


Non-communicable diseases (NCDs) including cardiovascular disease (CVD), type 2 diabetes, cancers and obesity-related conditions now account for some 60% of global deaths and almost half (47%) of the global burden of disease1. NCDs no longer principally touch high-income countries: low- and medium-income countries are increasingly implicatedReference Caballero and Popkin2, Reference Delpeuch and Maire3, as highlighted in the World Health Organization's (WHO) Global Strategy on Diet, Physical Activity and Health1. The WHO strategy addresses diet and physical activity, two of the major risk factors responsible for the growing burden of NCDs, and emphasises the need to limit consumption of salt, saturated fats and refined sugars, and to increase consumption of vegetables and fruit and levels of physical activity. It also identifies the need to address the role of consumer education and communication.
One of the obstacles to slowing down the increase of obesity and nutrition-related chronic disease in some low- and medium-income countries could be a lack of individuals' knowledge of their causes and relationship to factors such as poor diet and lack of physical activity. Certainly, lack of awareness of healthy behaviours by the general public in Africa is perceived as one contributory factor to NCDs4 and it has been proposed that the low level of formal education, especially in women, justifies emphasis on knowledge dissemination in AfricaReference Nyamwaya5. Even so, there are few studies in sub-Saharan Africa to date to substantiate this, which is to be expected given that NCDs are a relatively recent public health problem, with the exception of South AfricaReference Peltzer6.
Although some dietary knowledge is necessary to persuade individuals to choose health-promoting behavioursReference Holdsworth, Haslam and Raymond7–9, it is acknowledged that it still remains only one predisposing factor influencing the complex behaviour of eatingReference Green and Kreuter10, alongside factors such as attitudes, risk perception and social normsReference McCaffery, Wardle and Waller11. Accurate nutritional knowledge may be particularly important when individuals are ready to make dietary changesReference Holdsworth, Haslam and Raymond7 and when combined with behavioural and motivational strategiesReference Anderson, Cox, McKellar, Reynolds, Lean and Mela12. Early studies have been sceptical about the potential changes in behaviour that could result from enhancing knowledge, but the tools used to assess dietary knowledge have often been imprecise and rarely tested for their validity and reliability in measuring what was intended, making it difficult to judge if the findings were accurate. Nutrition knowledge tools have since been developedReference Parmenter and Wardle13–Reference Whati, Seneka, Steyn, Nel, Lombard and Norris15 which appear to be more sensitive at measuring dietary knowledge, as well as knowledge of the diet–NCD relationship. However, these do not contain the level of precision on the dietary and behaviour–NCD relationship needed for the current study.
Almost half of Senegal's inhabitants are urban, a figure which is set to increase, and a quarter of the Senegalese population lives in the region of the capital, Dakar. Obesity prevalence of women in a district of Dakar has doubled since 1996 and has recently been estimated at 18.6%Reference Holdsworth, Gartner, Landais, Maire and Delpeuch16. The likelihood that obesity is set to stay means that the wide range of determinants of obesity in this context need to be explored, including understanding of the causes and consequences of NCD, to help inform future preventive strategies. The purpose of the current study of these urban Senegalese women was to assess their knowledge of dietary and behaviour-related determinants of NCD, to identify gaps in knowledge that could be the target for future public health nutrition programmes.
Methods
Target population and sampling
The target population was Senegalese women aged 20–50 years living in Dakar. The sampling frame was the district of Pikine Ancien. This district (population of about 100 000 inhabitants) was chosen because it is the most diverse in terms of coverage of all sociodemographic groups in the large town of Pikine (population of about 1 million inhabitants). Although we cannot refer to how representative our sample is in statistical terms on a wider scale, we can say that the district of Pikine Ancien is by no means atypical of the rest of Pikine or Dakar in sociodemographic or cultural terms.
Approval was granted in April 2003 by the local ethical committee (Chief Medical Officer, Pikine District). Informed oral consent was obtained from each subject during recruitment. Fieldwork was carried out during April–June 2003 in Wolof (language understood by all). All interviews were conducted verbally by the same trained female interviewer, supervised by a female researcher at all times (E.L.).
Using a recent map, 310 compounds (a dwelling that several households may share) were randomly selected using random number tables; the additional 10 compounds were sampled to provide a replacement pool in case of refusals or where compounds no longer existed. One household (if the compound comprised more than one) was randomly selected using a die at the interior of the compound. Only one woman was randomly selected from this household to avoid any bias from potential clustering of knowledge within the same compound. On average 10 people comprise a household in Pikine.
Development and validation of the questionnaire
The questionnaire was composed of 24 items in total (Table 1). All items were developed specifically for this study, except for items 16 and 17 which were based on those used previouslyReference Swift, Glazebrook and Macdonald17. Questions were chosen on areas of knowledge with high scientific consensus about the causality of NCD, so that items were clearly unequivocally true or false. Areas of knowledge of modifiable behaviours were targeted to be able to inform intervention programmes. The questionnaire was pre-tested for face validity with 10 Senegalese women drawn from a population within Dakar. It was developed in French and was translated into Wolof, which was the language used for interviews, and then translated back into French to check that none of the meaning had been lost. Piloting ensured that ambiguous and confusing questions were identified and re-phrased. Although questions where the correct response was ‘false’ were included at the piloting stage, only one such question was retained after piloting. This was for several reasons. First, in terms of language, as negatively phrased questions were not well understood and some of these were perceived as patronising by the women as too obviously incorrect. Second, it has been recognised that adults with lower cognitive skills/formal educational level are more easily confused by questions where they have to answer ‘no’ for a correct response, leading to lower validity coefficientsReference Streiner and Norman18, and simply reversing the polarity of an item does not necessarily reverse its meaning.
Table 1 Questionnaire items
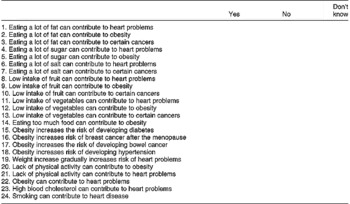
All responses are true except item 4.
Items presented here in the order that they appeared on the questionnaire.
The items were used to construct six knowledge domain scores: Score 1 – dietary and behaviour-related causes of NCD; Score 2 – diet quality–NCD relationship; Score 3 – fruit and vegetables link with NCD; Score 4 – health consequences of obesity; Score 5 – causes of CVD; and Score 6 – causes of certain cancers; all items were used for more than one of these knowledge domains (Table 2). These scores are mutually exclusive in their ability to measure their domain of knowledge. The six knowledge domain scores passed the criteria for internal consistency, item discrimination and item difficulty in the final sample of 301 women (Table 2).
(1) Internal consistency: The reliability of each set of items in measuring each domain indicated that item-to-item correlation was acceptable (Table 2) using Cronbach's α for all domain scores except Score 6 (α = 0.69), which was marginally below the suggested cut-off point of 0.7. Even so, this was retained because item discrimination and difficulty, as well as content validity, were convincing.
(2) Item discrimination: The ability of each individual item to discriminate between women with different levels of knowledge, i.e. highest 27% versus lowest 27%, was measured by correlating the response on each item with the scoreReference Kelley19. All items had an item-to-item score correlation of >0.2, below which items are considered too weakReference Streiner and Norman18.
(3) Item difficulty: Eighteen of the 24 items (Table 2) fell within the recommended range of 20–80% of correct responsesReference Anderson, Bell, Adamson and Moynihan14, Reference Kline20. Three of the remaining six items were too easy (88.4% correctly answered ‘obesity increases risk of hypertension’, 81.1% that ‘lack of physical activity can contribute to obesity’ and 81.4% that ‘eating a lot of fat can contribute to heart problems’) and three were too difficult (13.3% correctly answered ‘low intake of fruit can contribute to certain cancers’, 17.9% correctly answered ‘low intake of vegetables can contribute to obesity’ and 14.6% correctly answered ‘low intake of vegetables can contribute to certain cancers’). Even so, these items were retained on the grounds of content validity, as they were testing a crucial facet of the diet–NCD relationship not otherwise addressed in the questionnaire.
Table 2 Internal reliability of knowledge domain scores

NCD – non-communicable disease; CVD – cardiovascular disease.
* Item numbers correspond to those listed in Table 1.
Demographic, socio-economic and nutritional measures
Age, written literacy, education level, employment status and ethnicity were assessed. Economic level was estimated by the presence in the compound of dwelling utilities (electricity, running water), appliances (refrigerator, freezer) and ability to purchase staple food in advance. A synthetic index of economic level was constructed with multiple correspondence analyses on this matrix of indicator variables, based on an approach developed previouslyReference Martin-Prevel, Traissac, Delpeuch and Maire21. The first principal component of the correspondence analysis displayed a gradient of household wealth. The economic index developed classified households into three distinct groups of ‘low’, ‘average’ and ‘high’ economic level. Body mass index (BMI) was assessed from measured weight and height; weight was measured using scales accurate to 100 g, which were verified daily, and height was measured using a portable height measurer to the nearest mm. BMI data were classified into two groups for cross-tabulations: ‘underweight/normal’ and ‘overweight/obese’.
Data management and analyses
Data from questionnaires were entered twice by the same investigator (E.L.) in two separate files using EpiData (version 3; The EpiData Association, Odense, Denmark), their output was then compared by another researcher (A.G.) and the corrections identified and inputted. SPSS (version 11.5; SPSS Inc., Chicago, IL, USA) was used for descriptive analyses and ADE-4Reference Thioulouse, Chessel, Dolédec and Olivier22 was used for correspondence analysis when developing the economic index. Knowledge domain scores were attributed as follows: correct response = 1; incorrect response = 0; unsure/don't know = 0. The ‘unsure/don't know’ category was included to discourage bias from guessingReference Parmenter and Wardle13. Knowledge scores were standardised as percentages so that they could be compared. In the development of the scores, obesity was treated as an NCD, not one of the determinants. The relationship between the six knowledge scores and sociodemographic variables (economic level, employment status, age, BMI, literacy, ethnicity and education level) were investigated using the Kruskal–Wallis test. Differences were considered statistically different at the P < 0.05 level.
Results
Characteristics of the sample
The overall response rate was 97.1%, as 301 of the 310 randomly selected women agreed to participate and form the final sample. Wolof was the major ethnic group (45.2%) (Table 3). About two-thirds of women had received either no school education (35.9%) or only primary school level education (32.9%), almost over half of respondents reported being illiterate (47.8%). Only a quarter of women reported working outside the home (26.1%), and almost half of these (46.3%) were market/shop keepers. The majority of households had electricity (91.0%) and running water (89.7%) and nearly half owned a refrigerator (48.8%). Almost half the women (45.2%) were classified as either overweight (26.6%) or obese (18.6%).
Table 3 Characteristics of the sample (n=301 women)
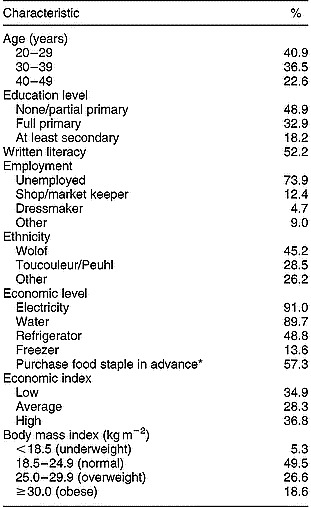
* At the beginning of the month.
Knowledge of diet and behavioural determinants of NCDs
Knowledge was understood better for the dietary fat–NCD relationship (Table 4) as the percentage of correct responses ranged between 49.8 and 81.4% according to the item, whereas they were lower for the sugar–NCD link (correct responses ranged from 32.6 to 54.5%). For example, the item ‘eating a lot of fat can contribute to heart problems’ was widely understood, with 81.4% of women answering correctly. Knowledge of the salt–NCD relationship was slightly lower, with correct responses in the range of 26.3–56.3%. However, the least well understood association was that between NCDs and low intake of fruit and vegetables (correct responses ranging between 13.3 and 31.6%); for example, only 13.3% of women correctly answered that a ‘low intake of fruit can contribute to certain cancers’.
Table 4 Correct responses for individual knowledge items (n=301 women)

Items presented here in the order that they appeared on the questionnaire.
Almost three-quarters of women were aware that eating too much food could cause obesity, whereas less were aware of the contribution of eating a lot of sugar (54.5%) and fat (59.5%) to obesity development (Table 4). Obesity as a risk factor for CVD was well understood, with 88.4% of women acknowledging that obesity could lead to hypertension and 75.4% agreeing that ‘weight increase gradually throughout life increases risk of developing heart problems’. Smoking as a CVD risk factor was also well understood (73.8% correct), as was fat consumption (81.4% correct). However, eating a lot of fat was seen to have more impact on CVD risk than development of obesity (59.5% correct). Over two-thirds of women (Table 4) were aware that high blood cholesterol was a CVD risk factor. A lack of physical activity was seen as having more impact in contributing to obesity (81.1% correct) than CVD development (58.8% correct).
Knowledge of the health consequences of obesity
The effect of obesity on CVD was generally well understood (Table 4), but its impact on certain cancers was less well known, less so for breast cancer (52.8% correct) than for bowel cancer (59.1% correct). Over half of the sample (59.1%) was aware that obesity could impact on life expectancy. However, the least well understood health consequence of obesity was its potential impact on the development of diabetes (51.2% correct).
Knowledge scores
The knowledge scores developed (Table 5) suggest that the health consequences of obesity (mean score of 65.4%) were best understood. Amongst the determinants of NCDs, the causes of certain cancers were less well understood than for CVD (Table 5). Knowledge of the protective effect of vegetables and fruit was least well known (mean score of 19.9%). No relationship was found between knowledge scores and women's age, economic level, literacy, education level, BMI or ethnicity. However, women who worked outside the home had significantly better knowledge than those unemployed for Scores 1 and 2 (P < 0.05).
Table 5 Scores for the six domains of knowledge measured

NCD – non-communicable disease; CVD – cardiovascular disease.
* Mean percentage of correct responses.
† Median percentage of correct responses.
Discussion
The purpose of this study was to assess knowledge of dietary and behaviour-related determinants of NCDs in urban Senegalese women, to identify gaps in knowledge that could be the target for future public health nutrition programmes. Overall, the findings suggest reasonable overall knowledge concerning dietary and behaviour-related causes of NCDs, especially given the relatively new context of the obesity epidemic in Senegal. However, there was particularly poor knowledge of the benefit of eating plenty of vegetables and fruit in preventing obesity, CVD and certain cancers. Knowledge of the potential for preventing cancers was least understood, whereas it was widely understood for CVD. These trends are similar to those reported in previous studies conducted in high-income countriesReference Parmenter, Waller and Wardle8, Reference Sapp and Jensen23.
The knowledge scores constructed suggest that women had less knowledge about the causes of NCDs than about the consequences of obesity. This could result from their direct or indirect life experiences of the consequences of obesity. However, the non-dietary causes of NCDs appear to be better understood than the dietary risk factors alone, which suggests that education should particularly focus on the dietary aspects. Contrary to expectations, no relationship was found between knowledge scores and economic level, literacy or formal education. This contrasts with studies in the USAReference Peltzer6, UKReference Parmenter, Waller and Wardle8 and South AfricaReference Peltzer6 that reported a relationship between formal education and knowledge. However, women who worked outside the home had better knowledge for two scores, suggesting that contact with the wider community is perhaps more important in determining current knowledge than previous formal education or literacy level. It was also anticipated that obese women would have a better knowledge of the causes and consequences of obesity, but this was not the case; one possible explanation could be that as over 45% of women are overweight or obese, the condition is so widespread that all women have direct experience of overweight/obesity.
The questionnaire successfully measures six domains of knowledge of the diet and lifestyle–NCD relationship, as they passed criteria for content validity, item discrimination, item difficulty and internal consistency. This knowledge questionnaire could also be used in other countries, including those where low literacy is prevalent, as items are not only specific to Senegal. However, it would need to be tested for item discrimination and content validity in the target population. There are limitations of the tool. Due to the small sample of women used for piloting and time constraints in conducting fieldwork, construct validity tests were conducted after data collection on the whole sample of women in the final study, rather than on the pilot sample. Even so, the fact that the tool passed these criteria in the whole sample does not reduce its content validation.
The findings suggest that education targeting the benefits of vegetables and fruit may have the greatest impact on knowledge, given the general low understanding. A recent review of fruit and vegetable consumption patterns in sub-Saharan AfricaReference Ruel, Minot and Smith24 reported low consumption, and our study of fruit and vegetable intake in Senegalese women concurs with this (data not presented here). A further reason for focusing on awareness of the benefits of fruit and vegetables is that increasing intake could have a potentially high impact in reducing many NCDsReference Lock, Pomerleau, Causer, Altmann and McKee25. However, nutrition education messages need to be communicated within the context of a whole diet approach9 supported by simple, clear, positive food-based messagesReference Kelly and Stanner26 and take account of attitudes, risk perception and social norms, e.g. the desirability of overweight body sizes in urban women is a potential barrier to change in SenegalReference Holdsworth, Gartner, Landais, Maire and Delpeuch16. It may also be important to target those areas of knowledge which are well understood by the population as these may be more malleable to behaviour change. Women's knowledge was of particular relevance given their role in food purchasing and cooking responsibilities. However, future studies need to evaluate men's knowledge to identify if the pattern is similar, to inform a population-wide approach to improving knowledge.
This will require the development, evaluation and promotion of food-based dietary guidelines, culturally relevant to Senegal, as a tool for nutrition education; using a similar development process to that of other countriesReference Hunt, Rayner and Gatenby27–Reference Vorster, Love and Browne29. Practical education strategies such as cooking, tasting and eating may be most effective, as education without associated skills development is likely to result in limited behaviour change.
Acknowledgements
The authors are grateful to the women of Pikine for participating so willingly in this study and to both Mame Sylla Diagne and Khady Diop for their invaluable work in the field.





