


Maternal nutrition during pregnancy is important for maternal and child health. Inadequate nutritional status of pregnant women has been reported to be associated with adverse birth outcomes( Reference Abu-Saad and Fraser 1 ), poor perinatal survival( Reference Rush 2 ), impaired physical and cognitive development in childhood, and nutrition-related metabolic disorders in adulthood( Reference Black, Victora and Walker 3 – Reference Ahmed and Tseng 5 ). Poor dietary intakes in pregnancy can contribute to suboptimal nutritional status and further influence maternal and child health. Severe protein and energy shortages are observed to decrease birth weight( Reference Lumey 6 ). Maternal Fe deficiency can lead to anaemia and increases the risk of low birth weight and preterm delivery( Reference Scholl and Hediger 7 ). Ca intake is associated with the reduced risk of pre-eclampsia and preterm birth( Reference Hofmeyr, Lawrie and Atallah 8 ). Fe and Ca deficiencies may also contribute to maternal deaths( Reference Black, Victora and Walker 3 , Reference Scholl and Hediger 7 , Reference Hofmeyr, Lawrie and Atallah 8 ). Poor Zn status during pregnancy has been suggested as a risk factor for adverse long-term consequences on growth, immunity and metabolic status of surviving offspring( Reference Chaffee and King 9 , Reference King 10 ). Low intake of folate during the periconceptional period is found to increase the risk of congenital abnormalities such as neural tube defects( Reference De-Regil Luz, Fernández-Gaxiola and Dowswell 11 ) and congenital heart defects( Reference van Beynum, Kapusta and Bakker 12 , Reference Ionescu-Ittu, Marelli and Mackie 13 ).
Results from the 2002 Chinese National Nutrition and Health Survey (NNHS) suggested that maternal diets during pregnancy were dominated by plant-based foods and that intakes of nutrients such as Ca, Fe, Zn, vitamin A, thiamin and riboflavin were often not satisfactory( Reference Yin 14 ). However, China is reported to have experienced a nutrition transition during the last few decades( Reference Popkin 15 ), with the intakes of animal-source foods and edible oils increasing rapidly and the intakes of grains and legumes reducing markedly( Reference Zhai, Du and Wang 16 ). Latest information on the dietary intakes and dietary patterns among Chinese pregnant women is needed to reflect their nutritional status during the nutrition transition in China. One recent study conducted in 2011 determined the nutrient intake status of pregnant women in urban China( Reference Liu, Zhang and Pares 17 ). A previous report based on the 2002 NNHS revealed significant differences in dietary intakes between pregnant women in urban and rural China( Reference Lai, Yin and Ma 18 ). However, to our knowledge, no recent study on maternal dietary intakes during pregnancy in rural China has been reported. Moreover, limited information on the nutritional status of pregnant women in western China is available( Reference Cheng, Dibley and Zhang 19 , Reference Dang, Yan and Zeng 20 ). In the present study we aimed to describe nutrient intakes, characterize dietary patterns and analyse the associations of nutrient intakes and dietary patterns with sociodemographic characteristics among pregnant women in Shaanxi Province of Northwest China.
Materials and methods
Study setting
The study was conducted in Shaanxi Province of Northwest China between August and November 2013. This area can be divided geographically into three regions: northern, central and southern Shaanxi. The climates of the three regions vary significantly because of the large span in latitude, with semi-arid temperate, north temperate monsoon and humid subtropic zones predominantly prevalent from north to south. Natural resources, history, culture and lifestyle also differ greatly among the three regions. The province had approximately 37·6 million inhabitants in 2013 and about 30 % of them resided in urban areas. Regarding socio-economic level, Shaanxi is ranked as a developing area in China with the provincial Gross Domestic Product amounting to $US 252·7 billion in 2013( 21 ).
Study design and participants
A population-based cross-sectional survey was carried out to investigate the prevalence of and risk factors for birth defects and the nutritional status of mothers during pregnancy in Shaanxi Province, Northwest China. Women who were pregnant during 2010–2013 and had pregnancy outcomes before the survey were enrolled. Women were excluded if they could not answer the survey because of limited cognitive capacity. A sample of 30 027 participants was obtained using a stratified multistage random sampling method. Twenty counties and ten districts were randomly selected from the eighty rural counties and twenty-four urban districts in Shaanxi Province according to the proportion of rural to urban residents, population size and fertility rate. In each sampled county, six townships were randomly selected; six villages were randomly obtained from each selected township; and then thirty eligible women were randomly selected in each village. In each sampled district, three streets were randomly selected; six communities were randomly obtained from each selected street; and then sixty eligible women were selected in each community. To obtain relatively accurate dietary recall, the present analysis included only those mothers who were pregnant during 2012–2013 and had infants less than 12 months old when interviewed. A total of 7750 eligible women were selected into the study. In addition, we excluded 288 women who reported an implausible dietary energy intake (greater than 20 920 kJ/d or less than 2092 kJ/d), leaving 7462 women for the final analysis. The median month after delivery when the 7462 mothers were asked to report diets during pregnancy was month 3 (10th–90th percentile, month 0–7).
Sociodemographic information
The participants were interviewed face to face by trained professional staff from Xi’an Jiaotong University Health Science Center. Sociodemographic information was collected through a standard questionnaire. Maternal age at delivery was divided into three categories (<25 years, 25–29 years and ≥30 years), parity into two categories (1 and ≥2), maternal educational level into three categories (primary school or below, junior high school and senior high school or above) and maternal occupation into two categories (farmer and others). Per capita annual household income was categorized into three quartiles (<6200 Yuan, 6200–11 999 Yuan and ≥12 000 Yuan, where 1 Yuan=$US 0·15 on 7 May 2016).
Dietary intake
Previous studies suggested that maternal dietary intakes and patterns change little from early to late pregnancy( Reference Crozier, Robinson and Godfrey 22 , Reference Rifas-Shiman, Rich-Edwards and Willett 23 ) and it is burdensome and expensive to evaluate dietary intakes at more than one period during pregnancy for large epidemiological studies( Reference Rifas-Shiman, Rich-Edwards and Willett 23 ). Thus, diet assessment during the whole pregnancy at one time can be reasonable, convenient and economical for our large epidemiological survey with multiple dietary exposures and outcomes of interest. In the present study, a semi-quantitative FFQ was used to assess dietary intakes of mothers during the whole pregnancy, at 0–12 months (median 3 months; 10th–90th percentile, 0–7 months) after delivery. The FFQ was established according to the previously validated FFQ designed for pregnant women in rural western China( Reference Cheng, Dibley and Zhang 19 , Reference Cheng, Yan and Dibley 24 ). In the validity and reproducibility study, FFQ were administered at the start of the third trimester and repeated three months later, and compared with six repeated 24 h recalls collected between the FFQ( Reference Cheng, Yan and Dibley 24 ). The correlation coefficients for most nutrients, for both reproducibility and validity, were within the range of 0·40 to 0·80( Reference Cheng, Yan and Dibley 24 ). A total of 107 food items were included in the FFQ, covering eighteen food groups (cereals, potatoes, legumes, vegetables, fungi, fruits, nuts, meats, dairy, eggs, fish, ethnic snacks, fast foods, beverages, liquor, sweets, oils and condiments) based on the China Food Composition Table( 25 ). The frequency scale of five food items (vegetable oils, animal oils, salt, sauce and sugar) was open-ended, and was listed as kilograms per month and the number of people who regularly consumed them. The frequency of the other 102 food items was reported according to eight predefined categories ranging from never to two or more times per day. The portion sizes for the 102 food items were recorded with the assistance of food portion images( Reference Cheng, Dibley and Zhang 19 , Reference Cheng, Yan and Dibley 24 ).
Dietary information in the FFQ was coded, computerized and transformed into daily energy and nutrient intakes according to the China Food Composition Tables( 25 , 26 ). The recommended nutrient intakes (RNI) from the latest Chinese Dietary Reference Intakes 2013 ( 27 ) were used to evaluate the dietary intakes of the participants during pregnancy. Since the reference values of some nutrients for women during the whole pregnancy are not available in the Chinese Dietary Reference Intakes 2013, the RNI for women during the three different trimesters of pregnancy were used. The adequate intake (AI) for vitamin E was used instead because of the unavailability of RNI for it. The RNI of energy for pregnant women with light physical level during the three trimesters is 7531, 8786 and 9414 kJ/d, respectively( 27 ). The recommended range for fat among pregnant women is 20–30 % of total energy and for carbohydrate is 50–60 % of total energy( 27 ). The median of the recommended range for fat and carbohydrate was used as the recommended value. In addition, dietary intakes among this population were compared with those in the 2002 NNHS. The design of the 2002 NNHS has been described in detail elsewhere( Reference Ma, Li and Jin 28 ). In brief, the 2002 NNHS was a nationally representative cross-sectional survey and dietary information was collected by 24 h dietary recall method for three consecutive days. Dietary intakes during the whole pregnancy were reported among 171 pregnant women in the 2002 NNHS( Reference Yin 14 ). The mean daily intakes in the 2002 NNHS were 9888 kJ for energy, 68 g for protein, 76 g for fat, 352 g for carbohydrate, 483 μg retinol equivalents for vitamin A, 1·1 mg for thiamin, 0·8 mg for riboflavin, 98 mg for vitamin C, 50 mg for vitamin E, 367 mg for Ca, 24 mg for Fe and 12 mg for Zn( Reference Yin 14 ).
Quality control
The interviewers were trained to standardize the administration of the questionnaire before the survey. Staff from the local health bureau and maternal and child health-care service centre coordinated fieldwork, with the help of doctors from the township hospitals and village clinics. During the investigation, a checking system was established in which all interviewers checked their own completed questionnaires, each interviewer checked another interviewer’s questionnaire and the supervisor checked all questionnaires. The participants were re-interviewed when key errors or missing values were identified.
Statistical analyses
A database was established using EpiData software version 3.1 and double data entry was conducted. Non-normal distribution of nutrient intakes was observed according to the Shapiro–Wilk test even after data transformations; therefore, median values were applied to describe nutrient intakes. The Wilcoxon signed-rank test was used to determine whether nutrient intakes were significantly different from those of pregnant women in the 2002 NNHS. The Mann–Whitney U test was applied to compare differences between two groups. The Kruskal–Wallis test was applied to compare the differences among more than two groups. The Wilcoxon two-sample test was further adopted to compare the differences between two subgroups of a sociodemographic group, with a Bonferroni-adjusted P≤0·017 (0·05/3) significant for the three pairwise comparisons.
Dietary patterns based on eighteen food groups in the China Food Composition Table( 25 ) were derived by principal component analysis with orthogonal (varimax) rotation. The Kaiser–Meyer–Olkin value and Bartlett’s test of sphericity were used to evaluate the reliability of principal component analysis before identifying the dietary patterns. The number of dietary patterns was extracted on the basis of eigenvalues >1·2, the scree plot and the interpretability of the factors( Reference Schulze, Hoffmann and Kroke 29 ). Food groups with absolute factor loadings >0·25 were considered as most highly related to the identified factors. Factor scores were calculated for each woman and each dietary pattern by multiplying factor loadings with the standardized value for each food and summing across the food items. Factor scores indicate the extent to which the woman’s diet conformed to the respective dietary patterns. The sociodemographic characteristics and daily nutrient intakes were described according to quartiles of dietary pattern scores. Categorical variables were reported as percentages and compared by the χ 2 test. Continuous variables were reported as median values and compared by the Kruskal–Wallis test. A two-tailed P<0·05 was considered statistically significant unless otherwise specified. Analyses were conducted using the Stata statistical software package version 12.
Results
Sociodemographic characteristics of the participants
The characteristics of the participants are shown in Table 1. About half (52·3 %) of the women were from central Shaanxi and 76·2 % lived in rural areas. The mean age at delivery was 26·7 (sd 4·6) years, with women aged 25–29 years at delivery accounting for 37·6 % of the sample. Regarding the recent pregnancy with known pregnancy outcomes, more than half of the women were at their first delivery. The majority (90·5 %) of participants had completed 9-year compulsory education (junior high school or above). Most participants (71·5 %) had no employment outside their home and were categorized as farmers.
Table 1 Sociodemographic characteristics of pregnant women (n 7462) in Shaanxi Province, Northwest China, 2013

* The number of missing values for maternal age at delivery, parity, maternal education and per capita annual household income was 58, 1, 21 and 1112, respectively.
Status of dietary intakes of energy and nutrients
Daily intakes of fat, Ca and Fe among pregnant women in Shaanxi, China were higher than those among pregnant women in the 2002 NNHS, while daily intakes of energy and other nutrients were lower than those in the 2002 NNHS. The percentage of energy derived from fat was higher than that among pregnant women in the 2002 NNHS (34 v. 31 %), while the percentages from protein and carbohydrate were similar to those in the 2002 NNHS.
Intakes of energy, protein and carbohydrate were higher than the reference values for pregnant women during the first trimester and close to the reference values of the second and third trimesters. Fe intake was higher than the nutrient reference values for women during the first and second trimesters of pregnancy, and close to the reference value of the third trimester. Pregnant women in Shaanxi, China had higher intakes of fat, niacin and vitamin E than the nutrient reference values for any trimester of pregnancy. The median percentage of energy from fat (34 %) was higher than the upper limit of the recommended range for fat (30 %). In fact, 72 % of participants had more than 30 % energy derived from fat and only 25 % of participants had the recommended range of energy derived from fat (20–30 %). However, other micronutrients such as vitamin A, thiamin, riboflavin, folate, vitamin C, Ca and Zn had low reported intakes (their intakes were below 65 % of the RNI/AI for all three gestational periods; Table 2).
Table 2 Daily energy and nutrient intakes of pregnant women (n 7462) in Shaanxi Province, Northwest China, 2013
RNI, recommended nutrient intake; RE, retinol equivalent.
* Values presented are RNI except for vitamin E, for which the adequate intake is given; RNI for pregnant women aged 18–49 years with low physical activity level during each trimester( 27 ).
† Percentage of the RNI that the median daily intake in the population accounts for.
Dietary intakes across sociodemographic groups
Geographic area
Median daily intakes of energy and selected nutrients across sociodemographic groups are presented in Table 3. Compared with participants from northern Shaanxi, pregnant women from central Shaanxi had higher intakes of energy and all selected nutrients. Pregnant women from central Shaanxi also had higher intakes of energy and most nutrients and lower intakes of fat and vitamin E relative to those from southern Shaanxi. For participants from northern and southern Shaanxi, intakes of fat, carbohydrate, vitamin E and Fe were significantly different.
Table 3 Median daily intakes of energy and selected nutrients according to sociodemographic group of pregnant women (n 7462) in Shaanxi Province, Northwest China, 2013

RE, retinol equivalent.
* Significant differences were found using the Wilcoxon two-sample test (P<0·017) in: (i) all selected nutrient intakes for central Shaanxi v. southern Shaanxi; (ii) all selected nutrient intakes for central Shaanxi v. northern Shaanxi; and (iii) intakes of fat, carbohydrate, vitamin E and Fe for southern Shaanxi v. northern Shaanxi.
† Significant differences were found in all selected nutrient intakes except carbohydrate (P=0·24) between the two groups using the Mann–Whitney U test (P<0·05).
‡ Significant differences were found using the Wilcoxon two-sample test (P<0·017) in: (i) all selected nutrient intakes for <25 years v. 25–29 years; (ii) all selected nutrient intakes except fat (P=0·032), carbohydrate (P=0·088) and Ca (P=0·107) for <25 years v. ≥30 years; and (iii) Ca intake for 25–29 years v. ≥30 years.
§ Significant differences were found using the Wilcoxon two-sample test (P<0·017) in: (i) all selected nutrient intakes for primary school or below v. senior high school or above; (ii) all selected nutrient intakes for junior high school v. senior high school or above; and (iii) all selected nutrient intakes except niacin (P=0·04) for primary school or below v. junior high school.
|| Significant differences were found in all selected nutrient intakes between the two groups using the Mann–Whitney U test (P<0·05).
¶ Significant differences were found using the Wilcoxon two-sample test (P<0·017) in: (i) all selected nutrient intakes for <6200 v. ≥12 000; (ii) all selected nutrient intakes except carbohydrate (P=0·803) for 6200–11 999 v. ≥12 000; and (iii) all selected nutrients intakes except carbohydrate (P=0·033), vitamin A (P=0·046), folate (P=0·047) and vitamin E (P=0·032) for <6200 v. 6200–11 999.
Residence
Women living in urban areas reported significantly higher intakes of energy and all selected nutrients except carbohydrate during pregnancy, compared with those in rural areas.
Maternal age at delivery
Pregnant women aged 25–29 years at delivery consumed significantly more nutrients than those aged <25 years at delivery. Significant differences also existed in most selected nutrient intakes for the 25–29 years group v. the ≥30 years group, while only Ca intake was significantly different between the <25 years and ≥30 years groups.
Maternal education
Women in the highest education subgroup had significantly higher intakes of energy and all selected nutrients during pregnancy than those in the medium and lowest education subgroups. Moreover, participants in the medium education subgroup had significantly higher consumption of all nutrients except niacin compared with those in the lowest education subgroup.
Maternal occupation
Pregnant women with paid employment outside their home reported significantly higher intakes of energy and all selected nutrients relative to those categorized as farmers.
Household income
Women in the highest household income subgroup consumed significantly more energy and nutrients during pregnancy than those in the lowest and medium subgroups. Compared with those in the lowest household income subgroup, participants in the medium household income subgroup had significantly higher intakes of energy and all selected nutrients except carbohydrate, vitamin A, folate and vitamin E.
Food groups contributing to nutrient intakes
The top five food groups that contributed to the intakes of energy and selected nutrients are shown in Table 4. Snacks, meats, oils, nuts and sweets contributed most to energy intake, accounting for about two-thirds of total energy intake. Seventy-five per cent of total protein intake came from meats, legumes, vegetables, snacks and fish. Oils, meats, nuts, snacks and legumes contributed 86 % of total fat intake. Carbohydrate intake was derived mainly from snacks, vegetables, sweets, cereals and fruits. The food group contributing most to the intakes of vitamin A, thiamin, riboflavin, niacin and Zn was meat, followed by vegetables. About three-quarters of total folate intake was derived from vegetables, legumes and nuts, and about 90 % of total vitamin C intake was from vegetables and fruits. More than 70 % of total vitamin E was derived from nuts, oils and legumes. A total of 81 % of Ca intake was derived from the top five food groups shown in Fig. 1(a), with vegetables accounting for about 30 % of total Ca. Vegetables was also the top food resource of Fe intake, followed by legumes and meats (Fig. 1(b)).
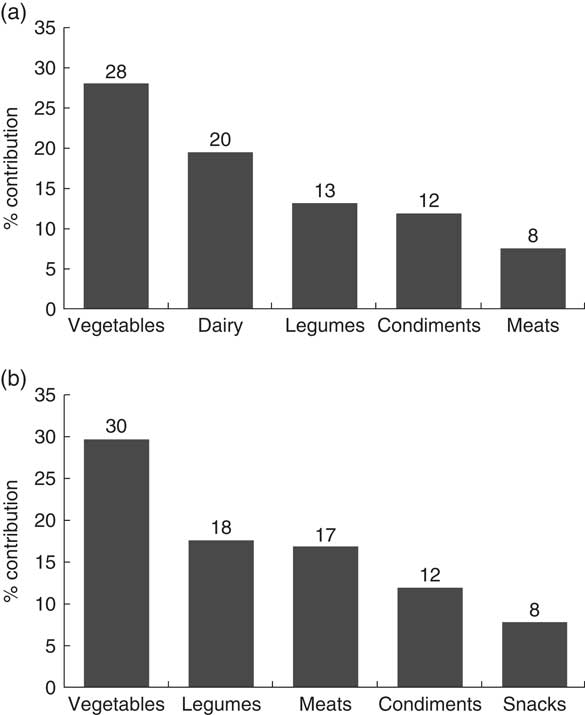
Fig. 1 Food groups contributing to (a) calcium intake and (b) iron intake among pregnant women (n 7462) in Shaanxi Province, Northwest China, 2013
Table 4 The top five food groups contributing to energy and selected nutrient intakes among pregnant women (n 7462) in Shaanxi Province, Northwest China, 2013

* Percentage of the nutrient intake derived from the food group
† Snacks included ethnic snacks such as Chinese cakes and cold noodles and fast foods such as biscuits, breads, dumplings, rice crust and instant noodles.
‡ Meats included products from livestock such as pig, beef and lamb.
Dietary patterns
Three dietary patterns were extracted by principal component analysis (Table 5). The Kaiser–Meyer–Olkin value was 0·800 and the P value of Bartlett’s test of sphericity was <0·0001. A total of 33·5 % of the variability in food intake was explained by the three patterns, with the first explaining 18·3 %, the second explaining 8·4 % and the third explaining 6·8 %. The first pattern had high positive loadings from various foods including meats, fungi, vegetables, fish, dairy, legumes, eggs, nuts, fast foods and fruits; this pattern was labelled the ‘balanced pattern’. The second pattern, which was labelled the ‘vegetarian pattern’, had high positive loadings from plant-based foods including potatoes, cereals, vegetables, fruits and legumes and high negative loadings from sweets, condiments and oils. The third pattern was labelled the ‘snacks pattern’, with food groups such as beverages, sweets, ethnic snacks, fast foods, potatoes and vegetables loading highly on this pattern.
Table 5 Factor loadings for the identified dietary patterns among pregnant women (n 7462) in Shaanxi Province, Northwest China, 2013

* Food groups are listed by the size of factor loadings, with negative loadings at the end. Food groups with absolute factor loadings <0·25 are not shown.
Associations of dietary patterns with sociodemographic characteristics and nutrient intakes
Sociodemographic characteristics and daily intakes of energy and nutrients according to quartiles of dietary patterns scores are organized in Table 6. Pregnant women with high scores on the balanced pattern were more likely to live in central Shaanxi, urban areas, be aged 25–29 years at delivery and be better educated, while those with high scores on the vegetarian pattern and the snacks pattern lived in central and southern Shaanxi respectively, rural areas, were aged <25 years at delivery and less educated. Pregnant women with high scores on the balanced pattern were also more likely to be wealthier and work outside, while participants with high scores on the snacks pattern were poorer and worked as farmers. No significant differences were found in the association of vegetarian pattern scores with maternal occupation and household income.
Table 6 Sociodemographic characteristics and median daily intakes of energy and nutrients according to quartiles of dietary patterns scores among pregnant women (n 7462) in Shaanxi Province, Northwest China, 2013
Q, quartile; RE, retinol equivalent.
* P values for the differences among the groups of dietary pattern scores were derived from the χ 2 test for categorical variables and the Kruskal–Wallis test for continuous variables.
† Values are presented as percentages for these categorical variables.
Women with higher scores on the balanced pattern had higher intakes of energy and all selected nutrients. Participants with higher scores on the vegetarian pattern had higher energy intake, lower fat intake and higher intakes of other selected nutrients. Significant differences were also found in energy and nutrient intakes among the four groups of the snacks pattern. Median daily dietary intakes in the first quartile group of the snacks pattern were higher than those in the second quartile group, while the median intakes gradually increased from the second to the fourth quartile group. In addition, energy and nutrient intakes were higher in the third and fourth quartile groups of the balanced pattern compared with the corresponding quartile groups of the vegetarian pattern and snacks pattern (all P<0·001).
Discussion
In the current population-based cross-sectional study, we found that pregnant women in Shaanxi, China had higher intakes of fat, niacin and vitamin E than the RNI, while most micronutrients such as vitamin A, folate, Ca and Zn were reportedly lower than the RNI. Three dietary patterns were identified among the participants: balanced pattern, vegetarian pattern and snacks pattern. The study suggested that dietary patterns and most nutrient intakes varied by sociodemographic groups in the population. Pregnant women with high scores on the vegetarian pattern and snacks pattern tended to be in low balanced pattern score groups and had lower nutrient intakes compared with those in high balanced pattern score groups.
Differences in dietary intake recommendations exist among countries, with some nutrients regarded as adequate and others as inadequate at the same intake levels( Reference Blumfield, Hure and Macdonald-Wicks 30 ). The adequate intake levels of some nutrients among pregnant women in Europe may be classified as inadequate in China, such as Ca and Zn. Moreover, the recommended intake levels in China may be lower than those in the USA, such as the recommended proportion of fat derived from energy (China v. America: 20–30 % v. 20–35 %). Possible reasons for the disparities include distinct genetic backgrounds, dietary habits, disease burdens, available scientific evidence and the extrapolation methods adopted when experimental data were insufficient. Thus, it is important to appropriately use the dietary reference tools and cautiously interpret when comparing nutrient intakes across geographic regions.
Our finding of high fat intake (the percentage of energy from fat, 34 %, was higher than the upper limit of the recommended range for fat in China, 30 %) was consistent with previous reports of pregnant women in China( Reference Liu, Zhang and Pares 17 , Reference Wang, Zhao and Piao 31 ), which may be partially due to the increasing consumption of oils and animal-source foods during the last decade. Pregnant women in Western developed countries also reported fat intakes above recommendations, at 35·0–37·1 % of energy( Reference Blumfield, Hure and Macdonald-Wicks 32 ). The high fat intake contributed to the excessive energy derived from fat in our study, suggesting the tendency to consume more energy-dense foods among pregnant women in China. This tendency might lead to excessive weight gain during pregnancy and further influence maternal and children’s health, including the risk of obesity, diabetes, CVD and metabolic syndrome( Reference Crozier, Inskip and Godfrey 33 , Reference Gilmore, Klempel-Donchenko and Redman 34 ). The increasing intakes of animal-source foods also contributed to the relatively high intake of niacin, which was similar to the previous study in China( Reference Wang, Zhao and Piao 31 ). Vitamin E intake was about 1·75 times higher than the reference value, but less than the tolerable upper intake level (700 g). The high vitamin E intake may be explained by the constant consumption of nuts and oils among this population.
Dietary intake of vitamin A was lower than 40 % of the RNI among the participants. In fact, more than 70 % of pregnant women in the study had inadequate intake of vitamin A compared with the estimated average requirement from the Chinese Dietary Reference Intakes 2013 (480 g, 530 g and 530 g for the three trimesters of gestation, respectively), indicating that food-derived vitamin A deficiency was a prominent problem among pregnant women in Shaanxi, China. A previous study reported that 70 % of total vitamin A was derived from plant-based foods among Chinese women( Reference Yin 14 ); however, our study found that meats accounted for 67·1 % of total vitamin A and vegetables accounted for 19·6 %, suggesting that the dietary habits of pregnant Chinese women may have changed gradually over the last decade. The inadequate vitamin A intake may be due to the low consumption of vitamin A-rich foods such as fish, animal liver and carrots among the population in Shaanxi, China. It is worth noting that folate intake was insufficient among the participants, which was supported by the finding of low plasma folate concentration among women in Shaanxi, China( Reference Dang, Yan and Zeng 20 ). Dietary intake of folate is also widely reported to be below the recommended level among pregnant women in developed countries( Reference Blumfield, Hure and Macdonald-Wicks 30 ), indicating the universality of poor dietary folate intake among pregnant women and the difficulty of meeting the increased folate demand in pregnancy with dietary intake( Reference Lee, Talegawkar and Merialdi 35 ).
Dietary intake of Ca was found to be notably higher than the intake reported in the 2002 NNHS, which may be explained by the increasing consumption of Ca-rich foods such as dairy and legumes. However, Ca intake was still below the RNI of any trimester. Zn intake was also below the RNI. Moreover, plant foods accounted for a relatively high proportion of total Ca and Zn intakes. The plant foods including cereal grains, nuts and legumes that were relatively frequently consumed in the current population contain high levels of phytate, an inhibitor of Ca and Zn absorption( Reference Weaver, Proulx and Heaney 36 , Reference Hunt 37 ). Thus, the bioavailability of Ca and Zn may be impaired among the population. Fe intake was higher than the average level in the 2002 NNHS and close to the RNI of the third trimester, which is different from the high prevalence of dietary Fe inadequacy during pregnancy in developed countries( Reference Pinto, Barros and dos Santos Silva 38 , Reference Turner, Langkamp-Henken and Littell 39 ). However, Fe absorption may be poor among the participants because dietary Fe was derived mainly from plant foods. Plant foods contain only non-haem Fe, whereas animal-source foods contain both non-haeme Fe and haem Fe. Non-haem Fe is much less well absorbed than haem Fe( Reference Hurrell and Egli 40 ), with an estimated absorption rate of 2·8 % from the intakes of cereals, legumes and vegetables( Reference Thankachan, Muthayya and Walczyk 41 ). Vitamin C in plant foods is recognized to enhance Fe absorption( Reference Cook and Monsen 42 ); however, the low intake of vitamin C among the participants may hardly exert much enhancing effect on Fe absorption.
Previous studies have suggested the association of dietary intakes with socio-economic status and demographic group( Reference Lai, Yin and Ma 18 , Reference Smith and Baghurst 43 – Reference Novakovic, Cavelaars and Geelen 47 ). People of higher socio-economic status (education, occupation or income) tend to report higher intakes of energy, macronutrients( Reference Larranaga, Santa-Marina and Begiristain 46 ) and most micronutrients such as vitamin A, folate, Ca, Fe and Zn( Reference Junior, Cesar and Fisberg 45 , Reference Novakovic, Cavelaars and Geelen 47 ). Our results also suggested that pregnant women in the highest education, occupation and household income groups had significantly higher intakes of all selected nutrients than those in the lowest groups. Moreover, pregnant women in urban areas reported higher intakes of most nutrients than those in rural areas, which is in agreement with the previous study conducted in China( Reference Lai, Yin and Ma 18 ). The findings may be partially due to the fact that people with higher socio-economic status or living in urban areas may have more opportunity to attain nutrition knowledge and pay more attention to their dietary quality. In our study, pregnant women with age at delivery of 25–29 years were found to have higher intakes of some nutrients than those in the lowest and highest age groups. A potential reason for this is that women who have a baby at the age of 25–29 years are more concerned about maternal and child health and then consume foods more selectively. Pregnant women in the three different geographic areas of Shaanxi, China also reported significant differences in some nutrient intakes, with the pregnant women in central Shaanxi having higher intakes of most nutrients. These results indicate that targeted programmes are needed to improve nutritional status among pregnant women from disadvantaged sociodemographic groups.
Dietary patterns represent a broader picture of food and nutrient intakes, and reflect overall dietary behaviour among the study population( Reference Hu 48 ). Three dietary patterns were identified: balanced pattern, vegetarian pattern and snacks pattern. The results suggested that pregnant women with high adherence to the balanced pattern tended to consume more energy and nutrients than those highly adhering to the vegetarian pattern and snacks pattern. Moreover, participants with high adherence to the balanced pattern were more likely to be better educated, wealthier, 25–29 years old at delivery, working outside and living in urban areas and central Shaanxi, which is consistent with the results of more energy and nutrient intakes among these sociodemographic groups. The balanced pattern identified in our study was comparable to the prudent pattern reported among pregnant women in Guangzhou, China( Reference He, Yuan and Chen 49 ), in which the high educational level was also found to be associated with a high pattern score. However, the vegetable pattern identified in Guangzhou was reported to be positively associated with education and income level( Reference He, Yuan and Chen 49 ), which is different from the results of the vegetarian pattern in our study. The difference may be partly due to the geographical disparity between Guangzhou, in southern China, and Shaanxi, in northern China, with distinct dietary habits identified among these people( Reference Zhang, Wang and Wang 50 ). Pregnant women with high adherence to the vegetarian pattern and the snacks pattern tended to be in the groups with low balanced pattern scores, and to have lower nutrient intakes compared with those with high adherence to the balanced pattern. The findings emphasize the importance of targeted programmes to improve the dietary patterns among sociodemographically disadvantaged pregnant women. Dietary patterns study may have great public health significance because the overall patterns might be easy for the public to interpret into daily diets. Further studies are needed to explore the associations of dietary patterns with pregnancy outcomes and pregnancy complications among pregnant women in Shaanxi Province of North-west China.
To our knowledge, the present study is the first large-scale nutrition survey in Northwest China. The study was performed in Shaanxi Province of Northwest China using a stratified multistage random sampling method according to the proportion of rural to urban residents, population size and fertility rate. Thus, the sample represented pregnant women in Shaanxi, China and the study results partly reflected the status of pregnant women in China. However, some limitations of the current study should be acknowledged. First, dietary intake was retrospectively self-reported by the participants. Women in the present study recalled diet during pregnancy that was 0 to 12 months (median 3 months; 10th–90th percentile 0–7 months) prior to answering the survey. Previous findings have suggested that pregnancy diet can be recalled rather well even after several years( Reference Bunin, Gyllstrom and Brown 51 , Reference Bosco, Tseng and Spector 52 ). Despite this, we cannot rule out the possible limitation of recall bias. To minimize bias, we made efforts to help mothers provide accurate responses during the survey. For one thing, standard questionnaires and detailed supporting materials such as food portion images and calendars were used to collect information. For another, the survey was tested in a pilot study and interviewers were rigorously trained according to the detailed guides before the formal investigation. Second, nutrient intakes were computed on the basis of the China Food Composition Tables which have been specifically created according to the food analyses in China. However, the calculation of nutrient contents in the food composition tables assumed that the nutrients in foods were constant among regions in China. Although multiple food samples were used to analyse the nutrient compositions, this sampling may not be nationwide for all foods( 25 , 26 ). Third, we did not collect blood samples from the population; thus, nutritional biomarkers of the participants such as serum Hb, plasma folate and homocysteine were not considered. The nutritional biomarkers may help us further understand the nutritional status of the population and explore the relationship between dietary patterns and nutritional status.
Conclusion
In conclusion, the present study suggested that pregnant women in Shaanxi Province of Northwest China had low intakes of most nutrients such as vitamin A, folate and Ca. Three dietary patterns were identified in the population: balanced pattern, vegetarian pattern and snacks pattern. Dietary patterns and most nutrient intakes varied by sociodemographic groups among the participants. Targeted programmes such as nutrition education, food fortification and multi-micronutrient supplementation are needed to improve the dietary intakes and dietary patterns among sociodemographically disadvantaged pregnant women.
Acknowledgements
Acknowledgements: The authors are grateful to all mothers who participated in this study, all staff who coordinated fieldwork and all investigators who contributed to data collection. Financial support: This work was supported by the National Natural Science Foundation of China (grant number 81230016). The National Natural Science Foundation of China had no role in the design, analysis or writing of this article. Conflict of interest: None. Authorship: J.Y., S.D., Y.C., L.Z. and H.Y. conceived and designed the study; J.Y., S.D., Y.C., L.Z., H.Q., B.M., Y.J., P.Q., Q.W., Q.L., Y.K. and Y.S. collected and cleared the data; J.Y., H.Q., B.M. and Y.J. analysed and interpreted the data; J.Y., S.D., Y.C. and H.Y. drafted and revised the manuscript. All authors read and approved the final version of the manuscript. Ethics of human subject participation: This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving human subjects were approved by the Xi’an Jiaotong University Health Science Center (number 2012008). Written informed consent was obtained from all subjects.







