



Introduction
The COVID-19 pandemic has had a disproportionate impact on people with dementia and their family carers (Alzheimer's Society, 2020; Liu et al., Reference Liu, Howard, Banerjee, Comas-Herrera, Goddard, Knapp, Livingston, Manthorpe, O'Brien, Paterson, Robinson, Rossor, Rowe, Sharp, Sommerlad, Suárez-González and Burns2021). In 2020, COVID-19 accounted for 73,766 (12.1%) of all deaths registered in England and Wales, with dementia and Alzheimer's disease as the most prevalent pre-existing condition (18,420 deaths) (Office for National Statistics, 2021). Curtailment of normal living has been caused by national lockdowns; in England, there have been three to date, with the last commencing in early January 2021 and concluding in late June 2021 with the ending of legal restrictions on social contact (Institute for Government, 2021). Therefore, although we are yet to reach this point, ‘as COVID-19 moves from pandemic to endemic, new ways of working will need to be developed to protect the dignity and quality of life for people with dementia and their families’ (Burns et al., Reference Burns, Lobo, Olde Rikkert, Robert, Sartorius, Semrau and Stoppe2021: 948).
There is also increasing global evidence, particularly from telephone and online surveys with people with dementia and their family carers, suggesting an adverse effect of the pandemic and associated restrictions on dementia-related symptoms. Cognitive decline and impacts on the mental health of people with dementia have been reported (e.g. Azevedo et al., Reference Azevedo, Calandri, Slachevsky, Graviotto, Vieira, Andrade, Rossetti, Generoso, Carmona, Pinto, Sorbara, Pinto, Guajardo, Olavarria, Thumala, Crivelli, Vivas, Allegri, Barbosa, Serrano, Miranda-Castillo and Caramelli2021; Rainero et al., Reference Rainero, Bruni, Marra, Cagnin, Bonanni, Cupidi, Laganà, Rubino, Vacca, Di Lorenzo, Provero, Isella, Vanacore, Agosta, Appollonio, Caffarra, Bussè, Sambati, Quaranta, Guglielmi, Logroscino, Filippi, Tedeschi and Ferrarese2021), with the mental wellbeing of their family carers also adversely impacted (e.g. Cagnin et al., Reference Cagnin, Di Lorenzo, Marra, Bonanni, Cupidi, Laganà, Rubino, Vacca, Provero, Isella and Vanacore2020; Mazzi et al., Reference Mazzi, Lavarone, Musella, De Luca, de Vita, Branciforte, Coppola, Scarpa, Raimondo, Sorrentino, Lualdi and Postiglione2020; Borg et al., Reference Borg, Rouch, Pongan, Getenet, Bachelet, Herrmann, Bohec, Laurent, Rey and Dorey2021; Budnick et al., Reference Budnick, Hering, Eggert, Teubner, Suhr, Kuhlmey and Gellert2021). This is reiterated in two systematic reviews, with Suárez-González et al. (Reference Suárez-González, Rajagopalan, Livingston and Alladi2021) reporting cognitive decline and the emergence or aggravation of behavioural and psychological symptoms in most studies; the authors suggest that the speed of such decline over three to four months cannot be attributed to dementia progression. Similarly, in their review of neuropsychiatric symptoms in dementia during the pandemic, Simonetti et al. (Reference Simonetti, Pais, Jones, Cipriani, Janiri, Monti, Landi, Bernabei, Liperoti and Sani2020) argue that the most frequently reported symptoms of apathy, anxiety and agitation are likely to have been caused by pandemic restrictions and prolonged social isolation. However, Liu et al. (Reference Liu, Howard, Banerjee, Comas-Herrera, Goddard, Knapp, Livingston, Manthorpe, O'Brien, Paterson, Robinson, Rossor, Rowe, Sharp, Sommerlad, Suárez-González and Burns2021) have argued that such research is mostly predicated on cross-sectional surveys, with very few studies comparing pre-pandemic and pandemic data; therefore longitudinal (quantitative) research is imperative. In addition, such studies were conducted during the early stages of the pandemic where emotional impact and uncertainty may have been at their greatest.
Notably, in the IDEAL cohort study, data collected before and during the pandemic have been contrasted. IDEAL centres on a large cohort study of people living with dementia and carers in Great Britain, focusing on facilitators of and challenges to living well with the condition and how capability to live well might change over time as dementia progresses. Of people living with mild-to-moderate dementia in the community, data from 173 people with dementia and 242 carer-informants collected during the pandemic's second wave was compared with pre-pandemic responses from the IDEAL cohort. In the United Kingdom (UK), the second wave is regarded as beginning in September 2020, peaking in January 2021 and finishing at the end of April 2021 (Office for National Statistics, 2021). Findings include significant negative impacts of the pandemic on loneliness, life satisfaction, and cognition and functioning, although the observed decline in cognition appeared consistent with the normal progression of dementia; there was also minimal impact on wellbeing and mental health (Clare et al., Reference Clare, Martyr, Gamble, Pentecost, Collins, Dawson, Hunt, Parker, Allan, Burns, Hillman, Litherland, Quinn, Matthews and Victor2022).
Although less prevalent, qualitative research has also provided invaluable insights into the experiences of people with dementia who are living through the pandemic. Findings from UK studies have highlighted perceptions of cognitive decline in the person with dementia according to the family care-giver or person with dementia (e.g. Talbot and Briggs, Reference Talbot and Briggs2021; Giebel et al., Reference Giebel, Hanna, Callaghan, Cannon, Butchard, Shenton, Komuravelli, Limbert, Tetlow, Rogers, Eley, Rajagopal, Ward and Gabbay2022). The toll on the mental health of people with dementia and family carers (including that due to loss of services) has also been suggested (Hanna et al., Reference Hanna, Giebel, Tetlow, Ward, Shenton, Cannon, Komuravelli, Gaughan, Eley, Rogers, Rajagopal, Limbert, Callaghan, Whittington, Butchard, Shaw and Gabbay2021; Tuijt et al., Reference Tuijt, Frost, Wilcock, Robinson, Manthorpe, Rait and Walters2021). Interviewing people mostly with young-onset dementia between June and July 2020, Talbot and Briggs (Reference Talbot and Briggs2021: 658) suggest that the pandemic has also exacerbated ‘the shrinking world effect’, with interviewees having lost confidence to re-engage with the world as restrictions were eased. Certainly, and perhaps unsurprisingly, the consequences of social isolation were suggested across these qualitative studies, with Tuijt et al. (Reference Tuijt, Frost, Wilcock, Robinson, Manthorpe, Rait and Walters2021) reporting people with dementia attributing their adverse psychological symptoms to lack of social engagement.
Social connections are often regarded as key to living well and quality of life in people with dementia (Martyr et al., Reference Martyr, Nelis, Quinn, Wu, Lamont, Henderson, Clarke, Hindle, Thom, Jones, Morris, Rusted, Victor and Clare2018; Birt et al., Reference Birt, Griffiths, Charlesworth, Higgs, Orrell, Leung and Poland2020) as well as supporting their sense of self and identity (e.g. Sabat and Harré, Reference Sabat and Harré1992, Reference Sabat and Harré1994; Sabat and Collins, Reference Sabat and Collins1999). Notably, Fazio (Reference Fazio2008) differentiates the ‘self’ as referring to conscious self-reflection and ‘identity’ as a broader term linked to an understanding of our place and perceived roles within society. In the social constructionist account of identity by Sabat and Harré (Reference Sabat and Harré1992), social personae and interactions with others are important for maintaining social identity in dementia. Yet for us all, restrictions due to the pandemic may have limited or prevented our social interactions with others. Certainly, for example, pre-pandemic research has suggested the importance of group identity for people with young-onset dementia (Clare et al., Reference Clare, Rowlands and Quin2008) whose diagnosis may feel ‘out of time’ (Greenwood and Smith, Reference Greenwood and Smith2016). Similarly, the development of collective identities for people with dementia has been linked with self-advocacy (Weetch et al., Reference Weetch, O'Dwyer and Clare2021). Therefore, developing a shared dementia identity may promote psychological wellbeing as well as ‘collective strength’ to effect social change (Clare et al., Reference Clare, Rowlands and Quin2008). During the COVID-19 pandemic, face-to-face peer support was suddenly stopped, with support such as day centres, memory cafes and tailored activities severely limited (Giebel et al., Reference Giebel, Lord, Cooper, Shenton, Cannon, Pulford, Shaw, Gaughan, Tetlow, Butchard, Limbert, Callaghan, Whittington, Rogers, Komuravelli, Rajagopal, Eley, Watkins, Downs, Reilly, Ward, Corcoran, Bennett and Gabbay2021). Therefore, for those who adopt a dementia identity, has the pandemic put this identity under threat? Or have people with dementia navigated ways to maintain their social relationships, including peer support from others?
For a time, the pandemic also impacted on what we could and could not do, i.e. our work and usual pastimes. Therefore, with our usual activities prevented or restricted during lockdowns, were there implications for our sense of self and identity? Certainly, an additional consideration, largely overlooked within frameworks of self and identity in dementia, is occupation. For example, the Components of the Self Model (COSM) in dementia does not discuss occupation explicitly (Bomilcar et al., Reference Bomilcar, Bertrand, Morris and Mograbi2021). However, within occupational science and occupational therapy, identity is regarded as being created and conveyed through occupation (Christiansen, Reference Christiansen1999), with Gallagher et al. (Reference Gallagher, Muldoon and Pettigrew2015: 7) stating that ‘what we do is inextricably linked to who we are’.
Occupations have been defined as ‘the everyday activities that people do as individuals, in families and with communities to occupy time and bring meaning and purpose to life’ (World Federation of Occupational Therapists, 2022). In people with dementia living in the community, engaging in daily activities supports both their identity and sense of agency or control (Phinney et al., Reference Phinney, Chaudhury and O'Connor2007; Chung et al., Reference Chung, Ellis-Hill and Coleman2017). Occupation has also been linked to identity in relation to people with dementia living in long-term residential care, with residents with advanced dementia expressing their identities through both activities and objects which were meaningful to them (Tatzer, Reference Tatzer2019). Moreover, Du Toit et al. (Reference Du Toit, Shen and McGrath2019) have argued that people with dementia living in long-term residential care are at risk of occupational deprivation and injustice, where opportunities for occupation are withdrawn. Certainly, there has been focus on tailored role-identity interventions within such settings, where activities supporting individual self-identity have been connected to overall wellbeing (Cohen-Mansfield et al., Reference Cohen-Mansfield, Parpura-Gill and Golander2006). However, there appears to be little consideration of identity in dementia with regard to the daily activities of occupation for people living in their own home during the pandemic.
Discontinuity in the subjective experience of self is also relevant, and has been assessed in the IDEAL cohort study, pre-pandemic at Time 1 (2014–2016) as well as during the second wave of the COVID-19 pandemic (Clare et al., Reference Clare, Martyr, Morris and Tippett2020b, Reference Clare, Martyr, Gamble, Pentecost, Collins, Dawson, Hunt, Parker, Allan, Burns, Hillman, Litherland, Quinn, Matthews and Victor2022). Discontinuity (as measured on a five-point Likert scale in response to the single item, ‘I feel I am the same person that I have always been’) was reported by 21 per cent of the IDEAL cohort (N = 1,465), with this group reporting significantly poorer psychological health and lower scores on measures of ‘living well’ than the ‘continuity’ group; although effect sizes were small to moderate for both (Clare et al., Reference Clare, Martyr, Morris and Tippett2020b). During the second wave of the COVID-19 pandemic (September 2020 to April 2021), and in addition to the negative impacts reported above, discontinuity in sense of self was significantly more likely in the INCLUDE (Identifying and Mitigating the Individual and Dyadic Impact of COVID-19 and Life Under Physical Distancing on People with Dementia and Carers) sample than in the whole IDEAL cohort at Time 3 (2016–2018): 29.5 per cent versus 20.3 per cent (Clare et al., Reference Clare, Martyr, Gamble, Pentecost, Collins, Dawson, Hunt, Parker, Allan, Burns, Hillman, Litherland, Quinn, Matthews and Victor2022). Such discontinuity could perhaps be attributed to the social restrictions imposed by the lockdown, although disaggregating discontinuity due to the pandemic from ageing and progression of dementia may be problematic. However, when comparing responses from INCLUDE participants with a matched sample of participants who took part in earlier stages of IDEAL data collection but not during the pandemic, there was no difference in the proportions experiencing discontinuity in sense of self (Sabatini et al., Reference Sabatini, Bennett, Martyr, Collins, Gamble, Matthews, Pentecost, Dawson, Hunt, Parker and Allan2022).
Moreover, discontinuity of self is of course different from the social constructionist account of social identity by Sabat and Harré discussed above. A qualitative approach could elucidate the perspectives of people with dementia during the pandemic, including in relation to decline and social identity. As suggested above, most of the pandemic-related studies are dependent on survey data, highlighting the perceived impacts on mental health and possible decline, with perhaps less qualitative research providing further insight into the experiences of people with dementia living through the pandemic. It is also important to gain the accounts of people with dementia in the later phases of the pandemic, as its impacts on wellbeing potentially continue or change.
Therefore, the key aims of the study presented here were to explore the perspectives of people with dementia on living through the COVID-19 pandemic (within the context of the ‘post-vaccine’ period and the national lockdowns in England and Wales); and to determine perceived challenges to and facilitators of ‘living well’ during the COVID-19 pandemic and beyond as restrictions were eased. Here, the ‘post-vaccine’ time period refers to that from December 2020 onwards when the vaccination programme within the UK had commenced (for further discussion, see the Methodological Approach section). In addition, the study findings are considered in relation to understandings of identity in dementia which the broader accounts of living through the pandemic have highlighted.
Methodological approach
Study design and ethics
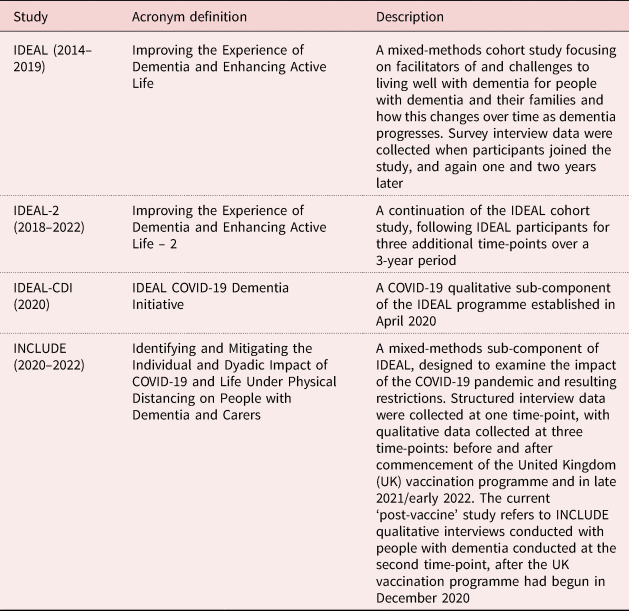
INCLUDE is a pandemic-specific mixed-methods component of the IDEAL cohort study. The IDEAL study has been running since 2014, with its second phase, IDEAL-2, commencing in 2018 (see Table 1). The INCLUDE ‘post-vaccine’ qualitative interview study presented here employed a subtle realist ontological approach, where phenomena are seen to exist but are subject to multiple, socially constructed interpretations (Hammersley, Reference Hammersley1992; Blaikie, Reference Blaikie2007). Throughout the research process, we maintained a sensibility to this approach; from the aims through to the choice of data collection, and with particular cognisance that the analyses and findings presented are our representation of the experiences of people with dementia, living through the COVID-19 pandemic.
Table 1. IDEAL, IDEAL-2 and INCLUDE cohort studies
IDEAL was approved by Wales Research Ethics Committee 5 and IDEAL-2 by Wales Research Ethics Committee 5 and Scotland A Research Ethics Committee. INCLUDE was approved as an amendment to IDEAL-2 for England and Wales. IDEAL and IDEAL-2 are registered with the UK Clinical Research Network.
Sampling and recruitment
A convenience sample of potential participants with mild-to-moderate dementia living in the community, drawn from INCLUDE survey interview respondents who could provide informed consent to take part in a qualitative interview, was initially approached either by telephone or email. Trained researchers had assessed participants' capacity to consent based on criteria set out in the Mental Capacity Act 2005 (HM Government, 2005) and the Mental Capacity Act Code of Practice (Department for Constitutional Affairs, 2005). No potential participants lived in residential care. Ten potential participants were contacted, and eight were recruited to the study. However, having been re-diagnosed with a different neurological condition, one person had her data excluded, resulting in seven participants.
Recruited participants had already provided written, informed consent to take part in the INCLUDE project (Clare et al., Reference Clare, Martyr, Gamble, Pentecost, Collins, Dawson, Hunt, Parker, Allan, Burns, Hillman, Litherland, Quinn, Matthews and Victor2022), therefore process consent only was required; as consent is an ongoing process (Dewing, Reference Dewing2008), it was requested before, during and after the qualitative interviews. However, potential participants were fully briefed about what the INCLUDE ‘post-vaccine’ qualitative interview would involve and had been given time to consider whether they wanted to take part or not.
Semi-structured interviews
Semi-structured interviews were conducted based on a flexible topic guide, drawing on the pandemic timeline but focusing on the current lockdown and in relation to daily routines, coping and help/support. Interview questions included the following: ‘How are you affected in the current situation now? – What are you doing differently now? Is anyone helping you?’; also ‘What support do you need or want now and going forward? What information do you need going forward?’ (for the full semi-structured interview schedule, see the online supplementary material, Interview Guide). All interviews were conducted remotely, five of the interviews via telephone and two via Zoom, in accordance with interviewee preference. Interviews ranged between 32 minutes and 1 hour 19 minutes. All interviews were recorded and professionally transcribed verbatim.
Interviews were carried out following the start of the COVID-19 vaccine rollout in England and Wales. Two of the interviews were conducted by CP during the first month of Lockdown 3 in England (January 2021), with the remainder completed by SSt on joining the study team (April to May 2021). All interviews took place during the third national lockdown in England and Wales. Notably, the research team had anticipated that the ‘post-vaccine’ time period (i.e. commencing from the start of the vaccine rollout onwards) would be significant in interviewees' accounts, e.g. hope that the vaccine meant the pandemic was coming to an end. However, interview accounts suggested more the ongoing impacts of COVID-19 restrictions. In addition, both interviewers were cognisant of the different lockdown stages and associated restrictions at the time of each interview, probing responses accordingly, but accounts were not greatly nuanced in this way.
Qualitative analysis
The interviews were analysed using framework analysis which is a five-stage generic data management tool for thematic analysis of qualitative data: familiarisation, identifying a thematic framework, indexing, charting, and mapping and interpretation (Ritchie and Spencer, Reference Ritchie, Spencer, Bryman and Burgess1994; Spencer et al., Reference Spencer, Ritchie and Ormston2014). Familiarisation with the data was conducted by reading and re-reading the transcripts and interview notes. SSt devised detailed transcript summaries and notes to aid the analytic decision-making process and development of an inductively derived initial thematic framework for all themes.
In terms of methodological rigour, CP reviewed this framework, providing additional notes and discussion after comparing it against two of the interviews. This was in addition to regular discussion of the ongoing analysis between SSt, CP and RC. The entire dataset was indexed using the most current version of NVivo (2020; QSR International, Melbourne), and charting applied but by retaining verbatim quotations in order to develop themes rooted in participants' interview accounts. Lastly, mapping and interpretation were applied to finalise themes, with further revision through discussion between SSt and CP.
Findings
The seven interviewees ranged in age from 53 to 83; five were female and three lived alone (see Table 2). Two had Alzheimer's disease, two had vascular dementia, two had a mixed dementia type and one had fronto-temporal dementia. Three of these interviewees had young-onset dementia (one with Alzheimer's disease, one with mixed dementia and one with fronto-temporal dementia). ‘Years since diagnosis’ was researcher-rated as part of the IDEAL cohort study from which interviewees were drawn for INCLUDE; four of the seven interviewees had been recorded as ‘between six and nine years’ since diagnosis. All but one of the interviewees were living in England at the time of interview, with only one interviewee living in Wales under somewhat different COVID-19 restrictions (see Table 3). When asked during interview, three reported ‘shielding’, i.e. being advised by the government to stay at home because they were clinically vulnerable due to other health conditions.
Table 2. Participant socio-demographic and clinical characteristics, and COVID-19 restrictions in place at the time of interview

Notes: 1. 18–25 = mild cognitive impairment; 10–17 = moderate cognitive impairment; less than 10 = severe cognitive impairment (MoCA Test, 2021). 2. Young-onset dementia refers to a diagnosis made before the age of 65 (Dementia UK, 2021). 3. This interviewee also referred to Lewy body dementia during the interview.
Table 3. Lockdown stage at which participant was interviewed and corresponding COVID-19 restrictions in place in England and Wales at that time

Three key themes were derived from the analysis (see Table 4). Theme 1, Coping with the psychological impact of the COVID-19 pandemic, relates to individuals' variable coping with the pandemic and its concomitant restrictions, with a sense of vulnerability related to individuals' perceived or feared decline in their dementia as much as to COVID-19 itself. Theme 2, Connected lives, focuses on the importance of individuals maintaining connections for their psychosocial wellbeing, within their social relationships, peer groups and communities but particularly for their sense of a connected identity in continued or alternative routines/activities during the pandemic. Theme 3, Pro-active service support and accessing health and social care: communication, agency and choice, captures diverse experiences of health and social care support during the pandemic, with pro-active support largely absent, and with a need to facilitate individuals' communication preferences as well as respecting individual choice as to their ‘dementia identity’. Therefore, this last theme resonates with issues people experienced prior to COVID-19 (e.g. lack of service support; adopting a ‘dementia identity’) but which the pandemic has further highlighted (for Themes and Subthemes with Definitions and Exemplar Quotations, see the online supplementary material).
Table 4. Themes, subthemes and definitions

Theme 1. Coping with the psychological impact of the COVID-19 pandemic
Coping with the pandemic: vulnerability, acceptance and adaptation
Even though interviews took place after the start of the vaccine rollout, the vaccine was largely discussed as something which had ‘got to be done’ (P3), with only a few suggesting it was ‘hope that we're turning a corner’ (P6). Most interviewees, particularly those not ‘shielding’, discussed coping reasonably well with the pandemic, with stoic acceptance of and adaptation to the rules and restrictions: ‘I suppose I'm a bit chameleon-like. You just adapt to it, don't you?’ (P7). One interviewee repeated the need to ‘take it one day at a time’ (P3), with another likening her resilience to living through the Second World War: ‘oh, it's an old war veteran, that's what it is’ (P1).
One interviewee (P4) who had become ‘a bit of a recluse’ before the pandemic, attributing his lack of self-motivation to low dopamine and his Lewy body dementia, felt the pandemic had actually come at a good time so he did not have to make excuses for not going out. For him also, staying positive was a choice:
And you've got the choice of letting it spoil your life or you can live your life to the full still. But, as I say, I just live day by day. (P4)
Talk of COVID-19 risk was not pervasive in interviewees' accounts but understandably was more evident in those of people who had been ‘shielding’. For one interviewee who was ‘shielding’ due to having had pleurisy, having to go into town shopping had been daunting ‘because it was, like, everybody's touched everything’, preferring instead to stay at home: ‘I felt safe because I've been in my little cocoon, in my little home’ (P2). Another interviewee had chosen to ‘shield’ before government advice to do so, and, early into the third national lockdown in England, his sense of confinement was clear:
To be honest with you, I'd think I'd … you know, not being flippant, but I think I'd have been better off in a prison than being under these situations because it's so … so difficult to keep coping with now. (P5)
Certainly, the ongoing impact of the pandemic restrictions was more significant in interviewees' accounts than the potential hope of the new vaccine because their daily lives remained affected. Although some people had adapted to the continuing rules and restrictions, others who had been ‘shielding’ still felt vulnerable.
Fear of decline: losing time?
However, where interviewees expressed vulnerability, this was not so much in terms of COVID-19 risk as due to feared or perceived decline during the pandemic. Although those who discussed this did not attribute their decline to the pandemic specifically, these interviewees seemed mindful of losing time and not being able to see family or engage in regular activities.
Some interviewees were very aware they were living with a neurodegenerative condition: ‘we don't know what we'll have forgotten. A year's a long time in the world of dementia’ (P6). For this interviewee, a year of lockdowns and fear of decline was also linked to losing her independence. For another interviewee, the loss of a year of seeing family and ‘making memories’ was resented:
And I feel like I've lost … wasted a year of my life. Because I've got dementia as you obviously know but I want to make the most of my life. So I don't want to sit indoors and do nothing. I want to do everything I possibly can while I can … And I feel like … I feel a bit cheated that I've been missed … I've lost a year. (P2)
Therefore, both fear of decline and the sense of missed time were key concerns for such interviewees, whereby skills and experiences may have been lost to the pandemic, perhaps never to be regained or lived.
‘The start of the end’: reconnecting with a ‘post-COVID’ world
Linked to ‘fear of decline’, some interviewees seemed to have lost self-confidence and felt worried as to which skills they might have forgotten, although most interviewees seemed keen to reconnect with the world (e.g. seeing family or going on holiday). As restrictions were eased, the interviewee with Lewy body dementia wanted to push himself to go out more but by staying local where he was known (P4). Similarly, another interviewee discussed a planned holiday to an area and a guesthouse she had visited many times previously so where she was known and felt safe. For this interviewee also, her hyperacusis (noise sensitivity) meant she had enjoyed the ‘quiet bubble’ of lockdown, therefore the ‘post-COVID’ world was somewhat daunting for her:
It's whether I want to come out of … to back to the world again … I've enjoyed this … this quiet world … And I'm not sure whether I want to join the noisy world again. (P6)
Therefore, although a few interviewees seemed apprehensive about getting out into the world because of endemic COVID-19, ‘it's still going to be around. I mean, the virus isn't going to go’ (P5), reticence for most was due to lack of self-confidence to renegotiate the world.
Theme 2. Connected lives
Purpose and personhood: maintaining activities
A dominant subtheme was the importance of activities and routines to maintain a sense of purpose and agency. Interviewees discussed trying to keep busy by establishing routines (e.g. walking every day, going for a run, gardening), although this had been easier during the warmer weather of the first lockdown rather than the repetitious ‘Groundhog Day’ (P7) of the second one during the winter months: December, January and February. The absence of valued activities due to the pandemic had been problematic, e.g. for the interviewee who had only got to go to her dementia choir once (P2) or the interviewees who had valued travelling to keep their minds active: ‘I'm doing it to keep my brain working’ (P5) and ‘the travelling, I called my Sudoku’ (P6). The latter interviewee, who had travelled independently and regularly before the pandemic, also said she had become depressed at the start when this travel had suddenly stopped: ‘I didn't know where I fitted in anymore’ (P6).
Therefore, this quotation suggests perhaps that the loss of valued activities had meant a disconnection from activities which were central to individuals' sense of identity. For one interviewee (P3), whom the pandemic had kept from her valued volunteering role, this seemed linked to her past job roles and family responsibilities (‘I've always been a carer’: P3); a phrase and identity she repeated and reiterated throughout the interview:
Yeah, I don't want to lose that part of me. I can't change after having the fit and the problem I've got. You know, if I see somebody struggling, I … I … I want to help. (P3)
The interviewee who had lamented being unable to travel managed to replace this with a different activity, photography (P6). Another interviewee who saw herself as creative (‘I've always made things’: P7) surprised herself during lockdown when she was still able to do dressmaking; although, having got physically fit prior to the pandemic, this interviewee's most valued activity was being able to continue her exercise regime during the lockdowns (country walks and going running). Certainly, a very few interviewees were able to continue valued activities (e.g. attending church groups online), with one interviewee continuing his volunteering, helping others by telephone and with dementia research (e.g. online talks to university students):
So it's good to be able to do something that keeps you occupied … And feel that you're part of the world. (P4)
Therefore, continuing with (or finding alternative) valued activities during the pandemic seemed to help interviewees' continued sense of self or a connected identity, wherein they were able to assert their agency; conversely, when valued activities were disrupted, interviewees' identity was disrupted also.
Social and emotional connections: friends, family and peer support
Loss of certain activities was also related to interviewees' social connections, with those who had attended dementia groups (or dementia choirs) missing the peer support, shared understanding and friendships these had provided. One interviewee missed ‘proper conversations’ over a coffee (P7) whereas another felt only others from her young-onset dementia group could really understand her struggle with memory: ‘it's like a totally different “I can't remember” … I know, I know it … I know, I know the information’ (P2).
Certainly, although most interviewees were using online communication (with some of one interviewee's dementia group members learning to do so during the pandemic), social and emotional connections were still profoundly missed. Missing family and friends due to the pandemic restrictions had been understandably difficult. One interviewee illustrated the distance created between himself and friends living close by: ‘well, I used to go and see my friends … who live a couple of hundred yards away and all that. But you can't do that’ (P5).
Some interviewees had been able to meet family outdoors (in a socially distanced manner) as restrictions were eased but a few had not seen family members who were frontline keyworkers, and hence at higher risk of developing COVID-19, for some time: ‘we Skype but it's not the same … I want hugs’ (P2). One interviewee also emphasised the importance of human contact in her ecclesiastical voluntary role: ‘men seem to benefit so much more by it, if someone can just sit there and hold their hand’ (P1). Similarly, another interviewee (who lived alone) reiterated the importance of emotional connections for people with dementia, although the three interviewees living alone did not imply they felt isolated or lonely:
…that emotion you feel from a visit far outstrips any good news that might have been imparted because you won't remember that. But it's just the emotional feeling that you … you do … you are left with. (P6)
Therefore, unsurprisingly, the absence of peer support from dementia groups as well as not seeing family and friends in person had been felt keenly by interviewees, with human contact and social connections even more important for people with dementia.
Connected communities were also apparent in some interviewees' accounts, relating to their local communities looking out for them, once their dementia was known (e.g. support getting shopping). There was also simply the sense of feeling more connected to others through the pandemic (‘people have been more friendly’: P2), particularly where interviewees lived in village communities: ‘but there's a lot of goodness in the world, and this virus has fetched a lot of it out’ (P4). Therefore, such accounts seem to reflect the community spirit triggered by the pandemic (e.g. receiving practical support) as well as simply a connection to others through the shared experience of living with pandemic restrictions.
Connecting with nature and the outdoors was also important. Going on daily walks or getting out and connecting with nature was imperative for interviewees' physical but particularly mental health. One interviewee appreciated the ‘lovely ridge walks’ she was able to go on to exercise in a nearby national park (P7) whereas another loved simply sitting in a car with her husband and watching the waves:
We go down to the sea and just watch the waves, as a lot of people do round here … It … It gets quite crowded … You almost have to book your place … But it's lovely … Because it's so soothing, watching the … watching the waves. (P1)
Certainly, getting out and connecting with nature was perhaps no longer taken for granted: ‘I'm very lucky. I've got a garden and the weather was beautiful’ (P2). Getting outdoors in whatever ways possible was imperative for managing day-to-day life under COVID-19 restrictions.
Theme 3. Pro-active service support and accessing health and social care: communication, agency and choice
Being forgotten: accessing practical support during the pandemic
This subtheme was discussed in relation to being left off supermarket ‘priority’ lists for home deliveries of food at the start of the pandemic, with some waiting several weeks to get a delivery slot: ‘dementia were missed off at the beginning, badly. They just forgot about us’ (P6). One interviewee (P5) also referred to being on a low income but having to meet the cost of increased energy bills during the winter lockdown and the cold season (December, January and February).
Pro-active service support and ‘signposting’
Perhaps in relation to ‘being forgotten’, when interviewees were asked, there was a notable absence in their accounts of pro-active health or social care support during the pandemic (e.g. from a memory clinic), with ‘checking in’ on interviewees largely being provided by charities (e.g. Alzheimer's Society). One interviewee attributed this lack of contact about his dementia (and other health conditions) to ageism, equating this to people dying in care homesFootnote 1 during the pandemic:
…it feels as if, you know that's it. You've had your time, you're 70 odd years old. Time for you to go. Make way! (P5)
Similarly, although another interviewee felt ‘lucky’ to have had some ‘checking in’ from his general practitioner (GP) practice, he was concerned that others (with health conditions including dementia) had been less fortunate: ‘people had said throughout all of this, they've felt as if they've just been … get on with it. Let go’ (P4). As was the case for other participants, this interviewee wanted to know when services or support would be restarting. He also reiterated the importance of ‘signposting’ to different services (and benefits), particularly following the ‘shock’ of diagnosis, after which he felt it was left to individuals to find out what support is available. Certainly, there was the sense from other interviewees' accounts that lack of ‘checking in’ and appropriate ‘signposting’ was not necessarily pandemic-specific but may have signified differential service support from the point of diagnosis onwards.
Accessing health and social care services: communication and choice
In terms of interviewees requesting access to health and social care services during the pandemic, experiences varied, perhaps inevitably due to interviewees' different health conditions (and localities). Of those who did, some had no difficulty getting nurse or doctor's appointments during the first lockdowns (P1, P4, P7) but another reported it took three months for him to get an appointment to confirm what he had suspected was diabetes (P5).
However, a common thread across all accounts was the need for health and social care services to provide choice and to adapt to individual communication preferences. One interviewee had been happy to have a telephone annual review with her GP (P7) but not all interviewees were happy using the telephone. GP or hospital telephone appointments only rather than video calls had been offered to the interviewee with hyperacusis (noise sensitivity), meaning her daughter (who lived in a different household) had had to talk to health-care professionals for her; consequently they had ‘got the wrong end of the stick’, with the interviewee feeling she had ‘lost all that independence with [her] health’ (P6). Therefore her message for health-care professionals was as follows:
Listen to our … offer us choice. Don't assume we can fit in with what you see as the best choice. Because I certainly couldn't fit in with the phone. (P6)
Therefore, different experiences of accessing health and social care services were apparent, with the importance of offering people with dementia choice in accessing such services also highlighted to support their agency.
Throughout these interviews, it was also apparent that adopting a ‘dementia identity’ varied, which is of importance when considering how people with dementia can best be supported. Although no interview accounts suggested individuals wanted to hide their dementia and several had attended dementia support groups, three interviewees who lived alone and independently were happy for it to be known (P4, P6, P7), also advocating for themselves (and others) with the condition as active participants in dementia groups and research.
Discussion
This study is one of the few to have explored the experiences of people with dementia later into the pandemic, after commencement of the vaccine programme. The psychological impact of the pandemic varied, with interviewees' accounts mostly suggesting a degree of stoicism in the face of the pandemic and social restrictions, with those who were ‘shielding’ perhaps struggling more. However, as well as reticence to re-engage with the world, losing time in relation to fear of decline was apparent, with the temporality of their condition heightened for people with dementia during the pandemic. Perhaps unique to this study with people with dementia, maintaining or adapting routines and activities during the restrictions was important for interviewees' sense of identity as well as to maintain a sense of purpose. Similarly, social connections were imperative which included the impact of absent dementia groups which would normally offer shared understanding and shared identity, particularly for interviewees with young-onset dementia. Other concerns, such as lack of pro-active service support, were not specific to the pandemic but have been highlighted further during this time.
Interviewees' largely stoic acceptance of social restrictions in our study with people with dementia is reflective of research with older people in general, although our sample also included some younger interviewees. Fewer impacts on the mental health of older people than younger age groups have been reported (Holingue et al., Reference Holingue, Badillo-Goicoechea, Riehm, Veldhuis, Thrul, Johnson, Fallin, Kreuter, Stuart and Kalb2020; Van Tilburg et al., Reference Van Tilburg, Steinmetz, Stolte, Van der Roest and de Vries2021), with older people in the UK discussing resilience in the face of COVID-19 restrictions (McKinlay et al., Reference McKinlay, Fancourt and Burton2021). However, different of course is our interviewees' discussion of fear of decline, where a plethora of evidence suggests the impact of the pandemic on cognitive decline in dementia (Suárez-González et al., Reference Suárez-González, Rajagopalan, Livingston and Alladi2021). This finding is also consistent with those from earlier in the pandemic (O'Rourke et al., Reference O'Rourke, Pentecost, Van den Heuvel, Victor, Quinn, Hillman, Litherland and Clare2021) where participants feared the impact of not taking part in their usual activities as well as getting out into the world again. Talbot and Briggs (Reference Talbot and Briggs2021) have reported similar findings in terms of people with dementia losing confidence as social restrictions continued, with apprehension about re-entering the world after the safety of lockdown; the ‘shrinking world effect’ amplified by the pandemic. The additional aspect in our study of losing time due to the pandemic, in relation to fear of decline, has not been suggested in previous pandemic-related qualitative studies as far as we are aware. However, lived time has been discussed as critical to the experience of people with dementia (Eriksen et al., Reference Eriksen, Bartlett, Grov, Ibsen, Telenius and Rokstad2020), including regarding their future outlook and ways of coping (Heaton et al., Reference Heaton, Martyr, Nelis, Marková, Morris, Roth, Woods and Clare2021).
Therefore, with such impacts potentially affecting the self-confidence of people with dementia in the longer term as well as the continued uncertainty as to the pandemic's duration, people with dementia may need continued support from family care-givers and service providers to regain self-confidence in their abilities as well as being re-engaged with their previous activities. Certainly, needing pro-active, post-diagnostic service support and ‘signposting’ was evident in INCLUDE interviewees' accounts during the pandemic, with this absence also suggested as preceding the pandemic but amplified by it. The pandemic has created additional challenges in supporting people with dementia and their family care-givers, wherein demand for rehabilitation, particularly for older people in general, may have increased (De Biase et al., Reference De Biase, Cook, Skelton, Witham and and Ten Hove2020). Nonetheless, it remains important to consider the role services can play in supporting people with dementia to regain their self-confidence and past activities and therein more of their lives.
The importance of such support becomes more apparent in considering other key findings from the study in relation to identity, namely maintaining a sense of purpose through previous or new activities, maintaining social and emotional connections, and also the shared dementia identity adopted by some interviewees. The sociological literature on identity has commonly considered chronic conditions as triggering a loss of self (Charmaz, Reference Charmaz1983) or biographical disruption (Bury, Reference Bury1982) wherein identity is under threat from the social consequences of the illness, with individuals striving to manage or adapt to this threat (Charmaz, Reference Charmaz, Albrecht, Fitzpatrick and Scrimshaw2000). This includes people with dementia (Clare, Reference Clare2003; Beard, Reference Beard2004; Beard and Fox, Reference Beard and Fox2008), where ‘identity construction is a deliberate, if shifting accomplishment’ (Beard, Reference Beard2004: 417), thus signifying identity reconstruction as a key aspect of agency in dementia. However, in our study, the source of disruption was not dementia itself but pandemic-related social restrictions superimposed on dementia.
The social constructionist account of dementia by Sabat and colleagues includes focus on the ‘self’ of social personae, whereby a sense of social identity is dependent on our interactions with others (Sabat and Harré, Reference Sabat and Harré1992, Reference Sabat and Harré1994; Sabat, Reference Sabat2021). Therefore, when such relationships are limited or prevented (here, due to the pandemic) our social identity is also under threat. This is in addition to social connections as a basic psychological need which have been linked to social health in dementia (Vernooij-Dassen and Jeon, Reference Vernooij-Dassen and Jeon2016; Dröes et al., Reference Dröes, Chattat, Diaz, Gove, Graff, Murphy, Verbeek, Vernooij-Dassen, Clare, Johannessen, Roes, Verhey and Charras2017) and are one aspect of social capital (Ferlander, Reference Ferlander2007) which the pandemic had adversely affected. Interviewees hoped to reconnect more with family and friends as restrictions eased; however, it is possible that not all people with dementia may have the social support networks they feel they need. Prior to the pandemic, approximately 30.1 per cent of IDEAL participants with dementia reported feeling moderately lonely and 5.2 per cent severely lonely (Victor et al., Reference Victor, Rippon, Nelis, Martyr, Litherland, Pickett, Hart, Henley, Matthews, Clare and IDEAL programme team2020), with increased loneliness reported during the pandemic's second wave (Clare et al., Reference Clare, Martyr, Gamble, Pentecost, Collins, Dawson, Hunt, Parker, Allan, Burns, Hillman, Litherland, Quinn, Matthews and Victor2022). IDEAL participants living alone were lonelier than those living with others but reported no differences in wellbeing (Clare et al., Reference Clare, Martyr, Henderson, Gamble, Matthews, Quinn, Nelis, Rusted, Thom, Knapp, Hart and Victor2020a). In the current study, there were no discernible differences between the interview accounts of those living alone or living with others, with one interviewee reiterating that she had chosen to live alone. Nonetheless, services may need to consider how best to support the social connections of people with dementia. Social prescribing could be one potential avenue and has been advocated as a key principle of personalised care (NHS England, 2022), although evidence for it is limited including in dementia care (Baker and Irving, Reference Baker and Irving2016).
As well as missing family and friends, INCLUDE interviewees also missed the peer support and shared experiences provided by their dementia support groups; in particular, those with young-onset dementia missed the shared understanding and peer support offered by others with the same diagnosis. Again this links with the work of Sabat and colleagues regarding the social self as well as resonating with previous work on shared group identity for people with young onset dementia such as the ‘collective strength’ gained from such group memberships (Clare et al., Reference Clare, Rowlands and Quin2008), and the impetus to challenge public perceptions and stigma about the condition (Hagan and Campbell, Reference Hagan and Campbell2021). Moreover, the three INCLUDE interviewees with young onset dementia engaged with advocacy work and were comfortable with adopting a public ‘dementia identity’, in spite of the risk of stigma, therein also suggesting the shift from a ‘deficit narrative’ towards active citizenship and driving social change (Birt et al., Reference Birt, Poland, Csipke and Charlesworth2017). Addressing stigmatising public perceptions and facilitating dementia awareness within the community is important. For example, the drive for dementia-friendly communities has been one such initiative (Buckner et al., Reference Buckner, Darlington, Woodward, Buswell, Mathie, Arthur, Lafortune, Killett, Mayrhofer, Thurman and Goodman2019), whereby the importance of raising societal awareness and understanding has been identified (Quinn et al., Reference Quinn, Hart, Henderson, Litherland, Pickett and Clare2021). However, as in our study, it is important to note that not all people with mild-to-moderate dementia may want to adopt a dementia identity and self-advocate, perhaps making them less likely to engage with peer support groups.
However, for all our interviewees, maintaining previous or new activities was central not only to keeping a sense of purpose during the pandemic but also for facilitating identity, e.g. the former ‘carer’ prevented from her volunteering role and looking after others or the self-reinvention by those revisiting past or taking up new hobbies. Within occupational therapy, occupation or carrying out day-to-day meaningful activities is regarded as imperative for wellbeing (World Federation of Occupational Therapists, 2022), and in dementia as supporting identity and agency (Phinney et al., Reference Phinney, Chaudhury and O'Connor2007; Chung et al., Reference Chung, Ellis-Hill and Coleman2017). Therefore, individuals' impetus to maintain such activities may also be a form of coping related to self-maintaining and self-adjusting responses, whereby the threat to self is managed (Clare, Reference Clare2003). ‘Meaningful activity’ has been linked to both expressing and maintaining identity (Han et al., Reference Han, Radel, McDowd and Sabata2016; Tierney and Beattie, Reference Tierney and Beattie2020), with Strick et al. (Reference Strick, Abbott, Thompson Coon and Garside2021) linking ‘meaningful occupation’ in dementia to past as well as evolving identity. However, much previous research has focused on loss of or persistence of the self, particularly in relation to autobiographical memory rather than on adaptation and change (Caddell and Clare, Reference Caddell and Clare2010), when shifts in identity may be important to ‘live well’ with dementia (Wolverson et al., Reference Wolverson, Clarke and Moniz-Cook2016). Regarding the COSM and ‘the emergent self’ in dementia (Bomilcar et al., Reference Bomilcar, Bertrand, Morris and Mograbi2021), where unified experiences are seen to be important, how current roles and activities merge with past ones may be one way identity is retained. Reconfiguring occupation within theoretical understandings of identity in dementia may be of use to drive future research.
This paper has outlined the broader experiences of INCLUDE interviewees during the ‘post-vaccine’ period of the COVID-19 pandemic as well as suggesting certain insights into identity from the study's findings. However, the study was not without its limitations, of course. Firstly, it is acknowledged that, if the project had been devised with identity as the focus, the topic guide and conduct of the interviews would have been framed accordingly, and therefore interviewees' perspectives on identity specifically would have been sought. This may have provided negating or conversely supporting data as to the insights offered in this paper. This may be particularly so perhaps in relation to the experiences of the four participants with young-onset dementia for whom identity concerns may have been different from those of older interviewees (Caddell and Clare, Reference Caddell and Clare2011; Greenwood and Smith, Reference Greenwood and Smith2016), if this aspect had been probed further during the interviews. Nonetheless, identity was identified as prominent and therefore included to ensure comprehensiveness and sufficiency of the thematic analysis (Richards, Reference Richards2005). A similar argument can be made in relation to gender as most (five of the seven) participants interviewed were female. Certainly, the convenience sampling strategy employed within the study, although not ideal within qualitative research (Patton, Reference Patton2015, was expedient within the context of the INCLUDE ‘rapid response’ work to the COVID-19 pandemic. However, within the recruited sample, there was a mix of participants with regard to criteria, including living alone or with a partner and with different types and durations of dementia.
In addition, the limited socio-demographic characteristics of the sample are acknowledged in that all interviewees were White British; although the INCLUDE cohort from which this sample was drawn was predominantly White British at 94.8 per cent which also reflects that there are fewer older BAME (Black, Asian and Minority Ethnic) people diagnosed with dementia in the population (Clare et al., Reference Clare, Martyr, Gamble, Pentecost, Collins, Dawson, Hunt, Parker, Allan, Burns, Hillman, Litherland, Quinn, Matthews and Victor2022). However, in recognition of the need to understand the experiences of people from diverse BAME communities living with dementia in the UK and those of their family care-givers, additional work is being undertaken (Silarova et al., Reference Silarova, Nelis, Ashworth, Ballard, Bieńkiewicz, Henderson, Hillman, Hindle, Hughes, Lamont, Litherland, Jones, Jones, Knapp, Kotting, Martyr, Matthews, Morris, Quinn, Regan, Rusted, van den Heuvel, Victor, Wu and Clare2018). Participants also all had mild-to-moderate dementia and were able to take part in an interview, therein also reflecting a dependence on verbal methods in qualitative dementia research (Phillipson and Hammond, Reference Phillipson and Hammond2018). Potential research focus on occupation and non-verbal expressions of agency in people with more advanced dementia necessarily demands alternative approaches (Collins et al., Reference Collins, Hunt, Quinn, Martyr, Pentecost and Clare2022). It can also be argued that, even without identity preconfigured as the theoretical framework in the qualitative research design, identity issues were still evident and perhaps brought to the fore because of the context of the COVID-19 pandemic.
Conclusion
This study has sought to elucidate the ongoing impacts of the COVID-19 pandemic on people with dementia after commencement of the vaccine programme in the UK, therein adding to the accounts of people with dementia during the pandemic but from within this later time-frame. Unlike earlier studies, our findings have highlighted that people with dementia were cognisant of the temporality of their condition, having lost time due to the pandemic, and experienced fear of decline due to social restrictions and lost confidence to re-engage with the world. In addition, our findings suggest the agency with which interviewees strove to cope with threats to social identity through maintaining social and emotional connections, with some also adopting a shared dementia identity. Occupation and maintaining previous or new activities for keeping a sense of purpose as well as facilitating identity has not been reported in previous qualitative studies with people with dementia during the COVID-19 pandemic. Therefore, as well as being an important consideration for supporting people with dementia as the pandemic eases, future research into occupation and identity for people with dementia is perhaps of potential value.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S0144686X22001350.
Data
INCLUDE data were deposited with the UK Data Archive in June 2022 and will be available to access from July 2023. Details of how the data can be accessed after that date can be found at https://reshare.ukdataservice.ac.uk/855800/.
Acknowledgements
We acknowledge the support of NIHR Dementias and Neurodegeneration Specialty (DeNDRoN), and Health and Care Research Wales with IDEAL cohort recruitment and data collection. We gratefully acknowledge the local principal investigators and researchers involved in participant recruitment and assessment within these networks. We are grateful to the IDEAL study participants for their participation in the IDEAL and INCLUDE studies, to the wider group of IDEAL programme researchers, and to members of the ALWAYs group and the Project Advisory Group for their support. The support of the Economic and Social Research Council is gratefully acknowledged.
Author contributions
SSt conducted interviews, carried out the analysis, devised and wrote the draft paper. CP contributed to the study's concept and design, conducted interviews, took part in ongoing discussions about and agreed the final analysis, provided edits and comments on drafts, and agreed the final version to be published. RC contributed to the study's concept and design, took part in ongoing discussions about and agreed the final analysis, provided edits and comments on drafts, and agreed the final version to be published. CQ contributed to the study's concept and design, provided edits and comments on drafts, and agreed the final version to be published. ED identified potential participants, provided edits and comments on drafts, and agreed the final version to be published. RM provided edits and comments on drafts, and agreed the final version to be published. SSa accessed participant socio-demographic and clinical characteristics, provided edits and comments on drafts, and agreed the final version to be published. JT provided edits and comments on drafts and agreed the final version to be published. LC devised the study, provided edits and comments on drafts, and agreed the final version to be published.
Financial support
‘Identifying and Mitigating the Individual and Dyadic Impact of COVID-19 and Life Under Physical Distancing on People with Dementia and Carers (INCLUDE)’ was funded by the Economic and Social Research Council (ESRC; grant number ES/V004964/1; Investigators: Clare, L., Victor, C., Matthews, F., Quinn, C., Hillman, A., Burns, A., Allan, L., Litherland, R., Martyr, A., Collins, P. and Pentecost, C.). ESRC is part of UK Research and Innovation (UKRI). The views expressed are those of the authors and not necessarily those of the ESRC or UKRI.
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
IDEAL was approved by Wales Research Ethics Committee 5 (reference 13/WA/0405) and IDEAL-2 by Wales Research Ethics Committee 5 (reference 18/WS/0111) and Scotland A Research Ethics Committee (reference 18/SS/0037). INCLUDE was approved as an amendment to IDEAL-2 for England and Wales (reference 18/WS/0111 AM12). IDEAL and IDEAL-2 are registered with the UK Clinical Research Network (numbers 16593 and 37955).







 Open access
Open access