

No CrossRef data available.
Article contents
Proposing the “continuum of UTI” for a nuanced approach to antimicrobial stewardship
Published online by Cambridge University Press: 29 September 2023
Abstract
Core share and HTML view are not available for this content. However, as you have access to this content, a full PDF is available via the ‘Save PDF’ action button.
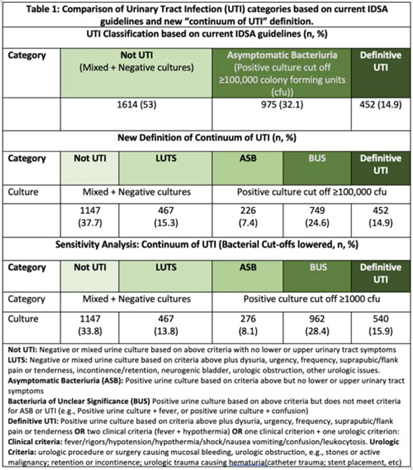
Background: Historically, diagnosis of urinary tract infections (UTIs) has been divided into 3 categories based on symptoms and urine culture results: not UTI, asymptomatic bacteriuria (ASB), or UTI. However, some populations (eg, older adults, catheterized patients) may not present with signs or symptoms referrable to the urinary tract or have chronic lower urinary tract symptoms (LUTS), making the diagnosis of UTI challenging. We sought to understand the clinical presentation of patients who receive urine tests in a cohort of diverse hospitals. Methods: This retrospective descriptive cohort study included all adult noncatheterized inpatient and ED encounters with paired urinalysis and urine cultures (24 hours apart) from 5 community and academic hospitals in 3 states (NC, VA, GA) between January 1, 2017, and December 31, 2019. Trained abstractors collected clinical and demographic data using a 60-question REDCap survey. The study group met with multidisciplinary experts (ID, geriatrics, urology) to define the “continuum of UTI” (Table 1), which includes 2 new categories: (1) LUTS to capture patients with chronic lower urinary tract symptoms and (2) bacteriuria of unclear significance (BUS) to capture patients who do not clinically meet criteria for ASB or UTI (eg, older adults who present with delirium and bacteriuria). The newly defined categories were compared to current guideline-based categories. We further compared ASB, BUS, and UTI categories using a lower bacterial threshold of 1,000 colony-forming units. Results: In total, 220,531 encounters met study criteria. After using a random number generator and removing duplicates, 3,392 encounters were included. Based on current IDSA guidelines, the prevalence of ASB was 32.1% (n = 975), and prevalence of patients with “not UTI” was 1,614 (53%). Applying the expert panel’s new “continuum of UTI” definitions, the prevalence of “not UTI” patients decreased to 1,147 (37.7%), due to reassignment of 467 patients (15.3%)to LUTS. The prevalence of ASB decreased by 24% due to reassignment to BUS. Lowering the bacterial threshold had a slight impact on the number of definitive UTIs (14.9 vs 15.9%) (Table 1). Conclusions: Our rigorous review of laboratory and symptom data from a diverse population dataset revealed that diagnostic uncertainty exists when assessing patients with suspicion for UTI. We propose moving away from dichotomous approach of ASB versus UTI and using the “continuum of UTI” for stewardship conversations. This approach will allow us to develop nuanced deprescribing interventions for patients with LUTS or BUS (eg, watchful waiting, shorter course therapy) that account for the unique characteristics of these populations.
Disclosures: None
- Type
- Antibiotic Stewardship
- Information
- Antimicrobial Stewardship & Healthcare Epidemiology , Volume 3 , Issue S2: SHEA Spring 2023 Abstracts , June 2023 , pp. s108
- Creative Commons

 This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.- Copyright
- © The Author(s), 2023. Published by Cambridge University Press on behalf of The Society for Healthcare Epidemiology of America
 You have
Access
You have
Access
 Open access
Open access