


The prevalence of risk factors for non-communicable diseases has increased in both adolescents and adults in Iran. According to the results of the Tehran Lipid and Glucose Study (TLGS)Reference Azizi, Allahverdian, Mirmiran, Rahmani and Mohammadi1, Reference Azizi, Rahmani, Madjid, Allahverdian, Ghanbili and Ghanbarian2, 18% of adolescents are overweight or obese, 12–18% have cholesterol level above 200 mg dl− 1 and 14–17% have low-density lipoprotein cholesterol level greater than 130 mg dl− 1. Epidemiological studies have shown that changes in lifestyle during recent years, especially changes in nutritional habits, may be responsible for increasing rates of non-communicable diseasesReference Harvey-Berino, Hood, Rourke, Terrance, Dorwaldt and Secker-Walker3. Nutritional factors have an important role in the incidence of non-communicable diseasesReference Woo, Leung, Ho, Lam and Janus4 and they are strong predictors of cardiovascular risk among adolescentsReference Azizi, Mirmiran and Azadbakht5. As poor nutritional habits may be formed during the teenage years, and most nutritional habits in adults result from nutritional behaviours gained during adolescence, it is very important to study the nutritional knowledge, attitudes and practices of adolescentsReference Harvey-Berino, Hood, Rourke, Terrance, Dorwaldt and Secker-Walker3.
Different studies have shown that most obese or overweight adolescents are at high risk of developing non-communicable diseases in adulthood6. Several decades have passed since nutritional education was first introduced to reduce non-communicable diseasesReference James, Ralph and Bellizzi7. Although education improves nutritional knowledge, there is often a big gap between knowledge and practiceReference Girois, Kumanyika, Morabia and Mauger8. For health promotion to be successful, it must address the needs and aspirations of the target audience and take into consideration their current knowledge, attitudes and behavioural patternsReference Buttriss9. Previous studies have investigated the knowledge, attitudes and practices of Iranian adolescents with regard to iron-deficiency anaemiaReference Keshavarz Mohammadi, Shojaee Zadeh, Mahmoodi, Froozani and Ghasemi10 and nutritional needsReference Sfarjani, Golestan, Derakhshani and Molabashi11, Reference Sfarjani, Golestan, Rasooli and Roosta12. But there is no study that determines the accordance between knowledge and practice in the field of non-communicable disease. Therefore the present study was conducted to determine the knowledge, attitudes and practices of Tehranian adolescents concerning the role of healthy nutrition for prevention of non-communicable diseases.
Subjects and methods
This study was undertaken on a representative sample of 7669 Tehranian adolescents aged 10–18 years. These adolescents were randomly chosen from 22 junior high schools and high schools. The study was conducted within the framework of the TLGS, a prospective study performed on residents of district 13 of Tehran with the aim of determining the prevalence of risk factors for non-communicable disease and developing a healthy lifestyle to improve these risk factorsReference Azizi, Rahmani, Emami and Madjid13.
A validated questionnaire was used to evaluate the knowledge, attitudes and practices (KAP) of adolescents with regard to healthy nutrition for preventing non-communicable diseases. Variables covered by this KAP questionnaire were weight, type of fat intake, and fibre, sugar and salt intake. Knowledge questions were designed to be answered as ‘yes’, ‘no’ or ‘I don't know’. The correct answer was scored as +1, the wrong answer as − 1 and ‘I don't know’ scored 0. Attitude was scored from 1 to 4 as the lowest and highest scores in each question, respectivelyReference Woo, Leung, Ho, Lam and Janus4. In practice questions, the consumption frequency of dairy, beverages, nuts, crisps, corn balls, vegetables and fruits, whole grains and refined grains was evaluated in meals and snacks separatelyReference Woo, Leung, Ho, Lam and Janus4. The frequency of food intake was determined in the KAP questionnaire by: 1, yes, always; 2, yes, often; 3, yes, sometimes; and 4, never. Face and content validity of the questionnaire was assessed by experts. For evaluating the reliability of the questionnaire pre-tests and post-tests were conducted one month apart; the correlation between the two tests was r = 0.7, P < 0.001. The maximum scores in the knowledge, attitudes and practices sections were 36, 28 and 64, respectively. In each part, scores of more than 75% of the maximum were considered ‘good’, scores of 50–75% were considered ‘fair’ and scores lower than 50% were considered ‘poor’Reference Harvey-Berino, Hood, Rourke, Terrance, Dorwaldt and Secker-Walker3. Thus poor, good and fair scores were as follows: < 18, >27 and 18–27, respectively, for knowledge; < 14, >21 and 14–21, respectively, for attitude; and < 32, >48 and 32–48 respectively, for practice.
Usual dietary intake was assessed by using a 168-item semi-quantitative food-frequency questionnaire (FFQ). The questionnaire was administered by trained dietitians who had 5 or more years of experience in the Nationwide Food Consumption Survey projectReference Kimiagar, Ghaffarpour, Houshiar-Rad, Hormozdyari and Zellipour14, 15. The FFQ consisted of a list of foods and a standard serving size for each (Willett format)Reference Rimm, Giovanucci, Stamfer, Colditz, Litin and Willett16. In this questionnaire subjects were asked to report their frequency of consumption of a given serving of each food item during the previous year on a daily (e.g. bread), weekly (e.g. rice, meat) or monthly (e.g. fish) basis. Portion sizes of consumed foods were converted to grams using household measuresReference Ghaffarpour, Houshiar Rad and Kianfar17. Each food and beverage was then coded according to the prescribed protocol and analysed for content of energy and the other nutrients using Nutritionist III software (version 7.0; N Squared Computing), which was designed for evaluation of Iranian foods.
The reliability of the FFQ in this cohort was evaluated in a randomly chosen subgroup of 132 subjects by comparing nutrient consumption determined by responses to the FFQ on two occasions. The correlation coefficients for the repeatability of grain, vegetable, fruit, dairy and meat were 0.85, 0.79, 0.71, 0.74 and 0.70, respectively. The FFQ also had high reliability for nutrients. For example, the correlation coefficients were 0.81 for dietary fibre, 0.75 for calcium and 0.71 for vitamin C. Comparative validity was determined by comparison with intake estimated from the average of twelve 24-hour dietary recalls (one for each month of the year). Preliminary analysis of the validation study showed that nutrients were moderately correlated between these two methods after controlling for total energy intake. These correlation coefficients were 0.69 for dietary fibre, 0.64 for vitamin C and 0.68 for calcium intake. Overall, these data indicate that the FFQ provides reasonably valid measures of the average long-term dietary intakeReference Esmaillzadeh, Mirmiran and Azizi18.
Results
The mean ( ± standard deviation) age and body mass index of the adolescents was 14 ± 1 years and 27.2 ± 11 kg m− 2, respectively.
Table 1 shows the frequency of the adolescents' nutritional knowledge, attitude and practice scores according to sex. The mean knowledge score was 30 ± 3.8 (range: 17–40) in boys and 31 ± 3.8 (range: 18–40) in girls. Attitude score was 20 ± 4.3 (range: 6–28) in boys and 19 ± 4.6 (range: 7–28) in girls. The mean score of nutritional behaviour (practice) in boys and girls was 44 ± 6.5 (range: 16–66) and 42 ± 6.8 (range: 11–64), respectively. There were significant differences in the knowledge, attitude and practice scores between girls and boys (P < 0.001). Twenty-eight per cent of the parents were university-educated. There was a significant positive correlation between the nutritional knowledge of students and the education level of their parents (r = 0.14, P < 0.001). A higher percentage of girls had good nutritional knowledge (82% of girls vs. 75% of boys, P < 0.05) but a higher percentage of boys had good nutritional attitude (39% of boys vs. 33% of girls, P < 0.05).
Table 1 Absolute and relative frequency of knowledge, attitude and practice scores among Tehranian adolescents

Values in parenthesis are relative frequency.
* Significantly different compared with girls: P < 0.05.
The key questions of the KAP questionnaire were defined according to the results of factor analysis. The frequency of adolescents giving the correct answer to the key questions is shown in Table 2. The results showed that 36% of adolescents did not know that sweets and candies increased weight. Fifty-six per cent of adolescents did not have correct knowledge about fish oil. Eighty-five per cent of adolescents knew that drinking too many soft beverages resulted in overweight or obesity, but only 4.5% of them did not drink soft beverages. Although 89% of adolescents knew that crisps and corn balls are not healthy snacks, 45% of them used such snacks during their break time. Twenty-eight per cent of adolescents preferred corn ball to nut consumption. Only 37% of adolescents consumed fresh vegetables with their meals and only 10% of them used whole-grain biscuits.
Table 2 Frequency of correct answers to key questions among Tehranian adolescents

* Significantly different compared with girls: P < 0.05.
Nutrient and food group intakes of the adolescents are shown in Table 3. The results reveal that girls consumed a higher amount of saturated fatty acids than boys (% of energy: 15% vs. 10%, P < 0.05), while boys consumed a higher amount of polyunsaturated fatty acids (% of energy: 14% vs. 10%, P < 0.05). Cholesterol intake was higher in girls (380 mg day− 1 for girls vs. 230 mg day− 1 for boys, P < 0.05). Boys consumed a greater amount of whole grains than girls (83 vs. 56 g day− 1, P < 0.05). Table 4 shows the food items that were eaten as snacks. Crisps were the salty snack with the highest consumption among adolescents. Creamy wafers had the first rank among sweet snacks. There was a significant correlation between nutritional knowledge and attitude scores (r = 0.24, P < 0.001), but the correlation between nutritional knowledge and behaviour scores was weak (r = 0.05, not significant).
Table 3 Nutrients and food groups consumed by Tehranian adolescents

Data are presented as mean ± standard deviation.
* Significantly different compared with girls: P < 0.05.
Table 4 Daily intake of food items eaten as snacks by Tehranian adolescents
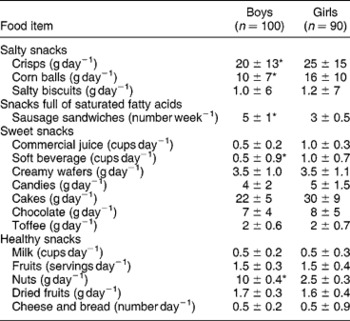
Data are presented as mean ± standard deviation.
* Significantly different compared with girls: P < 0.05.
Discussion
The results of present study, conducted among a group of Tehranian adolescents, showed that only 25% of boys and 15% of girls had good scores for nutritional practice, while 75% of boys and 82% of girls had good scores for nutritional knowledge. These results reveal a gap between knowledge and behaviour in Tehranian adolescents, as reported in other countriesReference Girois, Kumanyika, Morabia and Mauger8, Reference Rasanen, Niinikoski, Keskinen, Tuominen, Simell and Viikari19, Reference Pirouznia20. Findings from a study on Tehranian adults also indicated a sizeable gap between nutritional knowledge and behaviourReference Mohammadi, Mirmiran, Bayegy and Azizi21. More than half of the adults were residents of east Tehran and had moderate knowledge, whereas desirable practice was seen in only a quarter of themReference Mohammadi, Mirmiran, Bayegy and Azizi21.
Broad social and cultural factors play important roles in shaping food choicesReference Shephard and Stockley22. Physiological needs, body image, peer pressure, classmates' nutritional behaviour, media social norms, availability of foods, personal experiences and food preferences may be some factors. The packaging of foods is also important. The use of attractive boxes for non-nutritive salty and fatty snacks may have an important influence on food choice. There was a weak correlation between nutritional knowledge and behaviour among these Tehranian adolescents. The literature on eating behaviour and its relation to nutrition knowledge is contradictoryReference Shephard and Stockley22, Reference Cotugna, Subar, Heimendinger and Kahle23. Some researchers have shown that nutritional knowledge is highly and positively related to nutritional behaviours, whereas others have found little correlation between nutritional knowledge and actual choices of healthy food.
In the present study, the nutritional knowledge of girls was significantly higher than that of boys. Girls in general may be more knowledgeable about food, nutrition and health and they manifest a more heightened concern about their personal and physical appearance than boysReference Turrell24. Yet despite their lower knowledge, boys had a greater level of good nutritional practice. In the USA and Geneva, Switzerland, the knowledge and attitude of women about diet and health were better than those of menReference Girois, Kumanyika, Morabia and Mauger8. However, in that study the mean scores for knowledge, attitude and practice were not very different and it seems that this significance could be an artefact because of the large sample size.
The amount of salty and sweet snacks consumed by the Tehranian adolescents was much greater than the amount of healthy snacks. Thus it seems that the nutrition transitionReference Ghassemi, Harison and Mohammad25 has also transferred to adolescents. The findings of the present study reinforce those of a previous study in this field, which showed that the diet quality of 73% of Tehranian adolescents needs improvementReference Mirmiran, Azadbakht and Azizi26.
As a whole, the present study shows that nutritional knowledge is not the only factor that can influence eating behaviour. Our findings are similar to the opinions of PirouzniaReference Pirouznia20 in this field. Considering that analysis of the results of a KAP questionnaire may be beneficial in health promotion programmes, there is no standard questionnaire on nutritional KAP for adolescents in Iran, which is one limitation of our study.
Besides administering a KAP questionnaire we assessed nutritional practices with a validated FFQ, which increased the validity of our results and was one of the strengths of this study. As the nutritional knowledge of Tehranian adolescents does not accord with their nutritional behaviour, nutritional intervention seems warranted. The necessity for intervention is especially clear given the nutrition transition reported in Iran in recent yearsReference Ghassemi, Harison and Mohammad25.
As most nutritional habits are confirmed in the teenage years and these habits track as nutritional preferences into adulthood, nutritional intervention according to the results of KAP questionnaires may be important in health promotion programmes. Such results might help in the future design and targeting of appropriate interventions, such as nutrition education programmes.




