both before and immediately after the flood) on the specific health and perceived well-being outcomes discussed. We predefined a detectable signal as a statistically significant difference in a post-flood outcome between exposed (i.e., evacuated) and non-exposed (i.e., not evacuated) CLSA participants while acknowledging that this was dependent on the comparability of the two groups on other characteristics. We compared data provided by CLSA participants seen during the 6 months prior to and following the flood and also contrasted those from evacuated and non-evacuated communities as a proxy for likely direct flood impact.
Method
Study Design and General Methodological Items
This study is a secondary analysis of data collected during the baseline cycle of the CLSA from study participants residing in Calgary, a city of approximately 1,300,000 people located in the Canadian Province of Alberta. Ethics approval was obtained from the University of Calgary’s Conjoint Health Research Ethics Board (REB18–2130).
The CLSA is a national voluntary prospective cohort study on aging. At the time of recruitment, participants were between 45 and 85 years of age. Baseline data collection in Calgary began in the summer of 2012. Consenting participants agree to undergo data collection every 3 years for at least 20 years or until death. Different sampling designs used to recruit participants will be summarized subsequently, and are described in detail elsewhere (Kirkland et al., Reference Kirkland, Griffith, Menec, Wister, Payette and Wolfson2015; Raina, Wolfson, & Kirkland, Reference Raina, Wolfson and Kirkland2008).
CLSA participants are either in a national tracking or a comprehensive cohort. The national tracking cohort consists of 21,241 representative participants from across Canada. Their data is obtained through computer-assisted telephone interviews. The comprehensive cohort consists of 30,097 participants living within a 25–50 km radius of one of 11 data collection sites (DCS) situated across Canada, including one in Calgary. Participants in the comprehensive cohort undergo an in-home interview followed by a visit to their local DCS where additional data (questionnaires, cognitive testing, physical measures) are obtained and biological samples are collected. The data collected during the in-home and DCS visits do not overlap. Nationally, participants in the comprehensive cohort were recruited using either random digital dialing (as for all Calgary participants) or provincial health registries. Recruitment of the comprehensive cohort began in early 2012 and was ongoing during the time period of this study. Potential comprehensive participants were excluded if they could not speak or write in English (required for Calgary participants) or French, were living in an institution, were unable to provide informed consent at the time of enrollment, or were a full-time member of the Canadian Armed Forces.
This study was restricted to CLSA comprehensive participants residing at the time of recruitment within the borders of the City of Calgary (defined as Calgary Census Subdivision UID 4806016). Participants in the CLSA tracking cohort residing in Calgary were not included, as some of measures selected for our analyses were not collected on them. A total of 109 (3.7%) of the 2,956 Calgary comprehensive participants were excluded because their residence fell outside of the City of Calgary municipal limits.
The 2013 Calgary flood led to the closure of the local DCS from June 21 to June 26, 2013, although in-home interviews were conducted during this period in unaffected neighbourhoods.
Specific Methodological Items
Flood-related data collection dates
Participants were divided into those whose data were collected before or after June 20, 2013, which was the date when Calgary declared a state of emergency. The pre-flood group consisted of participants whose data were collected during the 6 months before the flood, whereas the post-flood group had their data collected during the 6 months after. We chose a 6-month time frame to be comparable with other studies examining the impact of floods, to ensure that the groups formed were large enough to protect the anonymity of local CLSA participants, and to increase the statistical power of our analyses. A time period of 4–6 months after flooding had been used for data collection in a number of similar studies (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013; Chen & Liu, Reference Chen and Liu2015; Hetherington, McDonald, Wu, & Tough, Reference Hetherington, McDonald, Wu and Tough2018), although it should be noted that Parker et al. (Reference Parker, Lie, Siskind, Martin-Khan, Raphael and Crompton2016) emphasized that there may be a 6-month delay between a traumatic event and the diagnosis of PTSD. The 2013 flood was an acute ecological disaster. We assumed that the post-flood effects we were looking for would have become evident within 6 months of the event (Morganstein & Ursano, Reference Morganstein and Ursano2020). Any data collected on June 20, 2013 (i.e., six in-home interviews and seven DCS visits) were allocated to the post-flood period.
The specific measures examined were collected either during the in-home interview or the DCS visit of the participant. In-home interviews and DCS visits are completed on different dates, typically several weeks apart. Based on the relationship to the flood date, we categorized the collection of data as follows: in-home visit pre-flood (n = 438), in-home visit post-flood (n = 415), DCS visit pre-flood (n = 405), and DCS visit post-flood (n = 421). This meant that for a small number of participants, data provided by some individuals could be included in the pre-flood grouping for some analyses but in the post-flood grouping for others if their in-home appointment happened prior to the flood but their DCS appointment took place afterwards.
Evacuated communities
We used forward sortation area (FSA) designations to allocate the residences of CLSA participants to Calgary communities. Evacuation status was determined by whether participants’ primary residences were in communities that received a mandatory evacuation order. These participants were considered directly exposed to flooding. The communities that received a mandatory evacuation order were Beltline, Bonnybrook, Bowness, Bridgeland Industrial, Chinatown Eau Claire, Cliff Bungalow, Deer Run, Discovery Ridge, Douglasdale, Downtown East Village, Elboya, Elbow Park, Erlton, Hillhurst, Inglewood, Mission, Montgomery, Quarry Park, Rideau, Riverbend, Riverdale, Roxboro, Sunnyside, Victoria Park, Westmount/ Hillhurst, and Windsor Park (Alberta Emergency Alert, 2013).
Outcomes
The outcomes selected were based on our review of the literature for likely sensitive markers of the psychological and behavioural effects of an ecological disaster (Morganstein & Ursano, Reference Morganstein and Ursano2020) followed by determination if the required data were available, as the CLSA was not specifically designed to assess the impact of events of this nature. We chose the following characteristics as our primary outcomes: symptoms of PTSD, depressive symptoms, diagnosed anxiety disorder, self-rated mental health, self-rated general health, and self-rated sleep satisfaction. PTSD symptoms were assessed using the four-item Primary Care Post-Traumatic Stress Disorder (PC-PTSD) screening instrument (Prins et al., Reference Prins, Ouimette, Kimerling, Cameron, Hugelshofer and Shaw-Hegwer2003). Positive responses on three or more of the items indicate that PTSD is present. Depressive symptoms were assessed using the 10-item Center for Epidemiological Studies Short Depression (CESD-10) scale (Andresen, Malmgren, Carter, & Patrick, Reference Andresen, Malmgren, Carter and Patrick1993). A score of 10 or more out of a maximum of 30 indicates a positive screen for depression. Anxiety was assessed by self-report of receiving a diagnosis of an anxiety disorder by a physician. Participants were asked, “Has a doctor ever told you that you have an anxiety disorder such as a phobia, obsessive-compulsive disorder or a panic disorder?”. “Yes” responses were taken as indicating an anxiety disorder. Mental health, general health, and satisfaction with current sleep pattern were self-reported using Likert scales in response to questions such as, “How satisfied or dissatisfied are you with your current sleep pattern?”. These were re-coded into binary categories for regression analyses. For mental and general health, “fair” and “poor” responses were coded as indicating a “low” or “worse” status. Others have used a similar approach (Stinchcombe, Wilson, Kortes-Miller, Chambers, & Weaver, Reference Stinchcombe, Wilson, Kortes-Miller, Chambers and Weaver2018). We coded “dissatisfied” and “very dissatisfied” responses as “low” or “poor” for satisfaction with current sleep pattern. Nicholson et al. (Reference Nicholson, Rodrigues, Anderson, Wilk, Guaiana and Stranges2020) used a similar approach.
Additional outcomes that we examined were life satisfaction and functional social support. The former was assessed with the Satisfaction with Life Scale (SWLS) which is a five-item instrument (Diener, Emmons, Larsen, & Griffin, Reference Diener, Emmons, Larsen and Griffin1985), while functional social support scale was assessed with the 19-item Medical Outcomes Study (MOS) Social Support Survey (Sherbourne & Stewart, Reference Sherbourne and Stewart1991). These measures were re-coded into binary categories for regression analyses. Overall satisfaction with life was assessed using a score derivation with a higher score indicating higher satisfaction with life (min: 5, max: 35). A SWLS score of 20 has been used as the midpoint between satisfied and dissatisfied (Jacobsson & Lexell, Reference Jacobsson and Lexell2016). Scores below 20 were coded as “lower” or “worse” life satisfaction. This included those with slightly dissatisfied (score 15–19), dissatisfied (score 10–14), and extremely dissatisfied (score ≤ 10) ratings. Unlike other studies, we were unable to differentiate formal from informal social support, as this information was not captured. Scores for overall social support (formal and informal) ranged from 0 to 100, with higher scores indicating greater social support. We dichotomized the data using a median split as scores were skewed towards higher values. This led to scores lower than 82.9 being coded as “lower” or “worse”.
Data on PTSD symptoms, self-rated mental, and general health status, and both the sleep and life satisfaction measures were collected during the in-home interview. The date of the in-home interview was used to assign participants into the pre- or post-flood groups. Information on depressive symptoms, presence of an anxiety disorder, and functional social support were collected during the DCS visit. We used the date of this visit to allocate participants to the pre- and post-flood groups for the analyses of these variables. Responses of “refused”, “required question was not answered”, “at least one required question was not answered”, and “don’t know/no answer” were re-coded as missing data and excluded from all analyses.
Socio-demographic characteristics
We compared participants in the pre-/post-flood groups and evacuated/not evacuated communities on the following selected characteristics: age (45–64 years or 65–85 years), sex (female or male), marital status (married/common-law or single, divorced, widowed), race/cultural background (white or other), ownership of dwelling (own or rent/other arrangement), total household income (< $50,000 CAD or ≥ $50,000 CAD), education (less than post-secondary vs. completed post-secondary or higher), and living alone (yes or no). Participant responses of “refused”, “required question was not answered”, and “don’t know/no answer” responses were re-coded as missing and were excluded from all analyses.
Statistical Analysis
Descriptive statistics examining socio-demographic factors were used to create group profiles for those seen during the 6 months pre-flood and those seen over the 6 months post-flood. This was also done for CLSA participants from evacuated and non-evacuated communities. To test for statistical significance, chi-square testing with Yates continuity corrections was done for categorical data. We did not correct for multiple comparisons because of the exploratory nature of study and the large number of comparisons being made (Bender & Lange, Reference Bender and Lange2001). No weight factors were applied to the CLSA measures presented in this study. The authors have confirmed in other work with the data set that unweighted CLSA baseline data is representative of the local population for the socio-demographic factors that were considered (unpublished data, available upon request).
For each of the eight outcomes (PTSD and depressive symptoms, diagnosed anxiety disorder, self-rated mental health, self-rated general health, sleep satisfaction, life satisfaction, and functional social support) a logistic regression model was built using community (evacuated or non-evacuated) as the exposure to the flood event while controlling for age, sex, total household income, and living alone (only the latter two characteristics were found to show a statistically significant difference between participants from evacuated and those from non-evacuated communities). To retain as much power as possible in the analyses, the number of factors controlled for were limited. Beyond age and sex, we were particularly interested in the potential protective effect of higher income (Kwan & Walsh, Reference Kwan and Walsh2017; Walsh et al., Reference Walsh, Gibson and Brown2016; Wang & Yarnal, Reference Wang and Yarnal2012) and the potential risk of living alone (Wang & Yarnal, Reference Wang and Yarnal2012). Although marital status may also be a protective factor (Kwan & Walsh, Reference Kwan and Walsh2017; Wang & Yarnal, Reference Wang and Yarnal2012), we felt that the living alone variable was likely highly related and an adequate proxy. Logistic regression was chosen because some outcome variables were binary. These logistic regression models involved stratified analysis by data collection date. All analyses were conducted in IBM SPSS v.25.0.
Results
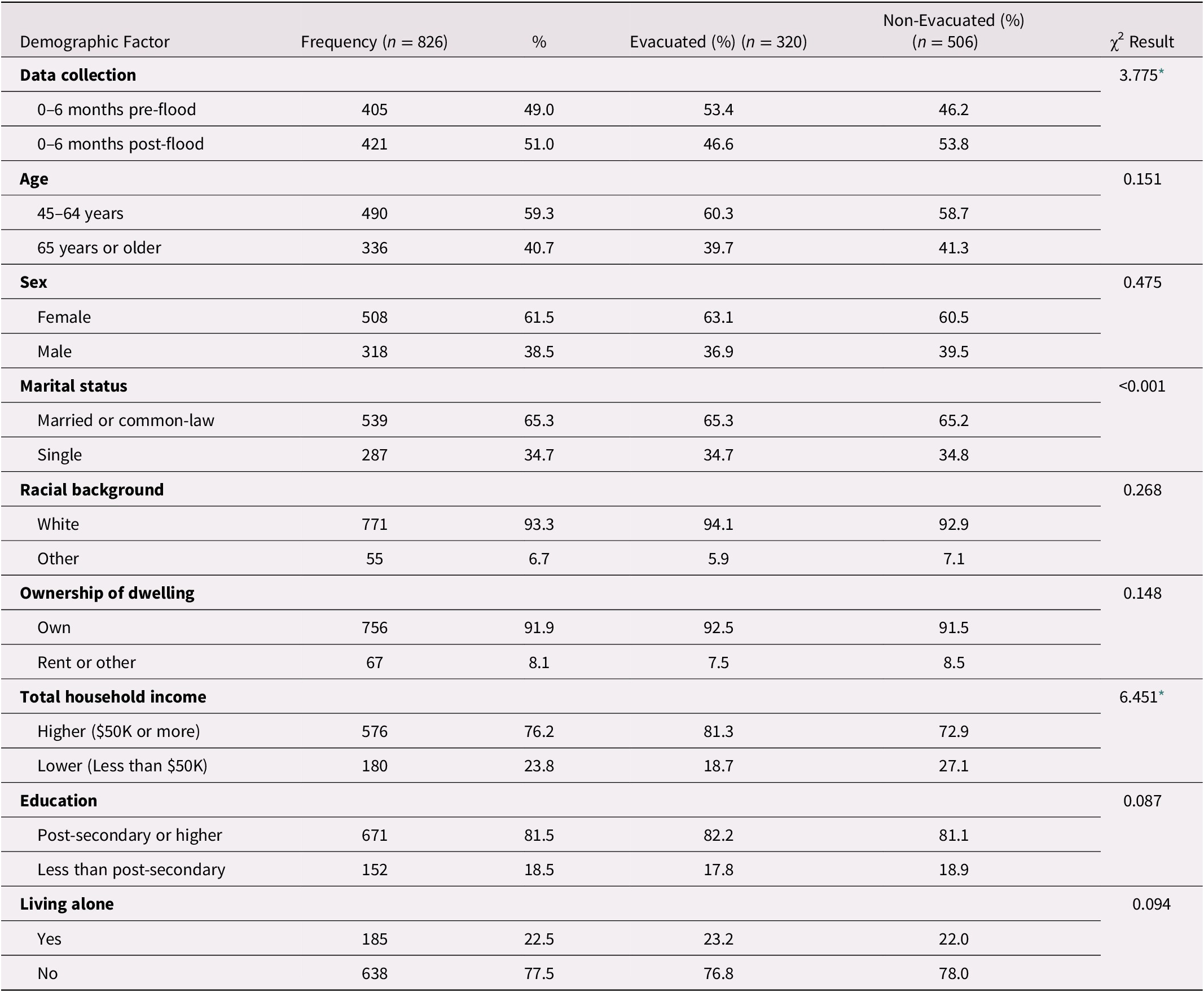
Table 1 provides a comparison of pre- and post-flood groupings of CLSA participants based on the time of their DCS visit. Analyses based on the time of in-home interviews yielded similar results (data not shown). Overall, CLSA participants were predominantly white with a relatively high socio-economic status (SES), based on factors such as total household income, proportion with post-secondary education, and home ownership. Post-flood participants were significantly more likely to be living alone (p < 0.05) and significantly less likely to be living in evacuated communities (p < 0.05).
Table 1. Comparison of socio-demographic characteristics of CLSA participants pre- and post-flood based on timing of data collection site (DCS) visit

Note. Chi-square test for independence with Yates Continuity Correction.
* p < 0.05.
Table 2 compares CLSA participants from evacuated versus non-evacuated communities as determined by the date of their DCS visits (data based on the date of in-home visits were similar and are not shown). Participants from the evacuated communities had significantly higher total household incomes (p < 0.05) than those from non-evacuated areas. In accord with the observation that post-flood participants were less likely to be from evacuated communities, there were significantly fewer participants from evacuated areas with DCS visits post-flood (p < 0.05).
Table 2. Comparison of socio-demographic characteristics of evacuated and non-evacuated CLSA participants based on date of data collection site (DCS) visit
Note. Chi-square test for independence with Yates Continuity Correction.
* p < 0.05.
There were no statistically significant differences in the relative proportions of CLSA participants pre- and post-flood experiencing three or more PTSD symptoms (5.0% pre-flood vs. 4.6% post-flood), fair or poor self-rated mental health (5.5% vs. 5.8%), fair or poor self-rated general health (11.2% vs. 8.9%), dissatisfaction with sleep (27.9% vs. 30.2%), lower level of life satisfaction (10.6% vs. 14.9%), significant depressive symptoms (14.4% vs. 15.6%), diagnosed anxiety disorder (5.7% vs. 5.2%), and lower levels of functional support (45.9% vs. 49.9%).
After adjusting for socio-demographic covariates (age, sex, total household income, living alone), those living in evacuated areas pre-flood were significantly less likely to report a diagnosis of an anxiety disorder (odds ratio [OR] = 0.284 [0.092,0.879] p = 0.029) (Table 3). Post-flood, this statistically significant difference disappeared (OR = 0.833 [0.304, 2.284], p = 0.723). This was explained by an increase in the prevalence of anxiety disorders among respondents in evacuated communities (from 2.4% pre-flood to 4.7% post-flood) and a decline among those in non-evacuated communities (from 8.1% pre-flood to 5.5% post-flood), see Table 4.
Table 3. Adjusted odds ratios comparing evacuated to non-evacuated CLSA participants for negative health and mental health outcomes pre- versus post-flood
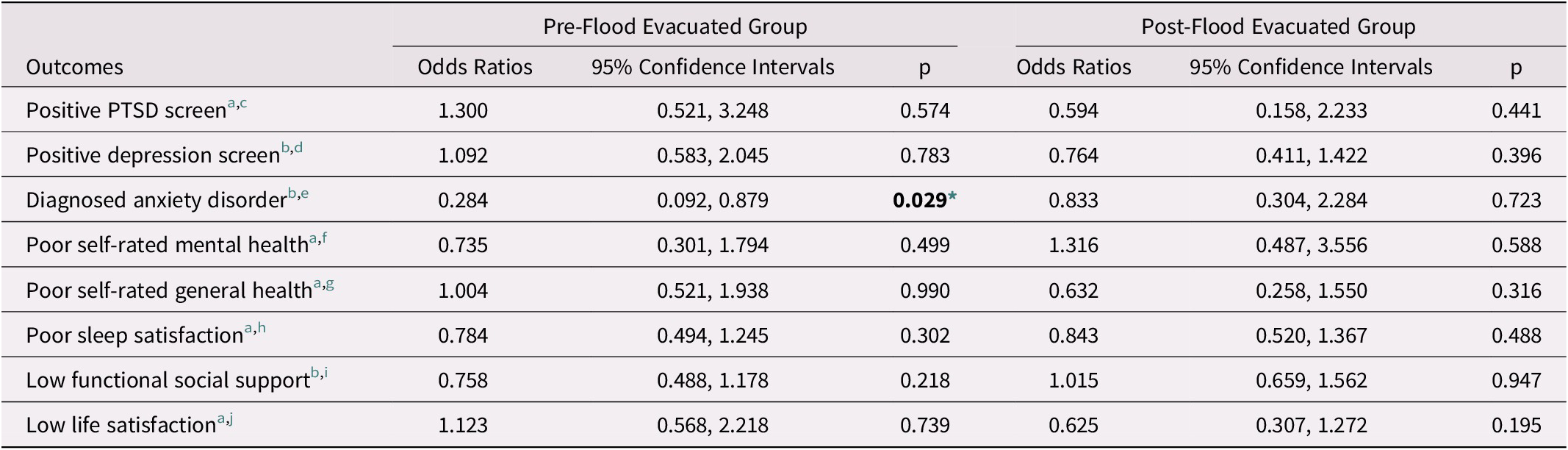
Note. Findings adjusted for age, sex, total household income, and living alone.
Bolding references a statistically significant finding (p < 0.05). *p < 0.05
a Data collected through the in-home questionnaire.
b Data collected through the data collection site visit questionnaire.
c Reference category is negative depression screen.
d Reference category is good self-rated mental health.
e Reference category is good self-rated general health.
f Reference category is good sleep satisfaction.
g Reference category is high functional social support.
h Reference category is high life satisfaction.
i Reference category is negative PTSD screen.
j Reference category is no diagnosed anxiety disorder.
Table 4. Prevalence of negative health and mental health outcomes among evacuated and non-evacuated CLSA participants pre- versus post-flood
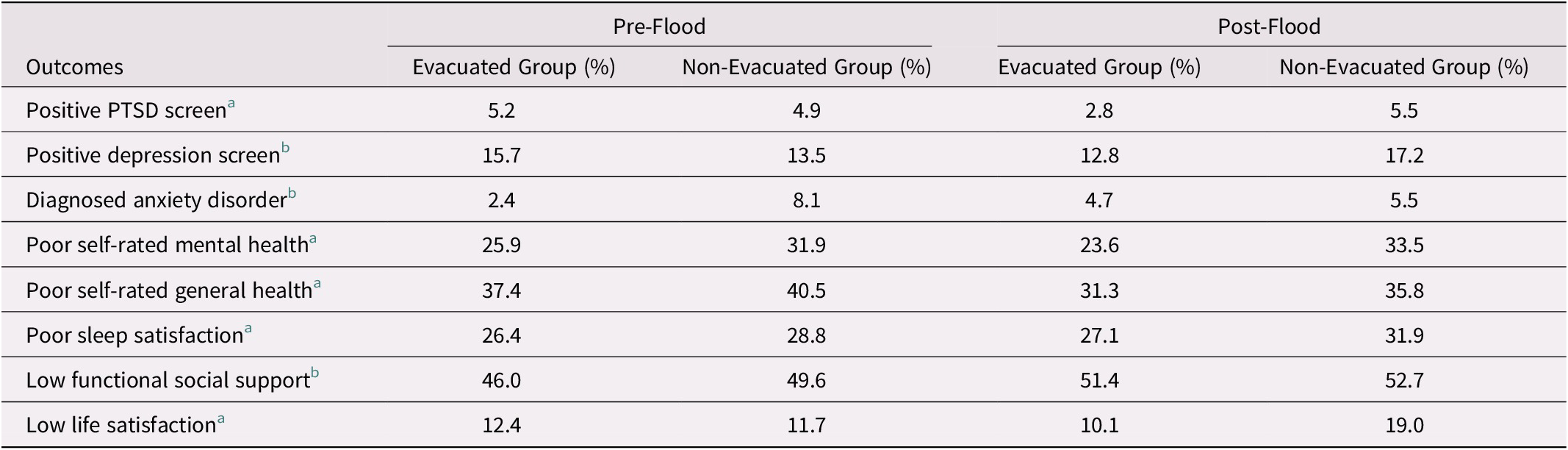
Note.
a Data collected through the in-home questionnaire.
b Data collected through the data collection site visit questionnaire.
As for the other outcomes examined, no statistically significant differences in the group comparisons were found. Those from evacuated areas interviewed pre-flood were less likely than participants from non-evacuated neighborhoods to report poor self-rated mental health, poor sleep satisfaction, and low functional support but more likely to report three or more PTSD symptoms, have a positive screen for depression, poor self-rated general health, and low life satisfaction, although none of these differences achieved statistical significance (p < 0.05). Compared with those from non-evacuated communities, participants from evacuated areas post-flood had non-statistically significant lower odds of having three or more PTSD symptoms, a positive screen for depression, poor self-rated general health, poor sleep satisfaction, and reduced life satisfaction post-flood, while they showed non-statistically significant higher likelihoods of reporting lower self-rated mental health and lower functional social support following the flood.
Higher total household income, living alone, and sex had statistically significant associations with a number of the examined outcomes while controlling for neighborhood evacuation status, age, sex, income, and living alone (see Table 5). For the pre-flood group, respondents with a higher total household income had reduced risks of a positive screen for depression (p = 0.015) or of reporting lower functional social support (p = 0.031). Living alone pre-flood significantly increased the risks of reporting both lower life satisfaction (p = 0.006) and lower functional social support (p < 0.001). For the post-flood group, a higher total household income significantly reduced the risk of having three or more PTSD symptoms (p = 0.035), worse self-rated mental health (p = 0.029), and lower life satisfaction (p = 0.009). Living alone post-flood increased the risk of reporting lower functional social support (p = 0.001), while being female decreased this risk (p = 0.008).
Table 5. Adjusted odds ratios for significant socio-demographic characteristics and negative health and mental health outcomes pre- versus post-flood
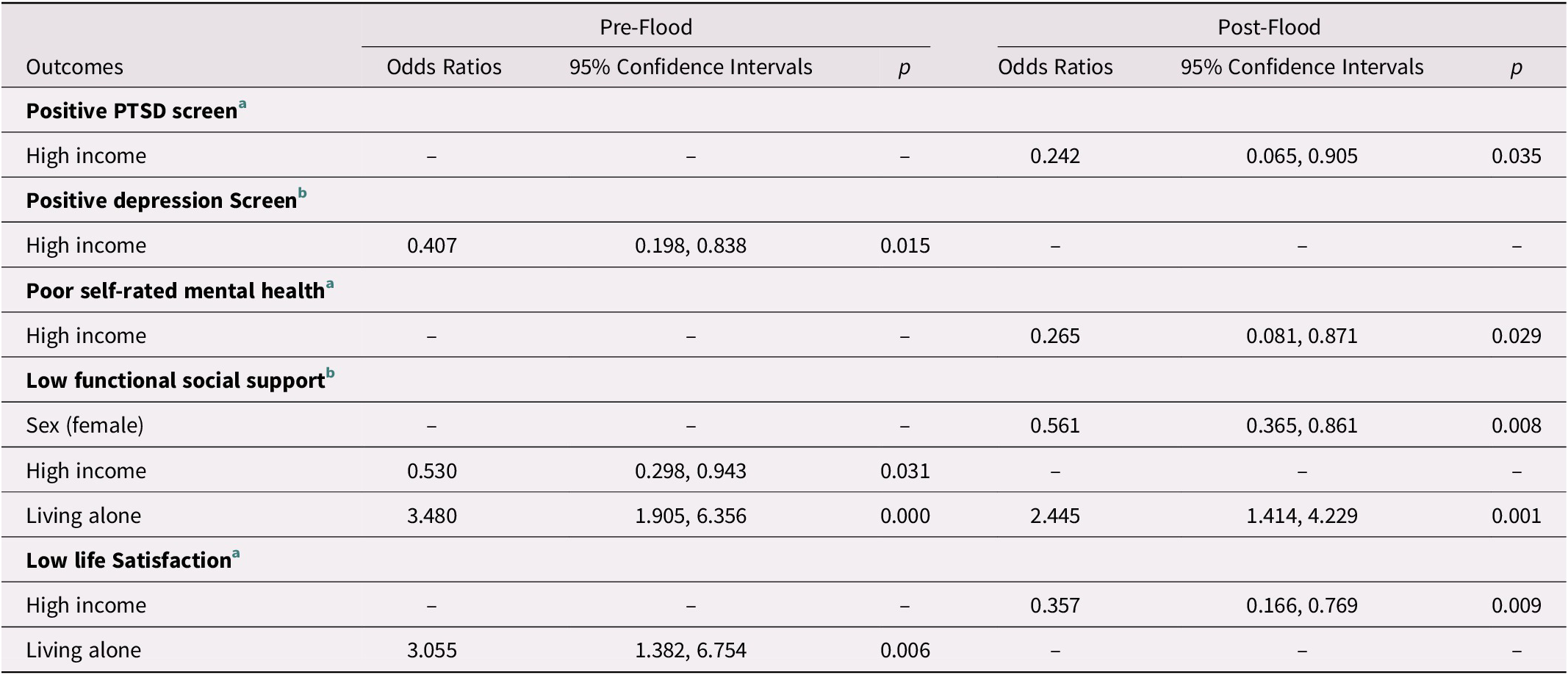
Note. Findings adjusted for evacuation status, age, sex, total household income, and living alone.
a Data collected through the in-home questionnaire.
b Data collected through the data collection site visit questionnaire.
Discussion
Our objectives were to determine whether we could discern any statistically significant group-level impacts of a major but non-catastrophic flood on the health and well-being of CLSA participants living in Calgary. The 2013 Calgary flood had a distinct geographic patterning, with some city neighbourhoods being directly affected and evacuated while others were not. We compared data from participants seen before and after the flood as well as those who lived in evacuated versus non-evacuated communities. We found no statistically significant flood impact on the outcomes assessed. Considering the components of the often-used Haddon matrix (Haddon, Reference Haddon1970; Morganstein & Ursano, Reference Morganstein and Ursano2020) that account for the host, agent/vector, and environment across pre-event, event, and post-event time periods, this finding may not be viewed as surprising. For example, although the Calgary flood was a major local emergency, it was not a catastrophic one with numerous fatalities. Also, Calgary overall had a relatively good pre-event profile of factors noted to impact the ability of a community to withstand an ecological disaster (Morganstein & Ursano, Reference Morganstein and Ursano2020) and the response to it was viewed favorably by the citizens of the municipality (Vroegop, Reference Vroegop2014). An acknowledged limitation (discussed further) was our inability to examine pre- and post-flood data on individual participants (i.e., we could only look for group differences).
Our inability to find statistically significant differences at a group level could be explained by insufficient power, imprecise measure of flood impact (i.e., the personal disruption from the flood could not be discerned with confidence using community as our smallest geographical unit), insensitive measures of the outcomes of interest (the methods and measures of the CLSA were not chosen to address the impact of an ecological disaster), and baseline differences in the characteristics of evacuated and non-evacuated neighbourhoods. Regarding the latter, evacuated and non-evacuated communities were not well matched on a number of characteristics. CLSA participants from evacuated communities were significantly more likely to report higher household incomes and less likely to have a diagnosed anxiety disorder pre-flood in adjusted analyses. This may have detracted from our ability to detect a flood impact. High income has previously been found to predict resiliency following natural disasters (Kwan & Walsh, Reference Kwan and Walsh2017; Walsh et al., Reference Walsh, Gibson and Brown2016; Wang & Yarnal, Reference Wang and Yarnal2012). In our study, higher income was significantly associated with lower odds of a positive screen for depression. Participants with higher income were also significantly less likely to have three or more PTSD symptoms, poor self-rated mental health, and low life satisfaction post-flood (p < 0.05). Wang and Yarnal (Reference Wang and Yarnal2012) found that a measure of social vulnerability, which included low income, was associated with greater overall vulnerability to floods. Walsh et al. (Reference Walsh, Gibson and Brown2016) has suggested that money provides “peace of mind”.
Two other studies have reported on the mental health effects of the 2013 Calgary flood. Among individuals providing data pre- and post-flood, Hetherington et al. (Reference Hetherington, McDonald, Wu and Tough2018) found that both living in a directly impacted community and having higher anxiety levels pre-flood, regardless of geographic location, were associated with a higher likelihood of PTSD post-flood. Using regional health surveillance data, Sahni et al. (Reference Sahni, Scott, Beliveau, Varughese, Dover and Talbot2016) found no increase in new prescriptions for anti-anxiety medications, sleep aids, or anti-depressants post-flood in Calgary, but among women in High River (a southern Alberta community 40 km south of Calgary that was more severely affected by flooding) there were significant increases in the use of both anxiety medications and sleep aids in the 6 weeks after the flood. Our findings tend to corroborate the apparent lack of measurable impact of the 2013 flood on collective levels of anxiety within Calgary, although there was a suggestion that levels of anxiety may have increased relatively among persons living within evacuated communities. Evidence of increased anxiety has been reported in some (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013; Leyva et al., Reference Leyva, Beaman and Davidson2017) but not all studies of the effects of floods (Sahni et al., Reference Sahni, Scott, Beliveau, Varughese, Dover and Talbot2016).
Social support has also been associated with resiliency to natural disasters (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013; Brockie & Miller, Reference Brockie and Miller2017; Heid et al., Reference Heid, Pruchno, Cartwright and Wilson-Genderson2017; Leyva et al., Reference Leyva, Beaman and Davidson2017). Living alone was the only characteristic in our models that significantly increased the odds of reporting lower functional social support among CLSA participants both pre- and post-flood. It was also significantly associated with lower life satisfaction prior to the flood.
Our finding of stable self-reported general health after the flood is consistent with Bei et al. (Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013), who also found that overall physical health seemed unaffected by flooding. In the study by Sahni et al. (Reference Sahni, Scott, Beliveau, Varughese, Dover and Talbot2016) mentioned previously, there were significant increases in injuries and sexual assaults detected by emergency department visits after the flood among Calgary residents. Likewise, we observed no overall statistically significant changes in life satisfaction or functional social support, although a prior study found significantly decreased satisfaction with life after flooding (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013).
Overall, the results of our study suggest that middle-aged to older persons may possess greater resiliency to major flooding than had been suggested in previous research (Gamble et al., Reference Gamble, Hurley, Schultz, Jaglom, Krishnan and Harris2013; Kwan & Walsh, Reference Kwan and Walsh2017; Leyva et al., Reference Leyva, Beaman and Davidson2017; Parker et al., Reference Parker, Lie, Siskind, Martin-Khan, Raphael and Crompton2016; Walsh et al., Reference Walsh, Gibson and Brown2016). In a small number of studies, evidence was found that older adults cope well following natural disasters, possibly by drawing upon more extensive life experience and embedded social networks (Brockie & Miller, Reference Brockie and Miller2017; Leyva et al., Reference Leyva, Beaman and Davidson2017). Again, it is important to note that our study’s sample of middle-to-older aged persons had a relatively high SES, which may have influenced our findings.
Strengths and Limitations
Ours is the first study of the 2013 Calgary flood to focus on the distress reaction and psychiatric disorder impacts for middle-aged and older adults, who may be particularly vulnerable to natural disasters (Gamble et al., Reference Gamble, Hurley, Schultz, Jaglom, Krishnan and Harris2013; Kwan & Walsh, Reference Kwan and Walsh2017; Leyva et al., Reference Leyva, Beaman and Davidson2017; Parker et al., Reference Parker, Lie, Siskind, Martin-Khan, Raphael and Crompton2016; Walsh et al., Reference Walsh, Gibson and Brown2016). Our study also considered the potential impact of unanticipated events of this nature on the data collected during longitudinal studies. Aside from short-term suspension of DCS visits, we did not find evidence of a significant impact of the flood on Calgary-based data collection other than possibly having more trouble recruiting participants from evacuated neighborhoods (see following paragraph). Longitudinal study data could still be affected by more severe and/or different types of disruptions, as has happened with the COVID-19 pandemic. The impact would be influenced by the characteristics of the study population, the nature of the event, and the specifics of the community where it occurs before, during, and after its occurrence.
An unexpected finding was that post-flood CLSA participants were less likely to be from evacuated communities. Random digit dialing to land lines was used to recruit Calgary participants (Canadian Longitudinal Study on Aging, 2017). Recruitment efforts continued throughout the period covered in this study. It is possible that the flood may have had an impact on recruitment. Potentially eligible individuals evacuated from their homes and/or residing outside of them post-event while repair work was underway would not have had access to their land line. Even if contacted, they may have not been inclined to volunteer because of other more pressing demands. One could reasonably speculate that this would preferentially affect those most impacted by the flood. This may have introduced unintended recruitment bias into our study, with those more severely affected by the flood disproportionally lost to enrollment during the time period we considered (i.e., up to 6 months post-flood). It is another possible explanation for our inability to detect differences between those participants who were exposed to the flood and those who were not exposed. Other studies have detected group-level deleterious effects among participants impacted by non-catastrophic natural disasters (Bei et al., Reference Bei, Bryant, Gilson, Koh, Gibson and Komiti2013; Heid et al., Reference Heid, Pruchno, Cartwright and Wilson-Genderson2017; Leyva et al., Reference Leyva, Beaman and Davidson2017; Zhen et al., Reference Zhen, Quan and Zhou2018).
Other limitations have already been noted. There were baseline differences between evacuated and non-evacuated neighborhoods. We were not able to compare pre-/post-flood measures on individual CLSA participants, which limited us to looking for group-level differences in the outcomes examined. As a proxy for the extent of exposure to and therefore the impact of the flood, we used community evacuation status, but did not know if participants in fact evacuated from their homes, were exposed to actual flooding, or were otherwise impacted by flooding. Specific measures of distress reactions, psychiatric disorders, and health risk behaviours may have been more sensitive in detecting an impact, but we were limited to the CLSA data that were collected. The prevalences found for a number of the outcomes examined (three or more PTSD symptoms, fair to poor self-rated mental health, diagnosed anxiety disorder) were low, meaning that our study was likely underpowered for detecting relevant impacts on these characteristics.
These and other limitations may account for our inability to demonstrate a statistically significant impact on the outcomes examined from the 2013 Calgary flood and may also explain differences between our findings and the prior literature. Our study design and methods could be adapted and refined to evaluate the impacts of future natural disasters on aging populations and on the data collected during longitudinal studies. Although flood studies typically employ cross-sectional designs, longitudinal study designs may offer greater opportunities to explore how people cope with flood experiences and reconstruct their lives (Hudson, Thieken, & Bubeck, Reference Hudson, Thieken and Bubeck2020).
Conclusion
The frequency of extreme weather events such as floods is expected to increase. Our study examined the mental and physical health impacts of a major river flood on Calgary-based CLSA participants. Overall, the flood had no significant relationship with the outcomes examined in our cohort at a group level. Higher income (≥ $50,000) was a protective factor for several potential adverse outcomes. Our findings add to the literature on the resilience of older adults to events such as major flooding, and suggest the complexity of vulnerability and resiliency to such events. The relationship between natural disasters and negative mental and physical health outcomes may be difficult to demonstrate in studies that were not designed to do this; however, catastrophic events do have the potential to influence the data being collected in research studies in ways that must be considered during the analysis of this data.
Acknowledgements
This research was made possible using the data/biospecimens collected by the CLSA. Funding for the CLSA is provided by the Government of Canada through the Canadian Institutes of Health Research (CIHR) under grant reference LSA 94473 and the Canada Foundation for Innovation. This research has been conducted using the CLSA Baseline Comprehensive Data Set version 4.0, under Application Number 180905. The CLSA is led by Drs. Parminder Raina, Christina Wolfson, and Susan Kirkland. S.J.N. received funding from the Brenda Strafford Centre on Aging at the University of Calgary. The authors thank Anita Blackstaffe for providing valuable assistance. This research was funded with operating funds belonging to the Brenda Strafford Centre on Aging at the University of Calgary. Data are available from the CLSA (www.clsa-elcv.ca) for researchers who meet the criteria for access to de-identified CLSA data.
Author contributions
A.M.T. and D.B.H. developed the research objectives and design. S.J.N. led the analysis of the data. All authors contributed to interpreting the data and drafting and revising the manuscript, and all authors approved the submitted manuscript.
Disclosure
The opinions expressed in this manuscript are those of the authors and do not reflect the views of the Canadian Longitudinal Study on Aging (CLSA).





