



It is estimated that globally 463 million adults are living with diabetes, which represents 9·3 % of the world’s population(1). Type 2 diabetes (T2D) disproportionately affects populations of Black African ancestry(Reference Pham, Carpenter and Morris2,Reference Goff3,4) . In both the USA and UK, where people of Black African ancestry form significant minority groups, T2D is estimated to be three times more prevalent than in White ethnic groups(5,6) . Furthermore, it is projected that the African continent will experience the greatest increase in T2D prevalence over the next two decades(1). Overweight and obesity has a significant association with incident T2D(4,Reference Mokdad, Ford and Bowman7) . Populations of Black African ancestry are most likely out of all ethnic groups to be overweight or obese(8,Reference El-Sayed, Scarborough and Galea9,10) , making it a main driving force in the difference in diabetes rates amongst these communities compared with White ethnic groups. Diabetes-related complications include kidney failure, non-traumatic lower-limb amputations, blindness among adults, heart disease and stroke and have been associated with worse quality of life(Reference Cannon, Handelsman and Heile11). In the USA, communities of Black African ancestry not only bear a disproportionate burden of developing T2D but they are also twice as likely to experience diabetes-related blindness, 2·3 times more likely to experience lower limb amputations, 3·5 times more likely to have kidney disease(8) and it is the fourth leading cause of death(Reference Goode12).
The burden of T2D and its associated complications occur as a result of prolonged elevations in blood glucose levels, which often occur as a result of poor self-management(Reference Goode12). The higher prevalence of complications seen in populations of Black African ancestry can be associated with poorer rates of disease management, as demonstrated by a 5-year longitudinal study finding that African-Americans spent fewer days engaging in self-care activities compared with White participants(Reference Trief, Izquierdo and Eimicke13). Engaging in self-care behaviours (e.g. self-monitoring blood glucose levels, participating in physical activity) plays an important role in the prevention of T2D risk factors(Reference Powers, Bardsley and Cypress14) as well as the management of disease and its complications. Diabetes self-management education intervention trials conducted in largely White ethnic groups have been shown to be effective at reducing glycated haemoglobin (HbA1c) and fasting blood glucose for up to 12 months(Reference Steinsbekk, Rygg and Lisulo15,Reference Gary, Genkinger and Guallar16) . However, a 2018 meta-analysis examining diabetes self-management education specifically in populations of Black African ancestry found no effect on HbA1c in these populations(Reference Cunningham, Crittendon and White17). This is perhaps due to inadequate matching of interventions to specific cultural barriers and needs such as historical barriers of racism, communication needs (e.g. language/literacy), low socio-economic status, high levels of food insecurity and limited access to safe areas and healthcare(Reference Gaskin, Thorpe and McGinty18).
Cultural tailoring of interventions is proposed as a key means by which to overcome these inequalities. There have been several behavioural interventions developed for African-American populations, incorporating culturally tailored strategies showing improvement of CVD risk profiles, smoking cessation, dietary behaviours and weight loss, but diabetes self-management and, in particular, prevention studies have not been as widely studied for these communities(Reference Samuel-Hodge, Keyserling and Park19). The available literature in populations outside of the USA is very scarce. Interventions of these types include a wide variation of culturally tailored strategies, where some may include one or a combination of strategies and others give little attention to defining them. This makes it challenging in the replication of methods and implementation in the public health sector. Lagisetty et al. (Reference Lagisetty, Priyadarshini and Terrell20) proposed a novel framework that characterised four key domains (Facilitator, Location, Language and Messaging) of culturally tailored interventions in order to define patterns that contribute to better outcomes.
The aim of this systematic review is to evaluate the methods of cultural tailoring used in lifestyle interventions for T2D prevention or management for populations of Black African ancestry and to examine the effectiveness of such interventions on glycaemic control.
Methods
Data sources and study eligibility
Three databases (Medline, Embase and Psychinfo) were searched for articles published from database inception until the search date (October 2020). The full search string is shown in Supplementary Material: search terms (exploded to retrieve related fields) included the following: ‘diabetes prevention’ or ‘management’, ‘Type 2 Diabetes’ and ‘African ancestry’, ‘African-American’, ‘Black’ or ‘Minority Groups’ in combination with ‘Cultural tailoring’ and ‘Randomised controlled trial’ or ‘intervention’. Grey literature databases and sources were not searched.
To be included, studies had to meet the following criteria: (1) adult population (aged ≥18 years) of Black African ancestry, defined as >50 % of study participants being of Black African ancestry; (2) population diagnosed with T2D or prediabetes, impaired fasting glucose or impaired glucose tolerance; (3) evaluation of a culturally tailored lifestyle intervention (interventions were considered culturally tailored if indicated in text as being culturally tailored, culturally adapted or cultural sensitivity tailoring); (4) intervention outcome measures included change in HbA1c or fasting blood/plasma glucose and (5) were randomised controlled trials. Studies were not excluded on the basis of language.
Study selection and data extraction
Titles and abstracts were screened by two independent assessors (NW, SA) and excluded if they did not meet the eligibility criteria, where eligibility could not be ascertained by title and abstract, full texts were reviewed by one assessor (NW). Full texts were reviewed to ensure eligibility by one author and in the case of uncertainty, a second independent reviewer (LG) was consulted to make the final decision. Additional studies were identified by hand searches of bibliographies and reference lists.
Descriptive data were extracted by one assessor (NW) to include year of publication, study design, number of participants, age, gender, ethnicity of targeted population, presenting condition (diabetes or pre-diabetes), setting of intervention, duration of intervention, intervention characteristics and control-arm characteristics. Outcome data extracted included mean/median HbA1c/fasting glucose, mean change (or baseline and post-intervention if not included) and statistical significance. If available, mean weight (in kg, or BMI in kg/m2) and weight change were also extracted, as well as measurements of diabetes knowledge as a secondary outcome. Details of components of the cultural tailoring of the intervention were extracted in accordance with the Facilitator-Location-Language-Messaging domains proposed by Lagisetty et al. (Reference Lagisetty, Priyadarshini and Terrell20) This was used to classify culturally tailored components based on use of Facilitators, Location, Language and Messaging. Information on Facilitator was regarded as the use of ethnically matched community health workers (CHW), community-based facilitators or healthcare professionals. Location of intervention referred to the setting where the intervention took place. The language domain accounted for adjustments in intervention to match literacy or language of the population, and messaging content encompassed altered content based on cultural specifics to faith, family, gender or diet.
Risk of bias
Risk of bias was assessed independently by two reviewers (NW, LG) using the Cochrane tool for assessing risk of bias in RCT(Reference Sterne, Savovic and Page21), adjusting the tool for lifestyle interventions. Bias was assessed at the outcome level based on elements including randomisation of sequencing, allocation concealment, blinding of outcome assessment and incomplete outcome data and given a rating of present (+), not present (-) or unclear (?) which was used to determine overall risk of individual studies.
Results
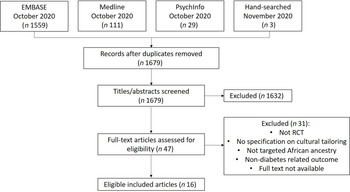
A total of 1702 citations were retrieved from EMBASE, MEDLINE, PsycINFO and hand searches of reference lists (Fig. 1). After removing duplicates, 1679 abstracts remained. Following screening of titles and abstracts, forty-seven full-text articles were further screened for inclusion. In total, sixteen RCT were eligible for inclusion.

Fig. 1 PRISMA flow diagram
Table 1 displays the characteristics of the included RCT; all took place in the USA with a total of 3568 participants. Mean age of participants was 54·8 years, and all studies recruited more than 50 % women; four studies included only women(Reference D’Eramo Melkus, Chyun and Vorderstrasse22,Reference Murrock, Higgins and Killion23,Reference Lutes, Cummings and Littlewood24,Reference Keyserling, Samuel-Hodge and Ammerman25) . Eleven of the studies exclusively enrolled adults of Black African ancestry and five targeted multiple ethnicities with more than 50 % of the population group being of Black African ancestry(Reference Ackermann, Liss and Finch26,Reference Ruggiero, Riley and Hernandez27,Reference Spencer, Rosland and Kieffer28,Reference Mayer-Davis, D’Antonio and Smith29,Reference Sharp, Tilton and Touchette30) . Two studies enrolled adults with pre-diabetes or at high risk of T2D(Reference Ackermann, Liss and Finch26,Reference Sattin, Williams and Dias31) , and seven reported HbA1c as a secondary outcome, with primary outcomes being weight loss (n 5)(Reference Ackermann, Liss and Finch26,Reference Mayer-Davis, D’Antonio and Smith29,Reference Sattin, Williams and Dias31,Reference Lynch, Liebman and Ventrelle32,Reference Samuel-Hodge, Holder-Cooper and Gizlice33) , physical activity levels(Reference Keyserling, Samuel-Hodge and Ammerman25) and 3-year hospital event(Reference Gary, Batts-Turner and Yeh34). There was one pilot RCT(Reference Lynch, Liebman and Ventrelle32). Follow-up ranged from 12 weeks(Reference Murrock, Higgins and Killion23,Reference Sattin, Williams and Dias31) to 20 weeks(Reference Samuel-Hodge, Holder-Cooper and Gizlice33), 6 months(Reference Spencer, Rosland and Kieffer28,Reference Lynch, Liebman and Ventrelle32) , 12 months(Reference Samuel-Hodge, Keyserling and Park19,Reference Lutes, Cummings and Littlewood24,Reference Keyserling, Samuel-Hodge and Ammerman25,Reference Ackermann, Liss and Finch26,Reference Ruggiero, Riley and Hernandez27,Reference Mayer-Davis, D’Antonio and Smith29,Reference Anderson, Funnell and Nwankwo35) , 18 months(Reference Lynch, Mack and Avery36) and 24 months(Reference D’Eramo Melkus, Chyun and Vorderstrasse22,Reference Sharp, Tilton and Touchette30,Reference Gary, Batts-Turner and Yeh34) . Nine provided group sessions(Reference Samuel-Hodge, Keyserling and Park19,Reference D’Eramo Melkus, Chyun and Vorderstrasse22,Reference Murrock, Higgins and Killion23,Reference Ackermann, Liss and Finch26,Reference Sattin, Williams and Dias31,Reference Lynch, Liebman and Ventrelle32,Reference Samuel-Hodge, Holder-Cooper and Gizlice33,Reference Anderson, Funnell and Nwankwo35,Reference Lynch, Mack and Avery36) , and five individual(Reference Lutes, Cummings and Littlewood24,Reference Ruggiero, Riley and Hernandez27,Reference Mayer-Davis, D’Antonio and Smith29,Reference Sharp, Tilton and Touchette30,Reference Gary, Batts-Turner and Yeh34) and two used a mixed approach of both individual and group sessions(Reference Keyserling, Samuel-Hodge and Ammerman25,Reference Spencer, Rosland and Kieffer28) .
Table 1 Study characteristics

HbA1c, haemoglobin A1c; FPG, fasting plasma glucose; DSMT, diabetes self-management training; PA, physical activity; DSME, diabetes self-management education; CHW, community health worker; TAU, treatment as usual; AA, African American; RI, reimbursable lifestyle intervention; UC, usual care; PCP, primary care physician.
All interventions were described as culturally tailored/adapted for African-American communities. Details of the cultural tailoring methods are provided in Table 2 and described in detail below.
Table 2 Facilitator-Location-Language-Messaging domains included in cultural tailoring

YDPP, YMCA diabetes practitioner; AA, African American; CHW, community health worker; RD, registered dietitian.
Effectiveness
Fifteen studies measured HbA1c (%) as an outcome, the remaining study by Sattin et al. (Reference Sattin, Williams and Dias31) on diabetes prevention measured fasting plasma glucose. Of the fifteen HbA1c studies, six reported significant differences (P-value of <0·05) in HbA1c at follow-up favouring the intervention(Reference Samuel-Hodge, Keyserling and Park19,Reference Murrock, Higgins and Killion23,Reference Ruggiero, Riley and Hernandez27,Reference Spencer, Rosland and Kieffer28,Reference Samuel-Hodge, Holder-Cooper and Gizlice33,Reference Lynch, Mack and Avery36) . A further five reported HbA1c changes favouring the intervention group but were NS (P > 0·05)(Reference D’Eramo Melkus, Chyun and Vorderstrasse22,Reference Lutes, Cummings and Littlewood24,Reference Mayer-Davis, D’Antonio and Smith29,Reference Lynch, Liebman and Ventrelle32,Reference Gary, Batts-Turner and Yeh34,Reference Anderson, Funnell and Nwankwo35,Reference Lynch, Mack and Avery36) . Two reported outcomes favouring the control (P = 0·33; P = 0·73, respectively)(Reference Samuel-Hodge, Keyserling and Park19,Reference Keyserling, Samuel-Hodge and Ammerman25) . Two studies targeted diabetes prevention, Sattin et al. (Reference Sattin, Williams and Dias31) measured fasting plasma glucose as a secondary outcome and found significant improvement in fasting plasma glucose in pre-diabetic participants in the intervention group compared with the control (-10·93 v. + 4·22 mg/dl, P = 0·017). In contrast, Ackermann et al. (Reference Ackermann, Liss and Finch26) measured change in HbA1c as a secondary outcome and found no significant difference between groups at follow-up (P > 0·05).
This review also considered diabetes knowledge as an indicator of intervention effectiveness. Seven of the included studies reported on diabetes knowledge using a range of questionnaires including (a) Diabetes Knowledge Test(Reference D’Eramo Melkus, Chyun and Vorderstrasse22); (b) Diabetes Knowledge Scale(Reference Samuel-Hodge, Keyserling and Park19,Reference Keyserling, Samuel-Hodge and Ammerman25) ; (c) Nutrition Knowledge Test(Reference Lynch, Liebman and Ventrelle32,Reference Lynch, Mack and Avery36) ; (d) perceived understanding of diabetes and (e) Spoken Knowledge in Low Literacy Diabetes Scale(Reference Sharp, Tilton and Touchette30). Five studies reported statistically significant improvements in knowledge compared with the control group (P = 0·003; P = 0·037; P = 0·010; P < 0·001; P = 0·048, respectively)(Reference Samuel-Hodge, Keyserling and Park19,Reference Keyserling, Samuel-Hodge and Ammerman25,Reference Lynch, Liebman and Ventrelle32,Reference Anderson, Funnell and Nwankwo35,Reference Lynch, Mack and Avery36) .
Twelve out of the sixteen articles reported on weight loss as either a primary(Reference Ackermann, Liss and Finch26,Reference Mayer-Davis, D’Antonio and Smith29,Reference Sattin, Williams and Dias31,Reference Lynch, Liebman and Ventrelle32,Reference Samuel-Hodge, Holder-Cooper and Gizlice33) or secondary outcome. Five studies reported a statistically significant reduction in weight, favouring the intervention (P = 0·046; P < 0·001; P < 0·010; P = 0·001; P < 0·0001, respectively)(Reference Lutes, Cummings and Littlewood24,Reference Ackermann, Liss and Finch26,Reference Mayer-Davis, D’Antonio and Smith29,Reference Sattin, Williams and Dias31,Reference Samuel-Hodge, Holder-Cooper and Gizlice33) , whilst seven found no significant difference between intervention and control groups (P > 0·05).
Methods of cultural tailoring – Facilitator-Location-Language-Messaging framework
Facilitators
Eleven of the sixteen interventions were delivered by, or supported by, members of the community. These members were all ethnically concordant and included a dance instructor(Reference Murrock, Higgins and Killion23), community diabetes advisor(Reference Samuel-Hodge, Keyserling and Park19,Reference Keyserling, Samuel-Hodge and Ammerman25) , community health worker (CHW)(Reference Lutes, Cummings and Littlewood24,Reference Spencer, Rosland and Kieffer28,Reference Sharp, Tilton and Touchette30,Reference Gary, Batts-Turner and Yeh34) , peer leaders(Reference Lynch, Liebman and Ventrelle32,Reference Lynch, Mack and Avery36) , church health advisors(Reference Sattin, Williams and Dias31) and YMCA instructors(Reference Ackermann, Liss and Finch26). Five interventions used healthcare professionals who consisted of registered dietitians(Reference Samuel-Hodge, Holder-Cooper and Gizlice33,Reference Anderson, Funnell and Nwankwo35) , nutritionist(Reference Mayer-Davis, D’Antonio and Smith29), medical assistant coach(Reference Ruggiero, Riley and Hernandez27) or a nurse(Reference D’Eramo Melkus, Chyun and Vorderstrasse22) Three studies used a combination of community members and healthcare professionals(Reference Sharp, Tilton and Touchette30,Reference Lynch, Liebman and Ventrelle32,Reference Lynch, Mack and Avery36) . No specification was given regarding ethnic matching of healthcare professionals except for in Ruggiero et al. (Reference Ruggiero, Riley and Hernandez27), where the medical assistant coach was ethnically matched to the participants. Of the eleven studies using members of the community, four reported statistically significant reduction in HbA1c at 8 months (P = 0·009), 12 weeks (P = 0·020) and 6 months (P < 0·010; P = 0·030, respectively)(Reference Samuel-Hodge, Keyserling and Park19,Reference Murrock, Higgins and Killion23,Reference Spencer, Rosland and Kieffer28,Reference Lynch, Mack and Avery36) ; however, two of these showed no significant difference (P = 0·330; P = 0·520, respectively) at 12-month follow-up(Reference Samuel-Hodge, Keyserling and Park19,Reference Lynch, Mack and Avery36) . A further three showed outcomes favouring the intervention but were NS (P > 0·05)(Reference Lutes, Cummings and Littlewood24,Reference Lynch, Liebman and Ventrelle32,Reference Gary, Batts-Turner and Yeh34) .
Location
Almost all studies (12/16) used convenient locations in the participants’ communities including community centres (n 7)(Reference Murrock, Higgins and Killion23,Reference Keyserling, Samuel-Hodge and Ammerman25,Reference Ackermann, Liss and Finch26,Reference Spencer, Rosland and Kieffer28,Reference Gary, Batts-Turner and Yeh34,Reference Anderson, Funnell and Nwankwo35,Reference Lynch, Mack and Avery36) , local churches (n 2)(Reference Samuel-Hodge, Keyserling and Park19,Reference Sattin, Williams and Dias31) , local park (n 1)(Reference Lynch, Liebman and Ventrelle32) or a local primary care centre specified as being in an underserved community (n 2)(Reference Ruggiero, Riley and Hernandez27,Reference Sharp, Tilton and Touchette30) . Three of these also included home visits(Reference Spencer, Rosland and Kieffer28,Reference Sharp, Tilton and Touchette30,Reference Gary, Batts-Turner and Yeh34) . In total, six of the twelve studies found the intervention resulted in a statistically significant difference between groups, including 3/7 studies using community centres(Reference Murrock, Higgins and Killion23,Reference Spencer, Rosland and Kieffer28,Reference Lynch, Mack and Avery36) . Both studies using local churches found significant differences between groups, favouring the intervention(Reference Samuel-Hodge, Keyserling and Park19,Reference Sattin, Williams and Dias31) . In the two studies conducted in primary care centres, both favoured interventions, but only one was significant(Reference Ruggiero, Riley and Hernandez27) (P < 0·001).
Language
Four studies adapted educational materials for literacy(Reference Samuel-Hodge, Keyserling and Park19,Reference Lynch, Liebman and Ventrelle32,Reference Anderson, Funnell and Nwankwo35,Reference Lynch, Mack and Avery36) , of which two found significant improvements in HbA1c favouring the intervention at 6 months(Reference Lynch, Mack and Avery36) and 8 months(Reference Samuel-Hodge, Keyserling and Park19) but not at 12 months. Two additional studies used CHW or medical staff to assist with forms and understanding to increase comprehension(Reference Ruggiero, Riley and Hernandez27,Reference Gary, Batts-Turner and Yeh34) . Of these, only Ruggiero et al. (Reference Ruggiero, Riley and Hernandez27) found a significant improvement in outcome measures between groups.
Messaging
The messaging component consisted of altering the content of the interventions and were divided into four subcategories: diet, faith, family and gender. Six tailored their intervention content to diet (Table 3)(Reference D’Eramo Melkus, Chyun and Vorderstrasse22,Reference Ruggiero, Riley and Hernandez27,Reference Mayer-Davis, D’Antonio and Smith29,Reference Lynch, Liebman and Ventrelle32,Reference Anderson, Funnell and Nwankwo35,Reference Lynch, Mack and Avery36) . Half specifically provided tailored cookbooks(Reference D’Eramo Melkus, Chyun and Vorderstrasse22,Reference Mayer-Davis, D’Antonio and Smith29,Reference Anderson, Funnell and Nwankwo35) and others (n 3) included cultural tailoring of diabetes nutritional education(Reference Ruggiero, Riley and Hernandez27,Reference Lynch, Liebman and Ventrelle32,Reference Lynch, Mack and Avery36) . These three all showed statistically significant improvements in HbA1c in the intervention group compared with the control group. Four studies targeted their content based on faith(Reference Samuel-Hodge, Keyserling and Park19,Reference D’Eramo Melkus, Chyun and Vorderstrasse22,Reference Murrock, Higgins and Killion23,Reference Lynch, Mack and Avery36) ; three of them were successful in improving glycaemic control in the intervention compared to control group. Only one study targeted content to family by use of family dyads(Reference Samuel-Hodge, Holder-Cooper and Gizlice33) and found a significant improvement in intervention group compared with the control.
Table 3 Effect of culturally tailored interventions on HbA1c, weight and diabetes knowledge

HbA1c, haemoglobin A1C; FPG, fasting plasma glucose; NR, not reported; NS, no significance; RI, reimbursable lifestyle intervention; UC, usual care.
* Significant within group difference; P < 0·05.
† The Diabetes Knowledge Test; a 25-item self-administered multiple- choice objective test developed by D’Eramo-Melkus, Wylie-Rosett, and Hagan (1992).
‡ 16-item adaptation of the Diabetes Knowledge Scale.
§ Adapted version of the Nutrition Knowledge Questionnaire; Score range 0–62. Higher scores indicate greater nutrition knowledge.
‖ Perceived understanding of diabetes; sale 1 = poor, 5 = excellent.
¶ Spoken Knowledge in Low Literacy in Diabetes scale.
** Significant within group difference; P < 0·001.
†† Mean % of correct answers.
Other methods were used in four studies to increase acceptability of the intervention. D’Eramo Melkus et al. (Reference D’Eramo Melkus, Chyun and Vorderstrasse22) provided free transportation, parking and/or childcare to participants and found improvements favouring the intervention at 24 months, although these were NS. Two studies provided free access to health facilities, one finding a significant difference between groups(Reference Spencer, Rosland and Kieffer28) and the other finding no improvement(Reference Ackermann, Liss and Finch26). Lutes et al. (Reference Lutes, Cummings and Littlewood24) provided participants with tools for weight, glucose and physical activity monitoring found to favour the intervention, yet results were NS at 12 months (P = 0·789).
One of the four studies using only one domain of cultural tailoring found significant HbA1c improvement (P = 0·040)(Reference Samuel-Hodge, Holder-Cooper and Gizlice33). Two of the five studies using two domains found significant difference between groups (P < 0·010; P = 0·017)(Reference Spencer, Rosland and Kieffer28,Reference Sattin, Williams and Dias31) . Seven studies incorporated more than two domains, and four found significant difference between groups (P = 0·009; P = 0·020; P < 0·001; P = 0·030, respectively)(Reference Samuel-Hodge, Keyserling and Park19,Reference Murrock, Higgins and Killion23,Reference Ruggiero, Riley and Hernandez27,Reference Lynch, Mack and Avery36) and the remaining showed non-significant improvements favouring the intervention (P > 0·05)(Reference Lynch, Liebman and Ventrelle32,Reference Gary, Batts-Turner and Yeh34,Reference Anderson, Funnell and Nwankwo35) .
Risk of bias
For the majority of studies included in this review, risk of bias was low. The majority of criteria for individual studies was assessed at low to uncertain risk of bias. Due to some studies’ selection bias, bias related to allocation concealment and bias in measurements of outcomes, the quality of the evidence was graded as moderate-low (Fig. 2).

Fig. 2 Risk of bias tool
Discussion
This review systematically investigated the effectiveness of culturally tailored lifestyle interventions on HbA1C and fasting glucose in people with T2D or prediabetes of Black African ancestry. Overall, the use of cultural tailoring resulted in improvements in glycaemic control. These results corroborate the Cochrane review by Attridge et al. (Reference Attridge, Creamer and Ramsden37) who found that culturally appropriate health education improved glycaemic control in participants from ethnic minority communities compared with those receiving usual care. However, the Cochrane review(Reference Attridge, Creamer and Ramsden37) focused on all minority ethnic groups, whereas this review focused solely on populations of Black African ancestry. In contrast to Attridge et al. (2014) who reported sustained improvement up to 24 months of follow-up, this review found short-term improvement prevalent up to 8 months(Reference Samuel-Hodge, Keyserling and Park19), but these effects on glycaemic control did not persist significantly at 12 or 24 months. A recent systematic review reported findings that the use of culturally tailored interventions for chronic disease management contributed to improvement in all healthcare outcomes, but that overall results were mixed(Reference Joo and Liu38). This outcome was seen in our study, where six articles reported non-significant improvement in HbA1c for the intervention compared with the control. The lack of significance can be explained by HbA1C as secondary outcome, no mention of statistical power or reporting of insufficient sample population to detect power hindering interpretation of true effectiveness of the intervention.
It has been reported that modest weight loss (˜5 %) can improve glycaemic control in T2D patients(Reference Horton, Silberman and Davis39). In the current review, twelve studies reported on weight loss, five as a primary outcome and only three of these found significant improvement(Reference Lutes, Cummings and Littlewood24,Reference Ackermann, Liss and Finch26,Reference Mayer-Davis, D’Antonio and Smith29) . However, weight loss was not associated with improved HbA1C in this population group. The average weight loss noted was 2·5 kg over 12 months, which may not have clinical significance on outcome measures. It is worth considering that greater reductions in HbA1c are seen with higher baseline HbA1c, and Ackermann et al. (Reference Ackermann, Liss and Finch26) investigated a pre-diabetic population with low baseline HbA1c (6·1 %), which may explain the insignificance on glycaemic control(Reference Esposito, Chiodini and Capuano40). Using a more sensitive marker of glycaemic control, such as plasma glucose concentrations, may exhibit improvements in pre-diabetic populations(Reference Knowler, Barrett-Connor and Fowler41). The study by Mayer-Davis et al. (Reference Mayer-Davis, D’Antonio and Smith29) reported a significant reduction in HbA1c in the control group despite a weight loss of only 0·2 kg. This may in part be due to the introduction of a diabetes management initiative at the clinic during the trial leading to improvements in diabetes self-management. In addition, participant motivation to engage in a 1-year long intervention for self-management improvement, described as the central concept in Wagner’s chronic illness care model(Reference Bodenheimer, Wagner and Grumbach42), may have also played a role in glycaemic improvement.
In contrast, improvements in diabetes knowledge scores were associated with improvement in glycaemic control. Five of the seven studies reporting on diabetes knowledge found significant improvements in intervention knowledge scores, which in the majority of studies also saw a positive impact on HbA1C. Self-management interventions are underpinned by patient education to subsequently increase patient knowledge about a disease(Reference Zimbudzi, Lo and Kerr43). The enhancement of knowledge is paramount to facilitate self-directed behaviour change and, consequently, improve health outcomes(Reference Brown44). A retrospective observational study on in-patient adults with T2D reported higher average HbA1C in those who had not received previous diabetes education(Reference Phillips, Rahman and Mattfeldt-Beman45). Further literature supports this association between metabolic control and participation in diabetes education interventions(Reference D’Eramo-Melkus, Wylie-Rosett and Hagan46). Although there is growing evidence to support this claim, it is important to note that knowledge in isolation has limited impact on behaviour change(Reference Lynch, Liebman and Ventrelle32,Reference Dunn, Beeney and Hoskins47) . Other factors such as patient attitudes, motivations and the integration of education with other therapies reflect the impact of intervention on behaviour change(Reference Norris, Engelgau and Venkat Narayan48). Culturally tailored interventions are based on the reframing of interventions to match pre-existing beliefs of ethnic minorities to facilitate the learning process(Reference Lynch, Mack and Avery36). The incorporation of these into the interventions in this review is the perceived mechanism for the positive association seen between knowledge and metabolic control. A 2012 pilot observational study found that combining culturally tailored education with shared decision making was a promising strategy for improvement in health outcomes in African-Americans(Reference Peek, Harmon and Scott49).
Resnicow et al. (Reference Resnicow, Baranowski and Ahluwalia50) proposed cultural sensitivity as defined by two dimensions; surface structures, involving matching of intervention materials and messages to surface or ‘superficial’ characteristics of a target population to increase acceptance, for example, language; or deep structures, involving incorporation of the cultural, social, historical or environmental forces that target health behaviour in the target population that determines efficacy of the programme. In the current review, the majority of studies tailored to location and facilitators with lesser amount tailoring to messaging and language. Overall, studies that tailored to all four domains showed greater success than those only tailoring to one. Lagisetty et al. (Reference Lagisetty, Priyadarshini and Terrell20) reported similar findings indicating the effectiveness of using more than one component of both surface and deep structures of cultural tailoring to increase efficacy of interventions.
This review reported improvements in glycaemic control in a majority of the studies with interventions using members of the community as facilitators. This contributes to the growing body of literature that suggests community members can have a positive impact on improving ethnic minority participants health status(Reference Fedder, Chang and Curry51). Ethnic minorities in the USA and UK are more likely than majority White populations to have lower levels of trust and satisfaction with their physician(Reference Hunt, Gaba and Lavizzo-Mourey52), with African-Americans reportedly preferring a culturally concordant physician(Reference Chen, Fryer and Phillips53). This was evidenced in the study by Ruggiero et al. (Reference Ruggiero, Riley and Hernandez27) which included the use of a medical assistant coach that was matched to patient’s ethnicity in routine diabetes clinic and found a significant improvement in HbA1c post intervention. This preference may be related to the perceived levels of racism within healthcare systems influencing cultural mistrust(Reference LaVeist, Nickerson and Bowie54). Interestingly, fewer than 40 % of primary care clinicians recognise the presence of disparities in health stemming from societal racism(Reference Sequist, Fitzmaurice and Marshall55) presenting a barrier for improved healthcare in ethnic minorities. An RCT of cultural competence training in USA primary care teams demonstrated an increase in clinician awareness of these disparities but reported limited evidence on the clinical impact in African-Americans, perhaps due to the population group being made of predominately Whites (64 %) v. 36 % African-Americans(Reference Sequist, Fitzmaurice and Marshall55). Nonetheless, as patient race may influence clinical decisions, more research and attention needs to be given to understandings of race v. ancestry or ethnic minority as concepts and to appreciate the need for improving cultural competence of healthcare professionals matched to ancestry to improve health outcomes and increase trust in healthcare systems. The ability of community members to promote health messages to their respective ethnic, cultural or geographical communities gives them the unique capability to bridge the relationship of mistrust between healthcare teams. Patients seemingly have more trust in CHW who understand their socio-cultural barriers, provide social support and can increase relevancy of disease management. A systematic review of strategies to improve response to cultural interventions in T2D by Glazier et al. (Reference Glazier, Bajcar and Kennie56) showed that more successful interventions used a community educator, correlating well with this review. This review found that studies often used CHW who had or lived with someone who had T2D, increasing the relevance and empathy between participants and facilitators.
This review also showed a favouring towards interventions using group sessions for education (n 8). In addition to ethnically matched facilitators, group settings elicited feelings of community in some studies. In Murrock et al. (Reference Murrock, Higgins and Killion23), the women in the focus group reported feeling ‘disappointed’ when they had to miss a session with other comments including ‘we all had the same thing so you don’t really think about it’ and ‘the fact that it was all different sizes, shapes, ages. There was nothing to be ashamed of and we were all here together. We all had the common ground.’ This exemplifies how inherent support of ethnically matched groups and facilitators is an important benefit to patient attitudes in tailored interventions.
Three quarters of studies in this review adapted the intervention to a suitable, convenient location for participants. Frequently reported barriers for engagement in health promoting behaviours in African-American women include unsafe neighbourhoods and lack of transportation. Community-based interventions using local, free community centres allows for increased accessibility, reduces effort to engage with the intervention and is perceived to achieve positive outcomes in self-management interventions. The study by D’Eramo Melkus et al. (Reference D’Eramo Melkus, Chyun and Vorderstrasse22) demonstrated that increasing level of care points by including interventions in local pharmacies in under-served communities may have a beneficial impact over standard care. More evidence would be needed to support this claim as the study did not test for differences against standard care. Samuel-Hodge et al. (Reference Samuel-Hodge, Keyserling and Park19) reported that effective community-based interventions can complement clinic-based care and lead to improved diabetes self-management. Only one study in this review included the use of both primary care and group sessions and found no significant improvement in glycaemic control(Reference Keyserling, Samuel-Hodge and Ammerman25) but did find significant improvement in their primary outcome of physical activity levels.
This review included two studies with interventions held in church-based settings, both of which saw positive impacts on glycaemic control. A higher percentage of people of Black African ancestry are likely to characterise themselves as religious and attend religious services regularly compared with other groups(57). As well as being a location of high point of contact, the churches play a major role in providing spiritual and social support for many attendees, providing them comfort to engage with trusted individuals. Therefore, using church-based settings enables the tailoring of interventions based on up to three domains (location, facilitator and messaging). The high attendance and comfort expressed in these venues makes churches ideal for reaching, recruiting and implementing self-management interventions, but the history of minorities being under-served and exploited can lead to suspiciousness and reluctance to participate that must be taken into consideration in public health implications(Reference Markens, Fox and Taub58). It is evidenced that increasing point of access to care for these population groups along with having access to social support is beneficial for individual health outcomes in these population groups.
In this review, language tailoring was the least frequently used and included adjustments to literacy by use of simple teaching materials, assistance with forms and use of interactive and hands-on teaching methods. The sensitive use of language is largely seen as a surface structure of cultural tailoring with ability to increase comprehensibility and ultimately acceptability of the intervention. The integration of the language domain as a supplementary tailoring method may therefore have positive effects, but no studies in this review used it as a sole method of tailoring.
The messaging domain of Facilitator-Location-Language-Messaging integrates deeper structures of cultural tailoring by incorporation of cultural and social forces of ethnic communities. A majority of studies tailoring the messaging used diet as the method of tailoring where interventions tailored the nutritional curriculum to match pre-existing cultural beliefs. For example, in Lynch et al. (Reference Lynch, Mack and Avery36), participants noted that categories of natural food were frequently labelled as God’s Food, so researchers used this pre-existing belief to build upon the nutritional curriculum to enhance participant understanding of macronutrient composition of foods and learning of new ways of eating. Fewer studies targeted faith (n 4) and only one study targeted family(Reference Samuel-Hodge, Holder-Cooper and Gizlice33). Interestingly, as well as finding a significant improvement in HbA1c, the use of family dyads also demonstrated improvements in health markers in the member of family that did not present with T2D. Certain family characteristics have been associated with poor diabetic outcomes(Reference Fisher, Chesla and Bartz59), suggesting that by encouraging family togetherness and interaction it may help to prevent diabetes onset. However, the current study was the only one using family and used a control receiving no treatment, thereby limiting evidence for the inclusion of family members and warranting further investigation for potential public health implication.
The strengths and limitations of our review warrant consideration. The focus on only RCT allowed for evaluation of differences between control and intervention groups in relation to culturally tailored components though it means other evidence was excluded that could have provided insights. All studies included in this systematic review were conducted in African-Americans in deprived communities of the USA. Due to the differences in culture and racial categorisations and the lack of sensitivity of these categories, it is unclear if these results can be successfully translated to other regions, including the UK. A further limitation is the very limited RCT in relation to prevention of T2D in populations of Black African ancestry.
In conclusion, this systematic review presents evidence on the effectiveness of culturally tailored interventions for diabetes management, with further evidence needed to support preventative implications. The evidence shows that the most common forms of tailoring were location and facilitator, with these showing the most success in improving glycaemic control. Interventions that tailored to more than one domain were, in general, more successful at improving glycaemic control in this population. Interestingly, these studies showed no association between weight loss and glycaemic control; however, the tailoring of interventions has led to increased knowledge and ultimately improvement in glycaemic control. Knowledge improvement is hence a potential driving force in the beneficial outcomes associated with tailored interventions. Heterogeneity in methods of tailoring, outcomes and control groups was evident across this review therefore limiting conclusions that can be drawn about the effectiveness of these interventions. The use of a standardised definition of cultural tailoring is needed to compare findings and for the creation of effective public health policy.
Acknowledgements
Acknowledgements: The researchers have no conflicts of interest. Initial searching in electronic databases and screening of studies was done in coordination with Summor Asantewa-Ampaduh, a final year BSc Nutrition student. Financial support: This research received no specific grant from any funding agency, commercial or not-for-profit sectors. LMG is supported by the National Institute for Health Research (NIHR) Applied Research Collaboration South London at King’s College Hospital NHS Foundation Trust. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health. Conflict of interest: There are no conflicts of interest. Authorship: All authors have made substantial contributions to this study. L.M.G. and C.R. were responsible for the study conception. N.M.W., S.A.-A., C.R. and L.M.G. were responsible for the design of the study. L.M.G., N.M.W. and S.A.-A. developed the protocol. N.M.W. and S.A.-A. undertook data identification and N.M.W. undertook data analysis and drafted the manuscript. All authors read, revised and approved the final manuscript. L.M.G. is guarantor. Ethics of human subject participation: Not applicable, secondary analysis, no primary data involved.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980021003682







 Open access
Open access