
162 results
76 Lessons learned during implementation of OMOP common data model across multiple health systems
- Part of
-
- Journal:
- Journal of Clinical and Translational Science / Volume 8 / Issue s1 / April 2024
- Published online by Cambridge University Press:
- 03 April 2024, p. 20
-
- Article
-
- You have access
- Open access
- Export citation
Emergency Medical Services Protocols for Assessment and Treatment of Patients with Ventricular Assist Devices
-
- Journal:
- Prehospital and Disaster Medicine , First View
- Published online by Cambridge University Press:
- 06 March 2024, pp. 1-6
-
- Article
- Export citation
Research agenda for antibiotic stewardship within the Veterans’ Health Administration, 2024–2028
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 02 February 2024, pp. 1-7
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
46 Cognitive Reserve and Gait Speed are Associated with Cognitive Performance in Black/African American Older Adults
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 354-355
-
- Article
-
- You have access
- Export citation
In vitro activity of clindamycin, doxycycline, and trimethoprim/sulfamethoxazole against clinical isolates of β-hemolytic Streptococcus spp. via BD Phoenix and broth microdilution
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 15 December 2023, e238
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Radiofrequency ice dielectric measurements at Summit Station, Greenland
-
- Journal:
- Journal of Glaciology , First View
- Published online by Cambridge University Press:
- 09 October 2023, pp. 1-12
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
-
We recently reported on the radio-frequency attenuation length of cold polar ice at Summit Station, Greenland, based on bi-static radar measurements of radio-frequency bedrock echo strengths taken during the summer of 2021. Those data also allow studies of (a) the relative contributions of coherent (such as discrete internal conducting layers with sub-centimeter transverse scale) vs incoherent (e.g. bulk volumetric) scattering, (b) the magnitude of internal layer reflection coefficients, (c) limits on signal propagation velocity asymmetries (‘birefringence’) and (d) limits on signal dispersion in-ice over a bandwidth of ~100 MHz. We find that (1) attenuation lengths approach 1 km in our band, (2) after averaging 10 000 echo triggers, reflected signals observable over the thermal floor (to depths of ~1500 m) are consistent with being entirely coherent, (3) internal layer reflectivities are ≈–60$\to$
 –70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.
–70 dB, (4) birefringent effects for vertically propagating signals are smaller by an order of magnitude relative to South Pole and (5) within our experimental limits, glacial ice is non-dispersive over the frequency band relevant for neutrino detection experiments.

Integrated efficacy analysis from phase 3 studies of investigational microbiome therapeutic, SER-109, in recurrent Clostridioides difficile infection
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s5
-
- Article
-
- You have access
- Open access
- Export citation
-
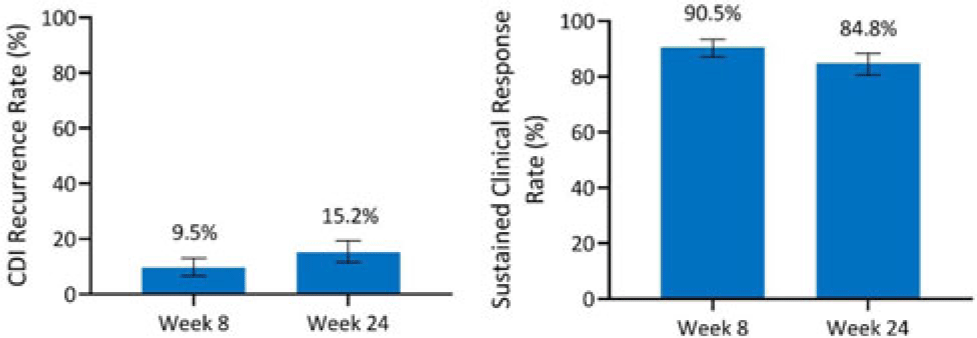
Background: Antibiotics alone are often insufficient to treat recurrent C. difficile infection (rCDI) because they have no activity against C. difficile spores that germinate within a disrupted microbiome. SER-109, an investigational, oral, microbiome therapeutic comprised of purified Firmicutes spores, was designed to reduce rCDI through microbiome repair. We report an integrated efficacy analysis through week 24 for SER-109 from phase 3 studies, ECOSPOR III and ECOSPOR IV. Methods: ECOSPOR III was a randomized, placebo-controlled phase 3 trial conducted at 56 US or Canadian sites that included 182 participants with ≥2 CDI recurrences, confirmed via toxin EIA testing. Participants were stratified by age (<65 years or ≥65 years) and antibiotic regimen (vancomycin, fidaxomicin) and were randomized 1:1 to placebo or SER-109 groups. ECOSPOR IV was an open-label, single-arm study conducted at 72 US or Canadian sites including 263 participants with rCDI enrolled in 2 cohorts: (1) rollover participants from ECOSPOR III who experienced on-study recurrence diagnosed by toxin EIA (n = 29) and (2) participants with ≥1 CDI recurrence (diagnosed by PCR or toxin EIA), inclusive of the current episode (n = 234). In both studies, the investigational product was administered orally as 4 capsules over 3 consecutive days following symptom resolution after standard-of-care antibiotics. The primary efficacy end point was rCDI (recurrent toxin-positive diarrhea requiring treatment) through week 8. Other end points included CDI recurrence rates and safety through 24 weeks. Results: These 349 participants received at least 1 dose of SER-109 in ECOSPOR III or ECOSPOR IV (mean age 64.2; 68.8% female). Overall, 77 participants (22.1%) enrolled with their first CDI recurrence. Four participants received blinded SER-109 in ECOSPOR III followed by a second dose of open-label SER-109 in ECOSPOR IV. Overall, the proportion of participants who received any dose of SER-109 with rCDI at week 8 was 9.5% (33 of 349; 95% CI, 6.6 %–13.0%), and the CDI recurrence rate remained low through 24 weeks (15.2%, 53 of 349; 95% CI, 11.6%–19.4%), corresponding to sustained clinical response rates of 90.5% (95% CI, 87.0%–93.4%) and 84.8% (95% CI, 80.6%–88.4%), respectively (Fig. 1). Most rollover participants (25 of 29, 86.2%) were from the placebo arm; 13.8% had rCDI by week 8. Conclusions: In this integrated analysis, the rates of rCDI were low and durable in participants who received the investigational microbiome therapeutic SER-109, with sustained clinical response rates of 90.5% and 84.8% at weeks 8 and 24, respectively. These data further support the potential benefit of microbiome repair with SER-109 following antibiotics for rCDI to prevent recurrence in high-risk patients.
Financial support: This study was funded by Seres Therapeutics.
Disclosure: None

Integrated safety analysis of phase 3 studies for investigational microbiome therapeutic, SER-109, in recurrent CDI
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s44-s45
-
- Article
-
- You have access
- Open access
- Export citation
Validation of antibiotic stewardship metrics for genitourinary infection management in Veterans Affairs outpatient settings
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s35
-
- Article
-
- You have access
- Open access
- Export citation
-
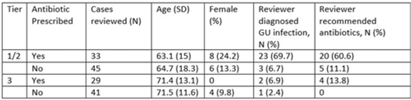
Background: Diagnosis and management of suspected urinary tract infection (UTI) in outpatient settings has been shown to be suboptimal. We previously developed a set of stewardship metrics for UTIs based on electronic health record (EHR) data (Antimicrobial Stewardship & Healthcare Epidemiology 2022;2 suppl 1:S5–S6. doi:10.1017/ash.2022). A tier-based approach was used to more fully capture antibiotic use associated with genitourinary (GU) symptoms and diagnoses. Herein we report a preliminary analysis of validity and reliability of these metrics based on chart abstraction. Methods: The study cohort consisted of patients who visited Veterans Affairs emergency departments or primary care clinics between 2015 and 2022 and who had a GU diagnosis based on International Classification of Disease, Tenth Revision (ICD-10) codes, divided into 3 categories: tier 1 (antibiotics always indicated), tier 2 (antibiotics sometimes indicated), and tier 3 (antibiotics not indicated). Visits related to urological procedures, nontarget settings, or concomitant non-GU infections were excluded. Cases were randomly sampled for manual review from within 8 strata based on tier, use of antibiotics, and visit type. An infectious disease physician and pharmacist abstracted charts using a standardized data-collection instrument. Clinical judgments regarding diagnosis and treatment were recorded on a Likert scale without knowledge of how the patient was managed. The intraclass correlation coefficient (ICC) was used to estimate interrater reliability. Results: To date, 148 cases have been reviewed (50 by both reviewers). Mean (SD) age was 67.5 (15.3) years and 12.2% were female. In a majority of tier 1 and 2 visits in which antibiotics were given, the reviewers found evidence for GU infection (69.7%) and favored prescribing of antibiotics (60.6%) (Table). In contrast, most patients in the tier 3 category who received antibiotics were judged to have noninfectious conditions (eg, benign prostatic hypertrophy) and to not require antibiotics. In the subset of records examined by both reviewers, the interrater reliability of judgments of whether antibiotics were warranted was good (ICC = .704). Conclusions: This preliminary validation provides support for a tier-based approach for stewardship metrics for GU conditions that relies upon electronic data to identify patients for whom antibiotics are generally not indicated.
Disclosures: None

A qualitative evaluation of frontline clinician perspectives toward antibiotic stewardship programs
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 12 / December 2023
- Published online by Cambridge University Press:
- 29 March 2023, pp. 1995-2001
- Print publication:
- December 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Reconstructing Middle Horizon Camelid Diets and Foddering Practices: Microbotanical and Isotope Analyses of Dental Remains from Quilcapampa, Peru
-
- Journal:
- Latin American Antiquity / Volume 34 / Issue 4 / December 2023
- Published online by Cambridge University Press:
- 23 January 2023, pp. 783-803
- Print publication:
- December 2023
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
13 - The Role of Academic Libraries in Developing Social Capital by Promoting Quality Reading in Local Communities
-
-
- Book:
- The Social Future of Academic Libraries
- Published by:
- Facet
- Published online:
- 11 February 2023
- Print publication:
- 22 December 2022, pp 257-272
-
- Chapter
- Export citation
Lack of correlation between standardized antimicrobial administration ratios (SAARs) and healthcare-facility–onset Clostridioides difficile infection rates in Veterans Affairs medical facilities
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 6 / June 2023
- Published online by Cambridge University Press:
- 01 December 2022, pp. 945-947
- Print publication:
- June 2023
-
- Article
- Export citation
Approaches to Monitoring Structural Modification Using In Situ Electron Microscopy
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 144-145
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Interpretability of Low-Dose HRTEM Images of Supported Metal Nanoparticles
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 2152-2154
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Formation of Defects in MoS2 during Data Acquisition of High-resolution Transmission Electron Microscopy
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 2192-2193
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
Large-scale Automated Analysis of High-Resolution Transmission Electron Microscopy Data Assisted by Deep Learning Neural Networks
-
- Journal:
- Microscopy and Microanalysis / Volume 28 / Issue S1 / August 2022
- Published online by Cambridge University Press:
- 22 July 2022, pp. 2984-2986
- Print publication:
- August 2022
-
- Article
-
- You have access
- Export citation
1 - Climate justice, social policy and the transition to net zero in the UK
-
-
- Book:
- Social Policy Review 34
- Published by:
- Bristol University Press
- Published online:
- 13 October 2022
- Print publication:
- 27 June 2022, pp 5-23
-
- Chapter
- Export citation
Regulation of baby food marketing in Thailand: a NetCode analysis
-
- Journal:
- Public Health Nutrition / Volume 25 / Issue 10 / October 2022
- Published online by Cambridge University Press:
- 23 June 2022, pp. 2680-2692
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Characteristics of nursing home residents and healthcare personnel with repeated severe acute respiratory coronavirus virus 2 (SARS-CoV-2) tests positive ≥90 days after initial infection: Four US jurisdictions, July 2020–March 2021
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 5 / May 2023
- Published online by Cambridge University Press:
- 20 May 2022, pp. 809-812
- Print publication:
- May 2023
-
- Article
- Export citation
