


Nuts are highly nutritious and especially rich in vitamins (e.g., vitamin E and folic acid), minerals (e.g., Mg and K), MUFA and PUFA, dietary fibre and other bioactive compounds including phytosterols, carotenoids and phenolics(Reference King, Blumberg and Ingwersen1). Aside from the nutritional perspective, previous studies suggested that nut intake was associated with glucose and blood lipid control, and modulation of inflammation, oxidative stress, endothelial function and insulin resistance(Reference Sabaté, Oda and Ros2–Reference Blomhoff, Carlsen and Andersen6). Through these mechanisms, nut intake may contribute to preventing CVD and other chronic diseases(Reference Luo, Zhang and Ding7–Reference van den Brandt and Schouten12). Although peanuts are legumes, they are treated as nuts because their nutrient contents are similar to those of almonds and other tree nuts(Reference Blomhoff, Carlsen and Andersen6).
Numerous epidemiological studies have suggested that nut intake is associated with reduced risks of all-cause, CVD and cancer mortality. Meta-analyses have revealed that compared with the lowest intake category, the highest intake category of nuts reduced the risk of all-cause mortality by 15 %–23 %(Reference Luo, Zhang and Ding7–Reference Mayhew, de Souza and Meyre10), CVD mortality by 25 %–29 %(Reference Grosso, Yang and Marventano8–Reference Zhang, Dai and Zhou11) and cancer mortality by 10 %–15 %(Reference Grosso, Yang and Marventano8,Reference Chen, Zhang and Martínez-González9,Reference Zhang, Dai and Zhou11,Reference van den Brandt and Schouten12) . The PREDIMED trial in Spain recently revealed that the risk of CVD was 28 % lower in subjects assigned to a Mediterranean diet supplemented with nuts than in those assigned to the control diet (advice on a low-fat diet)(Reference Estruch, Ros and Salas-Salvadó13). Although the Mediterranean population is well known to have a higher average intake level of nuts, most studies targeted European and North American populations(Reference Estruch, Ros and Salas-Salvadó13–Reference Fernández-Montero, Bes-Rastrollo and Barrio-López16). Considering the differences in diet and lifestyle, studies in different regions or races/ethnicities will provide additional insights into the association(Reference Mayhew, de Souza and Meyre10).
Till date, only two studies have investigated the associations between nut intake and all-cause and cause-specific mortality in non-Western countries, that is, China(Reference Luu, Blot and Xiang17) and Iran(Reference Eslamparast, Sharafkhah and Poustchi18). Although nuts were limited to peanuts in the Chinese study, nut intake was inversely associated with all-cause, CVD and cancer mortality, which is consistent with the findings of studies from Western countries. The Japanese population is unlikely to eat large amounts of nuts regularly. According to the National Health and Nutrition Survey(19), the mean intakes of nuts and seeds in Japanese men and women aged 20 years or older are 2·4 and 2·9 g/d, respectively. This is quite low compared with those in the Western populations. The Netherlands Cohort study reported that the average intakes of total nuts in Western men and women were 8·1 and 4·4 g/d, respectively(Reference van den Brandt and Schouten12). In the present study, we used data from a population-based cohort study in a Japanese community to examine the associations of total nut and peanut intakes with all-cause and cause-specific mortality.
Methods
Study participants
The Takayama study, a prospective cohort study, was initiated in 1992 and targeted all residents aged ≥ 35 years in Takayama City, Gifu, Japan. At baseline, a self-administered questionnaire was distributed to 36 990 residents. Among them, subjects who left four out of nine two-page spreads or more all blank, who answered only sixteen items or fewer, who were considered to be responded by other persons, who selected the food frequency category of ‘Never’ for all food items or who selected the food frequency category of ‘Once a day’ or ‘Two or more times a day’ for continuous forty food items or over were excluded from the study. Subjects who reported to have staple food (any kind of rice, bread, flour or noodles) five times or more, meat seven times or more, fish seven times or more, or ethanol 400 ml or more per day were also excluded. After these exclusions, the fixed cohort consisted of 31 552 subjects (response rate: 85·3 %)(Reference Shimizu20). Demographic characteristics, body weight and height, medical histories, and lifestyle and dietary habits (e.g., smoking, alcohol drinking and physical activity) were also collected. After excluding participants with a prior diagnosis of cancer (n 726), CHD (n 1451) or stroke (n 427) at baseline, 29 079 participants (13 355 men and 15 724 women) were included in the analyses.
Follow-up and end point
The participants were followed up from the baseline survey in September 1992 to the date of death or the end of follow-up (1 October 2008). The data of the participants who died or moved out of Takayama City were extracted from basic resident or family registration databases. The underlying causes of death were identified from death certificates provided by the Legal Affairs Bureau, which were coded according to the International Classification of Disease, Tenth Revision (ICD-10). The end points were total and cause-specific mortality, which included cancer (ICD-10 codes: C00–D48), CVD (ICD-10 codes: I00–I99), respiratory disease (ICD-10 codes: J10–J18 and J40–J47), digestive disease (ICD-10 codes: K00−K93) and other-cause mortality. The present study was approved by the ethics committee of the Gifu University Graduate School of Medicine.
Nut intake (exposure)
Dietary intake was assessed at baseline using a 169-item self-administered semi-quantitative FFQ. The participants reported how often and what amount of each food and beverage item they had consumed during the previous year. The FFQ was validated for subsamples of the cohort subjects by comparing a 3-d diet record, four 24-h recalls and a 12-d diet record over a year. Nutrient intakes were estimated from the data on frequency and portion size by using the fifth revised and enlarged edition of the Japanese Standard Tables of Food Composition. The FFQ and methods used for calculating the nutrient intakes were described in detail previously(Reference Shimizu, Ohwaki and Kurisu21). The FFQ contained eleven food items, including mixed nuts and dishes made with nuts (e.g., peanut butter, nut bread and rice cooked with chestnuts). Nut and peanut intakes were calculated according to the predetermined component food groups for each food item. The Spearman rank correlation coefficients between the FFQ and 12-d diet record for the estimated intakes of nuts and seeds were 0·45 and 0·36 in men and women, respectively. After adjusting for the total energy intake using the residual method of energy adjustment, we divided the participants into four groups according to the quartiles of total nut and peanut intakes, respectively.
Covariates
We considered the following variables measured at baseline as potential a priori confounders: age; sex; marital status (married or not married (single, divorced/separated or widowed)); years of education (≤8, 9–11, 12–14, or ≥15 years); BMI (in quartile, or missing); history of diabetes (no or yes); history of hypertension (no or yes); smoking status (never, former, current smoker or missing); alcohol intake; physical activity (continuous); use of any vitamin supplement (no, yes or missing); total energy intake per day (continuous); daily intakes of vegetables, fruits, and red meat (continuous) and menopausal status for women only (pre- or post-menopause). Alcohol intake was divided into quartiles for men and into three categories for women (non-drinkers, drinkers below the median value or drinkers above the median value). Physical activity was assessed with questions on the average time spent doing strenuous sports, vigorous work, and moderate exercise or work during the previous year. The time spent per week was multiplied by its corresponding energy expenditure (i.e., metabolic equivalent), and then the products were summed to yield a physical activity score (MET-h/week). This method and its validity were described in detail previously(Reference Suzuki, Kawakami and Shimizu22). Daily intakes of vegetables, fruits and red meat were adjusted for total energy intake using the residual method of energy adjustment(Reference Willet and Willett23).
Statistical analyses
All analyses were stratified by sex, considering that the association between nut intake and mortality may differ by sex. Person-years for each participant were counted from the date of the baseline survey to the date of death, date of censoring or end of follow-up (1 October 2008), whichever occurred first. Using Cox proportional hazards models, we first estimated the age-adjusted hazard ratios (HR) and 95 % CI for the associations of total nut and peanut intakes with all-cause and cause-specific mortality by using the first quartile category as the reference, respectively. Thereafter, we estimated HR after adjusting for all potential confounders by using the aforementioned method. In addition, we performed tests on linear trends for the associations estimated by the age- and fully-adjusted models. In so doing, we assigned the median values for each quartile category of total nut and peanut intakes.
In the sensitivity analyses, we repeated the analyses for the associations with all-cause mortality and cause-specific mortality using two different exposure categorisations as follows: we divided the fourth quartile of nut intake in halves and created a total of five categories, that is, first, second, third, fourth (lower half) and fourth (upper half) quartile categories for total nuts and peanuts, respectively; and we used the weekly frequency intake of mixed nuts, that is, none, <1 and ≥1 time/week. To examine the impact of reverse causation by preclinical disorders, we repeated the analyses for the associations of total nut and peanut intakes with all-cause mortality after excluding the data of the participants who died within the first 2 years of follow-up and who reported a prior diagnosis of diabetes at baseline. We further adjusted for a history of drug treatment for hypertension instead of its prior diagnosis in the multivariate models. To reduce the possibility of residual confounding from daily healthy diet and lifestyle, we adjusted for overall diet quality instead of daily intakes of vegetables, fruits and red meat in the multivariate models, and additionally adjusted for the intakes of total soya food and other types of nuts in the separate multivariate models. Adherence to the Japanese food guide (the Japanese Food Guide Spinning Top) was measured on a seventy-point scale based on consuming the recommended number of servings of grains, vegetables, fish and meat, milk, and fruits, as well as total daily energy intake and energy from snacks and alcoholic beverages(Reference Oba, Nagata and Nakamura24). Higher adherence scores were assumed as better overall diet quality. In addition, we conducted stratified analyses for all-cause mortality by risk factors (smoking status, BMI and physical activity). The proportional hazards assumption was examined by a test using Schoenfeld residuals and visual inspection of log-log plots, with no violations detected. A two-sided P value < 0·05 was considered statistically significant. Effect modification was tested by an interaction term in the multivariate models, that is, product of nut intake (median of quartiles) and the selected risk factor (binomial). The Stata/SE statistical software (version 16.1; StataCorp) was used for all the analyses.
Results
The mean intakes of total nuts were 1·8 (sd 3·6) and 1·5 (sd 2·6) g/d in men and women, respectively, and those of peanuts were 1·4 (sd 3·3) and 1·2 (sd 2·4) g/d in men and women, respectively. Table 1 shows the baseline characteristics of the male and female participants according to the quartile categories of total nut intake. Compared with the men in the lowest quartile category, those in the highest quartile category were more likely to be highly educated and were less likely to be current smokers and have a history of hypertension. Compared with the women in the lowest quartile category, those in the highest quartile category were less likely to be current smokers. A similar tendency in men and women was observed for peanut intake (online Supplementary Table 1).
Table 1. Age-standardised baseline characteristics* of male and female participants, according to total nut intake
(Numbers and percentages; mean values and standard deviations; median and interquartile range (IQR))

IQR, interquartile range; MET, metabolic equivalent.
* Continuous variables were age-adjusted by linear regression models (age: continuous), and categorical variables were age-adjusted by direct methods (age: 5 strata) using total male and female participants, respectively, as a standard population.
Table 2 shows the associations of total nut intake with all-cause mortality and mortality from cancer, CVD, respiratory disease, digestive disease and other causes. During the 16 years of follow-up (mean follow-up: 13·7 years; 183 299 total person-years), 2901 men died. Total nut intake was associated with a reduced risk of all-cause and digestive disease mortality in the men after adjusting for all potential confounders. In men, diseases of liver were the primary causes of death due to digestive disease and accounted for 52·5 % of total digestive disease mortality. For example, compared with the first quartile category, the HR (95 % CI) of total nut intake for all-cause mortality in the men of the second, third and fourth quartile categories were 0·88 (95 % CI 0·79, 0·99), 0·89 (95 % CI 0·79, 1·02) and 0·85 (95 % CI 0·75, 0·96), respectively (P for trend = 0·034). During the 16 years of follow-up (mean follow-up: 14·4 years; 227 054 total person-years), 2438 women died. The total nut intake was marginally associated with a reduced risk of all-cause and CVD mortality in the women of the fourth quartile category as compared with those in the first quartile category; however, no linear trends for the associations were statistically significant. Although a similar tendency was observed for the associations of total nut and peanut intakes with all-cause and cause-specific mortality in the men and women, a linear trend in the association between peanut intake and CVD mortality in the women turned to be significant (P for trend = 0·036; Table 3).
Table 2. All-cause and cause-specific mortality stratified by sex, according to total nut intake
(Hazard ratio (HR) and 95 % confidence intervals)
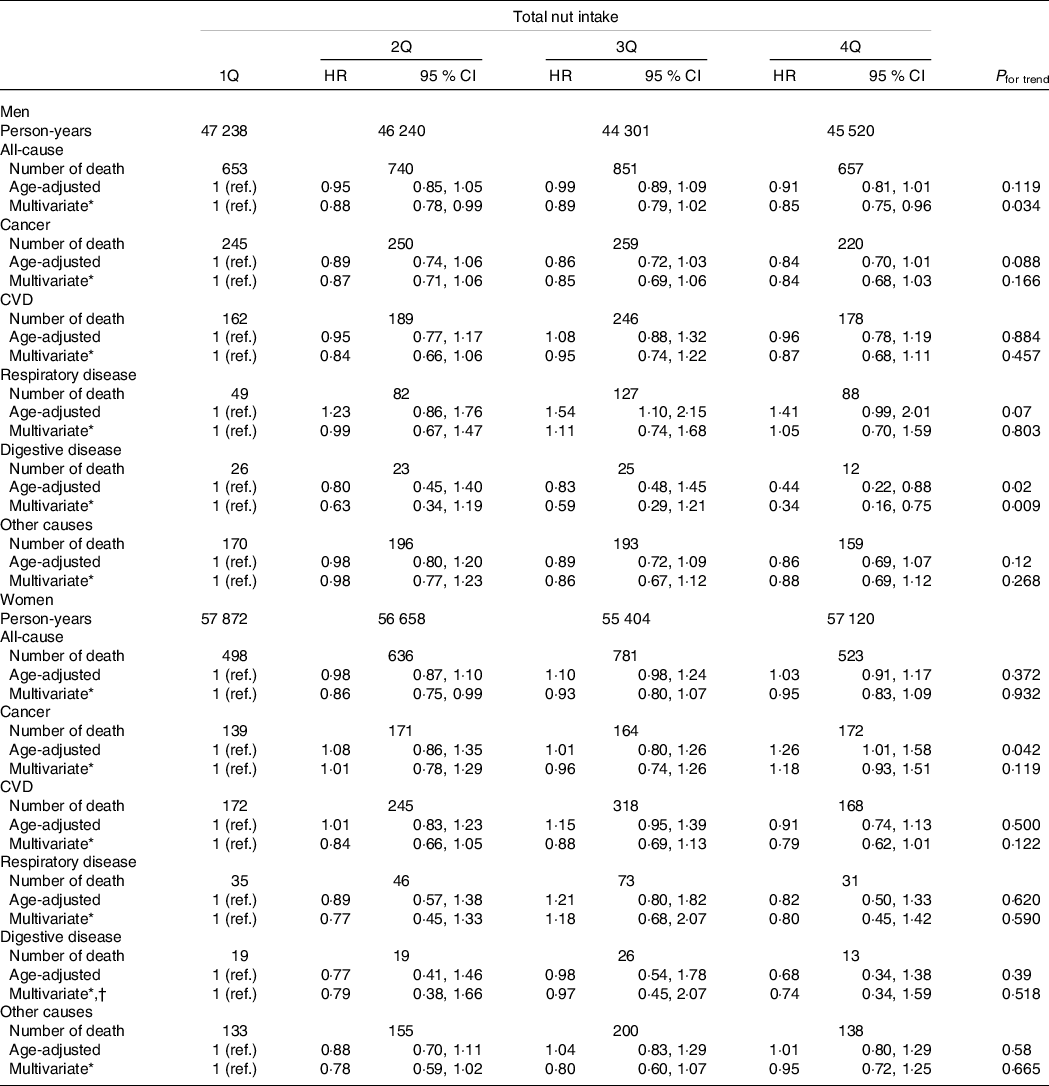
ref., reference; Q, quartile.
* Age, marital status, years of education, BMI, diabetes, hypertension, smoking status, alcohol intake, physical activity, use of any vitamin supplement, dietary intake (total energy, vegetables, fruits and red meat) and menopausal status (women only) were adjusted for.
† The multivariate HR were estimated after the higher two categories of years of education were collapsed into a single category (i.e., ≥12 years).
Table 3. All-cause and cause-specific mortality stratified by sex, according to peanut intake
(Hazard ratio (HR) and 95 % confidence intervals)
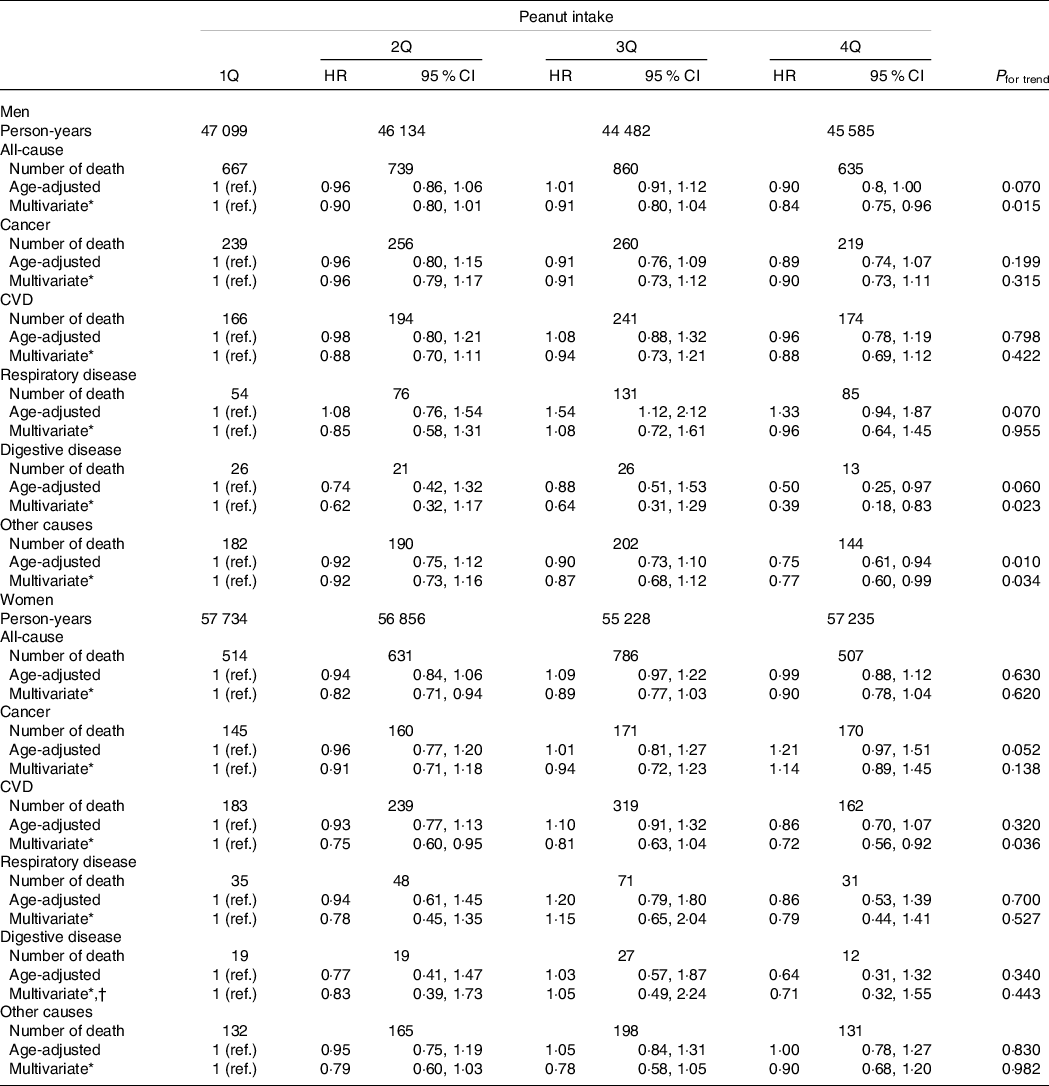
ref., reference; Q, quartile.
* Age, marital status, years of education, BMI, diabetes, hypertension, smoking status, alcohol intake, physical activity, use of any vitamin supplement, dietary intake (total energy, vegetables, fruits and red meat) and menopausal status (women only) were adjusted for.
† The multivariate HR were estimated after the higher two categories of years of education were collapsed into a single category (i.e., ≥12 years).
In the sensitivity analyses, the results for the associations with all-cause mortality and cause-specific mortality using the two different exposure categorisations remained compatible with those with the main analyses (online Supplementary Tables 2 and 3). For example, the HR (95 % CI) of total nut intake for all-cause mortality in the men of the second, third, fourth (lower half) and fourth (upper half) quartile categories, as compared with those of the first quartile category, were 0·88 (95 % CI 0·79, 1·00), 0·91 (95 % CI 0·80, 1·03), 0·91 (95 % CI 0·78, 1·05) and 0·80 (95 % CI 0·69, 0·93), respectively (P for trend = 0·010). Excluding the participants who died in the first 2 years of follow-up and who had a prior diagnosis of diabetes at baseline, and adjusting for a history of drug treatment for hypertension instead of its prior diagnosis did not substantially change the main findings of the present study (online Supplementary Table 4). For example, after excluding the first 2-year deaths, the HR (95 % CI) of peanut intake for all-cause mortality in the men of the second, third and fourth quartile categories, as compared with those of the first quartile category, were 0·89 (95 % CI 0·79, 1·01), 0·92 (95 % CI 0·80, 1·05) and 0·86 (95 % CI 0·76, 0·98), respectively (P for trend = 0·051). Adjusting for overall diet quality instead of daily intakes of vegetables, fruits and red meat, and additionally adjusting for the intakes of total soya food and other types of nuts did not substantially change the present findings. The stratified analyses indicated that the associations of total nut intake with all-cause mortality were similar between the strata of the selected risk factors except for physical activity. In both men and women, a higher intake of nuts was associated with a lower risk for all-cause mortality among the participants who were more physically active, but not among those who were less physically active (online Supplementary Table 5).
Discussion
In the present study, we targeted community-dwelling people in Japan to evaluate the associations of total nut and peanut intakes with all-cause and cause-specific mortality. We used the data of a Japanese community from a population-based prospective cohort study, the Takayama study. The results showed that despite the extremely low intake levels, total nut and peanut intakes were associated with a reduced risk of all-cause mortality, particularly in men, after adjusting for all potential confounders. In addition, total nut and peanut intakes were associated with a reduced risk of digestive disease mortality in men. Furthermore, peanut intake was associated with a reduced risk of CVD mortality in women.
Meta-analyses have consistently reported the protective effects of nut intake on all-cause and CVD mortality(Reference Luo, Zhang and Ding7–Reference Mayhew, de Souza and Meyre10). Moreover, clinical trials have compiled evidence for the positive effects of nut intake on markers related to CVD and other chronic conditions, for example, blood lipid levels and endothelial function(Reference Sabaté, Oda and Ros2–Reference Casas-Agustench, López-Uriarte and Ros5). Recently, the PREDIMED trial demonstrated that compared with the control diet, the Mediterranean diet supplemented with nuts (30 g/d) had protective effects on CVD(Reference Estruch, Ros and Salas-Salvadó13). In addition, previous studies suggested that nut intake was associated with glucose control, and modulation of inflammation, oxidative stress and insulin resistance. These mechanisms may have beneficial impacts on the prevention of CVD and other chronic diseases, leading to all-cause mortality reduction. Although a gap in intake levels exists, the findings of previous studies and the biological plausibility of nutrients in nuts support the present findings regarding all-cause mortality in men and CVD mortality in women.
Peanut intake accounted for approximately 80 % of the total nut intake in our participants. In addition, we observed inverse associations of peanut intake with all-cause and CVD mortality, and the estimates appeared to be comparable in direction and magnitude with those of total nut intake; therefore, the observed associations for total nuts may be attributed to peanuts. Moreover, a meta-analysis indicated that peanut intake was inversely associated with all-cause and CVD mortality(Reference Chen, Zhang and Martínez-González9). Furthermore, the findings for peanut intake are biologically plausible considering the similarity in nutrients between peanuts and almonds and other tree nuts(Reference Blomhoff, Carlsen and Andersen6).
We failed to find a clear linear trend in the associations of nut intake with all-cause mortality in women and CVD mortality in men. At least two explanations are possible. As indicated in previous studies(Reference Luo, Zhang and Ding7,Reference Luu, Blot and Xiang17) , small variations in intake levels can hinder the detection of a statistically significant difference. In the present study, the mean of nut intake was low and its variation was small in both sexes. Furthermore, the beneficial impacts of nut intake may reflect other characteristics of nut eaters; for example, people who eat nuts are assumed to live a healthy life(Reference Katz25). Although we carefully evaluated the associations after adjusting for important diet and lifestyle factors, the possibility of residual confounding from other dietary and lifestyle factors cannot be ruled out.
In the present study, nut intake was not associated with cancer mortality in women. However, an inverse association of nut intake with cancer mortality was marginally significant in men of the highest quartile category, indicating that the associations might have differed by sex. This appears to be consistent with the findings of a cohort study in Iran, which reported that nut intake lowered the risk of cancer mortality in women but not in men(Reference Eslamparast, Sharafkhah and Poustchi18). These sex-differentiated associations could be due to chance. Four meta-analyses have suggested the protective effect of nut intake on cancer mortality(Reference Grosso, Yang and Marventano8,Reference Chen, Zhang and Martínez-González9,Reference Zhang, Dai and Zhou11,Reference van den Brandt and Schouten12) . However, one of the four meta-analyses that combined four cohorts in Europe and the USA presented no evidence for heterogeneity in the associations between men and women(Reference van den Brandt and Schouten12). An explanation for this inconsistency in findings may be that the common causes of cancer mortality differ by sex and regions or races/ethnicities(Reference Luu, Blot and Xiang17,Reference Eslamparast, Sharafkhah and Poustchi18) . Further studies evaluating the associations of nut intake with site-specific cancer mortality stratified by sex in different regions or races/ethnicities are warranted.
We found that nut intake was inversely associated with digestive disease mortality, particularly in men, but not with respiratory disease mortality. This is inconsistent with the findings of two cohort studies that suggested inverse associations between nut intake and respiratory disease mortality(Reference van den Brandt and Schouten12,Reference Bao, Han and Hu26) . By contrast, another study indicated that nut intake was inversely associated with mortality from inflammatory diseases, including respiratory disease and digestive disease(Reference Gopinath, Buyken and Flood27). Regarding digestive disease mortality, diseases of liver were the primary causes of death due to digestive disease in our cohort and accounted for 52·5 and 29·3 % of total digestive mortality in men and women, respectively. A review summarised potential benefits of nut intake to the liver, that is, improvement of liver function tests, and reduction of non-alcoholic fatty liver disease development and oxidative stress(Reference Gupta, Mah and Garcia28). An epidemiological study of Iran reported that nut intake was negatively associated with the severity of hepatic cirrhosis(Reference Pashayee-Khamene, Saber-Firoozi and Hatami29). These mechanisms may support the present findings for digestive disease mortality. In addition, a gap of digestive disease mortality between men and women could explain the sex-differentiated associations for digestive disease mortality and all-cause mortality. Future studies investigating the associations between nut intake and digestive disease mortality and a difference in the associations by sex are warranted.
The major strengths of this study are that we used data from a prospective population-based cohort study in Japan with 16 years of follow-up and a high participation rate (85·3 %). Another strength is the use of a validated dietary questionnaire. Furthermore, we examined important diet and lifestyle factors, including a validated physical activity level. The present findings provide further evidence of the beneficial impacts of peanut intake among non-white, non-Western populations.
The present study has several limitations. First, self-reported dietary intake may have influence on our results, just as in other studies on nutritional epidemiology; however, it is unlikely that nut intake at baseline in the deceased participants would be systematically underestimated. Second, because nut intake was assessed only at baseline, it may not reflect long-term intake. A study of two prospective US cohorts revealed that nut intake remained constant over 20 years during the study follow-up period, although the dietary intake was measured every 2–4 years(Reference Bao, Han and Hu26). People with one or more chronic diseases may alter their nut intake. However, we excluded such participants from the analyses. Moreover, we conducted sensitivity analyses after excluding the data of participants who died within the first 2 years and who reported a prior diagnosis of diabetes at baseline and adjusting for a history of drug treatment instead of a prior diagnosis for hypertension; however, these did not substantially change the present findings. Second, information regarding foods containing tree nuts may be lacking. For example, in the target area of the study (Takayama city), local sweets such as gohei mochi (rice cake with salty-sweet sauce containing walnuts) contain walnuts. Information bias due to local sweets is likely to occur, particularly in women, considering the moderate correlation for the intake of nuts and seeds. However, this would be a non-differential misclassification, making the estimates towards the null. Third, as mentioned earlier, the possibilities of residual confounding from other diet and lifestyle factors and effect modification by physical activity cannot be ruled out, although the associations were evaluated after adjusting for all potential confounders. Finally, despite the various sensitivity analyses, there is some possibility that the protective associations for the overall low intake of nuts could occur due to confounding by unknown factors and residual confounding. Further studies targeting the populations who eat few nuts are thus needed.
In conclusion, we found that total nut and peanut intakes were associated with a reduced risk of all-cause mortality, particularly in men, and cause-specific mortality (digestive disease mortality in men and CVD mortality in women). Peanuts are more ubiquitously available and reasonably priced than tree nuts, particularly in Asia. Therefore, casual intake of peanuts, even in low amounts, could contribute to long life in Japan and other Asian countries.
Acknowledgements
This work was supported in part by grants from the Ministry of Education, Culture, Sports, Science, and Technology, Japan. The sponsor was not involved in deciding the study design, the collection, analysis and interpretation of data, the writing of the report and the decision to submit this paper for publication.
This work was supported in part by grants from the Ministry of Education, Culture, Sports, Science, and Technology, Japan. The sponsor was not involved in deciding the study design; the collection, analysis and interpretation of data; and the writing of the report and decision to submit this paper for publication.
M. Y., K. W., S. K., T. U., Y. N., Sa. O., Sh. O. and C. N. designed the study and analytical strategy; K. W., Sh. O. and C. N. obtained data; M. Y., S. K., T. U., Y. N., Sa. O. and Sh. O. performed the analysis and interpretation of data; M. Y. drafted the initial manuscript; K. W., S. K., T. U., Y. N., Sa. O., Sh. O. and C. N. reviewed and revised the manuscript; C. N. obtained the grants and supervised the study; and all authors approved the final manuscript as submitted.
The authors have no conflicts of interest to disclose.
Supplementary material
For supplementary material referred to in this article, please visit https://doi.org/10.1017/S0007114521002257





