


Introduction
Psychological distress among higher education students is a growing concern, both internationally and in Ireland (Royal College of Psychiatrists, 2011; Eisenberg et al. Reference Eisenberg, Hunt and Speer2013; Dooley et al. Reference Dooley, O’Connor, Fitzgerald and O’Reilly2019). For example, in the United Kingdom (UK), approximately one in three university students experience clinical levels of psychological distress (Bewick et al. Reference Bewick, Gill, Mulhern, Barkham and Hill2008), while Brown (Reference Brown2016) concluded that young people in higher education may be at greater risk of mental health problems than non-students. This is because periods of transition, such as progressing to higher education and adjusting to new circumstances, are associated with an increased risk of developing mental health problems, while peer pressure and the need to adapt to new forms of learning can also contribute to the mental ill health of students (Brown, Reference Brown2016).
In the United States (US), a number of studies have also found a high overall prevalence of mental health problems among college students (Eisenberg et al. Reference Eisenberg, Hunt and Speer2013; American College Health Association, 2018). Holm-Hadulla & Koutsoukou-Argyraki (Reference Holm-Hadulla and Koutsoukou-Argyraki2015) examined data on the prevalence of complaints and disorders across a range of countries and found that psychological and mental disorders in students are highly prevalent. As well as the personal consequences for students themselves, which can include diminished wellbeing, unhappiness, social isolation, and decreased enjoyment of life, the high prevalence of mental health problems amongst students has a range of implications for the higher education sector. For example, poor mental health affects both student retention and academic performance (Eisenberg et al. Reference Eisenberg, Hunt and Speer2013; Hysenbegasi et al. Reference Hysenbegasi, Hass and Rowland2005; Keyes et al. Reference Keyes, Eisenberg, Perry, Dube, Kroenke and Dhingra2012). Additionally, demand for student counseling services has risen internationally, which has led to long waiting times in many HEIs due to resource limitations (Prince, 2015).
Many of the findings in the international literature are consistent with previous studies in Ireland. For example, Deasy et al. (Reference Deasy, Coughlan, Pironom, Jourdan and Mannix-McNamara2016) found a high prevalence of significant psychological distress amongst nursing/midwifery and teacher education students. Sources of distress included academic, financial, and psychosocial stressors, while demographic, programmatic, and lifestyle variables were also found to be associated with higher levels of psychological distress. In another study, McLafferty et al. (Reference McLafferty, Lapsley, Ennis, Armour, Murphy, Bunting, Bjourson, Murray and OʼNeill2017) considered behavioral problems and treatment seeking among students commencing a university in Northern Ireland, finding 22.3% of students with problems would not seek help. In a recent national survey of 3,340 higher education students in Ireland by the Union of Students in Ireland (USI), Price and Smith (Reference Price and Smith2019) reported high levels of anxiety, depression and stress, including large differences in outcomes across student groups. However, the report did not include any statistical analysis of these differences. In relation to mental health service use, Cullinan et al. (Reference Cullinan, Walsh and Flannery2020) found evidence of large socioeconomic disparities in unmet need, which were driven by higher rates of mental ill health among those from lower socioeconomic backgrounds. In addition, there have also been important studies focussing on younger people in Ireland more generally, rather than higher education students specifically (Cannon et al. Reference Cannon, Coughlan, Clarke, Harley and Kelleher2013; Dooley et al. Reference Dooley, O’Connor, Fitzgerald and O’Reilly2019). Most recently, Dooley et al. (Reference Dooley, O’Connor, Fitzgerald and O’Reilly2019) analyzed a large sample of young people, including both students and non-students, and found high rates of depression and anxiety.
Nonetheless, despite this previous research, there remain gaps in the literature on the prevalence of, and variation in, psychological distress among higher education students in Ireland. This is important, since reliable information on the prevalence of psychological distress among higher education students and across specific groups is needed so that campus counseling services and HEI managers can better support students who are experiencing mental health issues (Sharp & Theiler, Reference Sharp and Theiler2018). Indeed, the National Student Mental Health and Suicide Prevention Framework in Ireland stresses the need to identify students who are at risk of mental health problems, as well as promote mental health awareness for all students and all front-facing staff (HEA, 2020). It is also important to track changes in student mental ill health over time, both in overall terms and by subgroup, in order to identify potentially problematic trends and/or developments that need to be addressed. For example, it seems highly likely that the COVID-19 pandemic will result in increases in the prevalence of psychological distress and disparities across student groups. In this context, and given the significant personal and societal costs associated with mental ill health, this paper aims to examine levels of psychological distress among a large and broadly representative sample of higher education students in Ireland overall and across a range of personal, higher education, and socioeconomic characteristics.
Methods
Study design
A cross-sectional online survey was used to explore levels of, and differences in, stress, anxiety, and depression symptom scores and associated severity categories in a large sample of higher education students in Ireland.
Setting
The higher education sector in Ireland is currently comprised of universities, technological universities (TUs), institutes of technology (ITs), as well as a small number of other public and private colleges, though at the time of our survey there were no TUs. Compared to universities, ITs have a larger proportion of mature and disadvantaged students, while there are also differences in the nature and range of fields of study on offer (HEA, 2019). Mental health service provision is institution-specific in Ireland, with budgets and the type of provision decided by each HEI individually. Expenditure per student on mental health services tends to be lower in ITs compared to universities (Walsh et al. Reference Walsh, Cullinan, Flannery and Kennelly2020). Regarding provision, there are some commonalities, with all HEIs offering some form of one-to-one counseling service on an appointment basis. However, differences also exist, with some HEIs offering wellness and resilience programs, workshops and online self-help resources.
Recruitment
The data used are from a national survey of higher education students in Ireland conducted in February and March 2018. While the survey focussed on eliciting student preferences for campus counseling services using a discrete choice experiment (Walsh et al. Reference Walsh, Cullinan, Flannery and Kennelly2020), a range of supplementary questions were also included, which are the focus of this analysis. The survey questionnaire was developed through an iterative design process, involving a literature review, focus groups, pre-pilot interviews, and a pilot study of higher education students, and was targeted at students enrolled in higher education in Ireland. In order to recruit students, a letter of invitation was sent to the Registrar (Deputy President) of each of 26 HEIs in Ireland (see Appendix 1 in the supplementary online material) and, if the Registrar agreed, an email was sent to all registered students inviting them to participate in an online survey, subject to being 18 years or older. Upon completion of the survey, respondents were provided with information on relevant support agencies. Ethical approval was provided by the NUI Galway Research Ethics Committee.
Psychological distress instrument
The 21-item Depression, Anxiety and Stress Scale (DASS) instrument was used to measure psychological distress among respondents. The DASS, though not a diagnostic tool, is a widely used measure in both clinical practice and research. It includes three independent self-reported subscales that assess the severity of symptoms associated with depression, anxiety, and stress respectively (Lovibond & Lovibond, Reference Lovibond and Lovibond1995). Following Cullinan et al. (Reference Cullinan, Walsh and Flannery2020) and Larcombe et al. (Reference Larcombe, Finch, Sore, Murray, Kentish, Mulder, Lee-Stecum, Baik, Tokatlidis and Williams2016), and to make the main results easier to present and discuss, we analyzed three separate severity categories based on DASS scores i.e. normal, mild/moderate, and severe/extremely severe. In terms of service provision, those in the latter severity category are likely to be in need of professional help. It should be noted that our main findings and conclusions were not sensitive to a more disaggregated set of severity categories.
Independent variables
Data in relation to a range of personal, higher education, and socioeconomic variables were also collected as part of the survey. Personal characteristics included information on a respondent’s age, gender, sexual orientation, and country where they were born. Higher education related variables included information on enrollment type (i.e. undergraduate or postgraduate), year of study, and the specific HEI they were attending. Finally, socioeconomic variables included a student’s social class and difficulty ‘making ends meet’, with the latter used as a proxy variable for financial difficulties.
Analysis
Statistical analysis was undertaken using Stata version 16.1. Since the DASS severity categories are ordinal, Wilcoxon–Mann–Whitney and Kruskal–Wallis tests were performed to assess statistical differences in categories across student groups defined on the basis of personal, higher education, and socioeconomic variables. The Wilcoxon–Mann–Whitney test is a rank-based nonparametric analog to the independent samples t-test and was used when considering an independent variable with two levels (i.e. independent groups). The test then considers the hypothesis that the two groups are from populations with the same distribution of the dependent variable. The Kruskal–Wallis test is also a rank-based nonparametric test that can be used to determine if there are statistically significant differences between groups of an independent variable on an ordinal dependent variable. The null hypothesis of the Kruskal–Wallis test is that the mean ranks of the groups are the same and we employ this test where there are three or more categories of the independent variable under consideration.
In addition to the main analysis, we also consider issues relating to missing data and self-selection, and their implications for our results and findings. Details are presented in the appendices in the supplementary online materials.
Results
Participants
Overall, 6,508 students took part in the survey from 13 HEIs that agreed to partake, giving a HEI response rate of 50%. The average response rate at a national level from students in higher education was 4.3%. In order to reduce the risk of low-quality data, we dropped respondents who completed the survey in less than five minutes (878 respondents) – this cutoff was based on tests conducted by the authors on what would constitute a minimum time for accurately completing the online questionnaire and is consistent with the cutoff used in Cullinan et al. (Reference Cullinan, Walsh and Flannery2020) and Walsh et al. (Reference Walsh, Cullinan, Flannery and Kennelly2020). We also dropped respondents who had missing data on variables relating to mental health, or on the personal, higher education, or socioeconomic characteristics analyzed here (429 respondents). This resulted in a final estimation sample of 5,201 individuals.
Descriptive statistics
Sample descriptive statistics are presented in Table 1. For our sample of 5,201 students, the mean DASS score for depression was 11.7 (standard deviation (SD): 10.6), the mean score for anxiety was 8.8 (SD: 8.7), while the mean score for stress was 13.8 (SD: 9.8). Figures A2.1–A2.3 in Appendix 2 in the supplementary online material present graphical illustrations of group variation in mean DASS scores for depression, anxiety, and stress respectively, showing notable differences by age, gender, sexual orientation, enrollment type, HEI type, social class, and ability to make ends meet. No differences in mean scores are apparent for country of birth or year of study, apart from some evidence of differences in the former for stress (see Figure A2.3). For information, Appendix 2 in the supplementary online material also presents full details of mean DASS scores for depression, anxiety, and stress across groups.
Table 1. Variable definitions and sample descriptive statistics
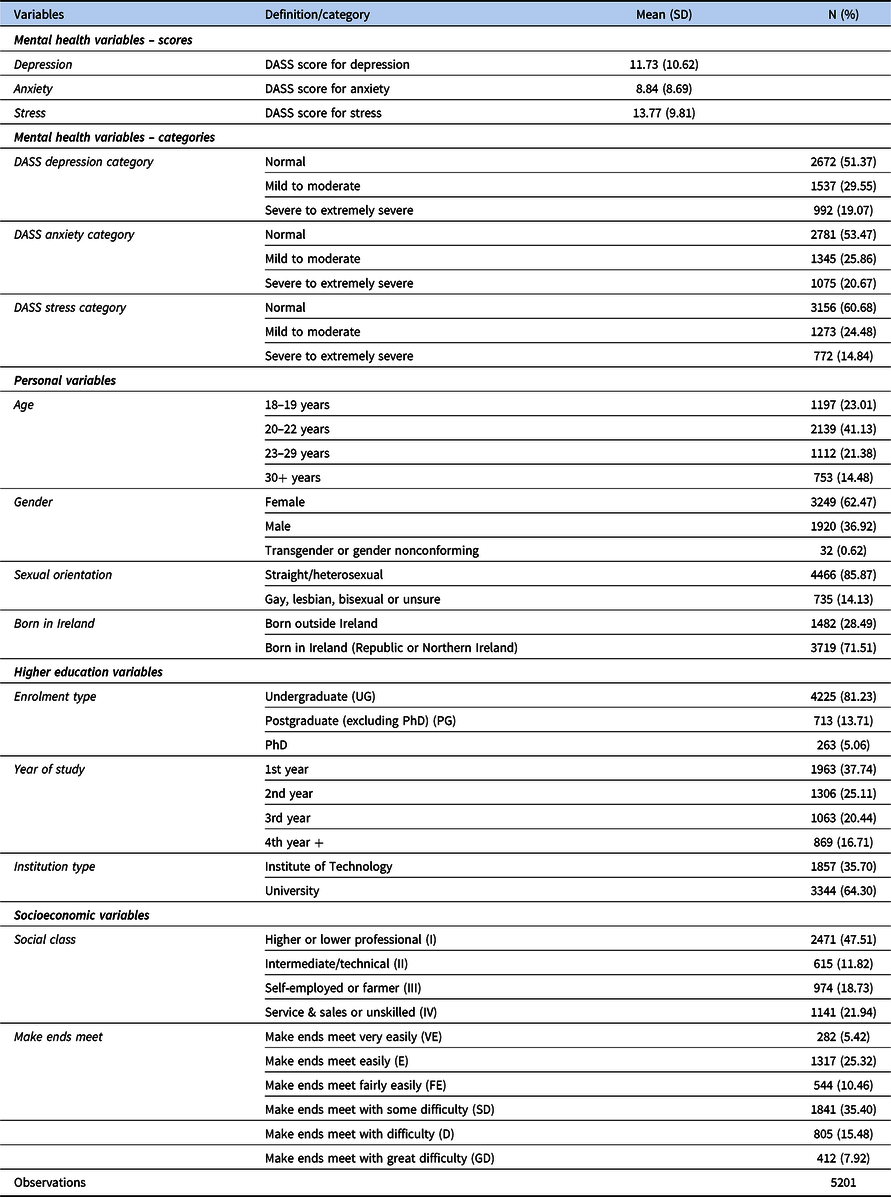
Source: Analysis of data from Walsh et al. (Reference Walsh, Cullinan, Flannery and Kennelly2020).
In terms of severity categories, overall 29.6% of respondents were classified in the mild to moderate range for depression based on their self-reported DASS scores and 19.1% were in the severe to extremely severe range – see Table 1. The corresponding proportions were 25.9% and 20.7% for anxiety and 24.5% and 14.8% for stress. Table 1 also reports sample descriptive statistics for all of the personal, higher education, and socioeconomic variables considered in the analysis.
Main results
Tables 2–4 present the main results.Footnote 1 Starting with personal characteristics, Table 2 shows statistically significant differences in categories of depression (χ2 = 19.85, p < 0.01), anxiety (χ2 = 37.19, p < 0.01), and stress (χ2 = 19.40, p < 0.01) by age, with students aged 30+ years having lower rates on average. Differences are also evident by gender (depression: χ2 = 37.50, p < 0.01; anxiety: χ2 = 71.28, p < 0.01; stress: χ2 = 86.31, p < 0.01), with transgender students having notably higher rates of psychological distress across all three dimensions, and females having higher rates than males, on average. There are also significant differences by sexual orientation (depression: z = −10.09, p < 0.01; anxiety: z = −8.38, p < 0.01; stress: z = −10.26, p < 0.01), with gay, lesbian, bisexual, or unsure students having much higher rates of severe to extremely severe psychological distress than heterosexual students on average. Table 2 suggests no difference in depression (z = 0.10, p = 0.92) or anxiety (z = −0.39, p = 0.69) between students born in or outside Ireland, but some evidence of greater stress for students born in Ireland (z = −2.73, p < 0.01).
Table 2. DASS category breakdowns by personal characteristics
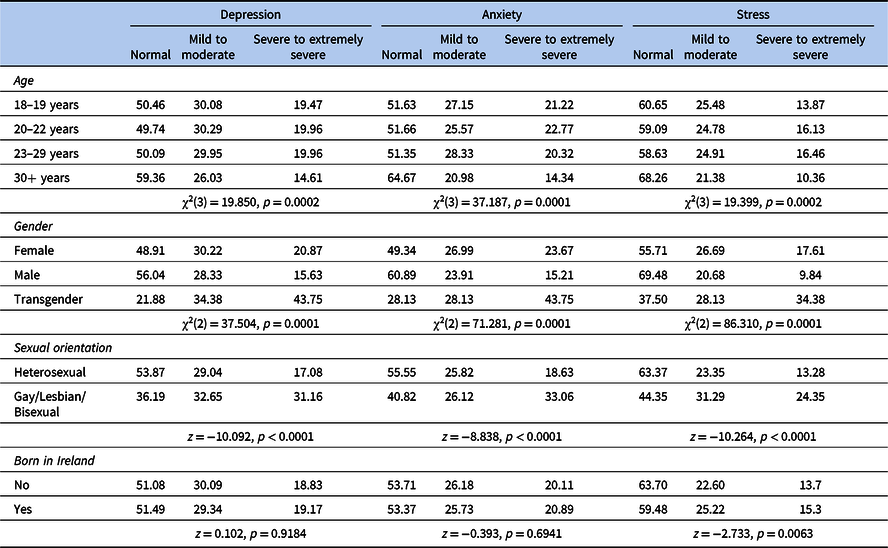
Source: Analysis of data from Walsh et al. (Reference Walsh, Cullinan, Flannery and Kennelly2020).
Note: z statistics relate to Wilcoxon–Mann–Whitney rank-based tests (used where there are two categories for an independent variable) and χ2 statistics relate to Kruskal–Wallis equality-of-populations rank tests (used where there are three or more categories for an independent variable).
Table 3. DASS category breakdowns by higher education characteristics

Source: Analysis of data from Walsh et al. (Reference Walsh, Cullinan, Flannery and Kennelly2020).
Note: z statistics relate to Wilcoxon–Mann–Whitney rank-based tests (used where there are two categories for an independent variable) and χ2 statistics relate to Kruskal–Wallis equality-of-populations rank tests (used where there are three or more categories for an independent variable).
Table 4. DASS category breakdowns by socioeconomic characteristics
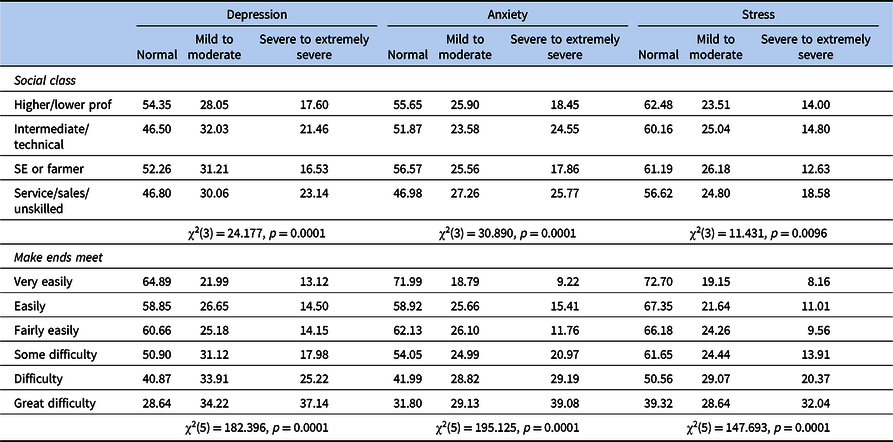
Source: Analysis of data from Walsh et al. (Reference Walsh, Cullinan, Flannery and Kennelly2020).
Note: χ2 statistics relate to Kruskal–Wallis equality-of-populations rank tests.
Table 3 shows there are also significant differences by some higher education characteristics. For example, it shows statistically significant differences by enrollment type (depression: χ2 = 16.11, p < 0.01; anxiety: χ2 = 27.08, p < 0.01; stress: χ2 = 14.63, p < 0.01), with much higher rates of severe to extremely severe depression amongst undergraduate students compared to postgraduate and PhD students on average. However, year of study is not found to be statistically significant (depression: χ2 = 4.33, p = 0.23; anxiety: χ2 = 1.25, p = 0.74; stress: χ2 = 5.27, p = 0.15). There are notable differences in all three measures of psychological distress by HEI type (depression: z = 3.74, p < 0.01; anxiety: z = 6.57, p < 0.01; stress: z = 3.52, p < 0.01). In particular, students in ITs have higher rates of severe to extremely severe psychological distress than students in universities on average, while severe to extremely severe rates of depression, anxiety, and stress range from 10.8% to 26.8%, 16.9% to 38.9%, and 8.43% to 27.8%, respectively.
Finally, Table 4 presents similar analysis for the two socioeconomic characteristics considered. There are statistically significant differences in all three measures of psychological distress by social class (depression: χ2 = 24.18, p < 0.01; anxiety: χ2 = 30.89, p < 0.01; stress: χ2 = 11.43, p < 0.01) and by ability to makes ends meet (depression: χ2 = 182.40, p < 0.01; anxiety: χ2 = 195.13, p < 0.01; stress: χ2 = 147.69, p < 0.01). For social class, rates of depression, anxiety, and stress tend to be higher for intermediate/technical and service/sales/unskilled groups compared to higher/lower professional and self-employed/farmer groups. Differences across the ability to make ends meet spectrum (i.e. from ‘very easily’ to ‘with great difficulty’) are particularly pronounced, ranging, for example, from 13.1% to 37.1% for depression, 9.2% to 39.1% for anxiety, and 8.2% to 32.0% for stress.
Discussion
Robust and detailed data on the prevalence and correlates of psychological distress among higher education students is vital so that campus counseling services and HEI managers, faculty, and administrators can better support students who are experiencing mental health issues (HEA, 2020). Such information can also help support policymakers at the national level. This paper is the first to provide evidence of the prevalence of psychological distress along with a statistical analysis of differences across student groups using a large-scale survey of higher education students in Ireland. In that regard, it augments previous research focussing on the mental health of this cohort (Price & Smith, Reference Price and Smith2019; Cullinan et al. Reference Cullinan, Walsh and Flannery2020).
Based on our survey, we find high levels of psychological distress in the student population. Overall, 29.6% and 19.1% of our estimation sample are classified in the mild to moderate and severe to extremely severe ranges for depression, respectively. The corresponding proportions are 25.9% and 20.7% for anxiety, and 24.5% and 14.8% for stress. We also find considerable variation in these figures across various personal, higher education, and socioeconomic characteristics. In particular, higher levels of psychological distress are found among transgender and female students compared to males, gay/lesbian/bisexual students compared to heterosexual students, undergraduates compared to postgraduates, students from intermediate/technical or service/unskilled social classes compared to professional/self-employed classes, as well as for students having financial difficulties. Levels of psychological distress were lower for those studying at university relative to ITs. Overall our results show high rates of mental ill health among students in higher education in Ireland. They also provide evidence of considerable heterogeneity across student groups.
In previous Irish research, McLafferty et al. (Reference McLafferty, Lapsley, Ennis, Armour, Murphy, Bunting, Bjourson, Murray and OʼNeill2017) showed that almost a quarter of students experienced a lifetime major depressive episode, with over a fifth experiencing generalized anxiety disorder. Using DASS, Dooley et al. (Reference Dooley, O’Connor, Fitzgerald and O’Reilly2019) found that 23% of young people (including both students and non-students) were in the severe or very severe category for depression, with 28% in these categories for anxiety. A gender breakdown of the DASS scores showed a higher proportion of females in the severe and very severe anxiety categories relative to males (Dooley et al. Reference Dooley, O’Connor, Fitzgerald and O’Reilly2019). Price & Smith (Reference Price and Smith2019) found severe levels of anxiety in 38.4% of those surveyed, with 29.9% in the severe category for depression and 17.3% for stress. They also found that females and those identifying as nonbinary had the highest reported levels of anxiety, but that males reported higher levels of severe depression than females in the study. Thus, our results are broadly consistent with previous research from Ireland showing a high prevalence of significant psychological distress among higher education students, though we find slightly lower rates of severe and extremely severe depression than some studies (Price & Smith, Reference Price and Smith2019).
In terms of the international literature, studies have employed a range of samples, psychological distress measures, and analysis techniques to consider the relationship between psychological distress and sociodemographic factors. However, there are commonalities between our findings and some international studies. For example, using the Patient Health Questionnaire (PHQ) in a US university, Eisenberg et al. (Reference Eisenberg, Golberstein and Gollust2007) found that while females and males were equally likely to screen positive for depression, females were about twice as likely to screen positive for anxiety. Also using the PHQ, Said et al. (Reference Said, Kypri and Bowman2013) found that a greater proportion of women in a large public university in Australia had depression and anxiety. They also showed that students who identified as homosexual or bisexual, undergraduates, and those experiencing financial difficulty were more likely to experience mental health disorders, which is in line with our findings.
Using the DASS measure, Larcombe et al. (Reference Larcombe, Finch, Sore, Murray, Kentish, Mulder, Lee-Stecum, Baik, Tokatlidis and Williams2016) examined the prevalence and sociodemographic correlates of severe levels of psychological distress among university students in a large metropolitan university in Australia. Looking at particular subgroups, young women and sexual minorities were shown to be at increased risk for anxiety and stress, which again is in line with our findings. Rosenthal et al. (Reference Rosenthal, Russell and Thomson2008) focused on the psychological distress experienced by international students from one university in Australia. While age and gender were not found to be strongly associated with students’ health or risk behaviors, younger international students experienced more psychological distress than older students. Furthermore, a number of other studies from Turkey, Hong Kong, and India have found that age, gender, sexual orientation, and field of study are all associated with psychological distress in students (Bayram & Bilgel, Reference Bayram and Bilgel2008; Wong et al. Reference Wong, Cheung, Chan, Ma and Tang2006; Bhat et al. Reference Bhat, Amaresha, Kodancha, John, Kumar, Aiman, Jain and Cherian2018).
Overall our results have a range of implications for service provision, as well as for future research. First, our findings of statistically significant differences in the prevalence of psychological distress across student groups bolsters the case for more targeted services. As just one example, we show significantly higher rates of distress amongst transgender or gender nonconforming students, as well as amongst gay, lesbian, or bisexual students. This suggests that consideration could be given to prioritized or ring-fenced services and supports for these groups within HEIs. Another example, at a wider sectoral level, relates to significant differences by HEI type. Our results show significantly higher levels of mental ill health amongst students in ITs (now mainly technological universities) when compared to universities, suggesting a need for increased relative investment in the former. Nonetheless, whatever decisions are made in relation to resource allocation, both within and across HEIs, it is important to ascertain the overall effectiveness of this spending in terms of reducing overall levels and disparities in distress. In that regard the results and findings in this paper provide useful baseline information.
Second, our results can be combined with previous evidence to inform decisions relating to the way in which services and supports are delivered. For example, we find that undergraduate students have higher levels of distress relative to postgraduate students and we also find evidence of a very strong socioeconomic gradient in mental ill health. Our previous research using the same data (Walsh et al. Reference Walsh, Cullinan, Flannery and Kennelly2020) showed that undergraduate and less well-off students place a significantly higher value on information provision relating to mental health services and supports. The results in the current paper therefore strengthen the case for greater information provision to both of these groups. Once again, however, it would be useful for future research to evaluate the effectiveness of this approach.
Third, the findings in this paper also provide important and interesting avenues for additional future research. As noted, we have provided evidence of significant differences in psychological distress across student groups. While the existing national and international literature provide some evidence as to why these disparities exist, future research should focus on developing a better understanding in the Irish context. Again, to provide just one example, future research could examine the drivers of differences in prevalence rates across HEIs and/or HEI types, considering factors such as differences in student background, services and supports, commuting patterns, etc.
Our survey was conducted prior to the COVID-19 pandemic. As a result, our findings offer useful baseline estimates of psychological distress that could inform future studies on its impact on student mental health in Ireland. The full effects of the pandemic on societal mental health is expected to be severe and enduring, leading to increases in prevalence rates and likely exacerbating existing disparities (Gavin et al. Reference Gavin, Lyne and McNicholas2020; Power et al. Reference Power, Hughes, Cotter and Cannon2020). In the higher education context, the rapid change in the normal student experience, reduction and change in the services available for people experiencing mental health difficulties, increased worry about future career prospects, limits placed on social interaction, and reduction or elimination of typical health producing activities are just some of the factors that have affected the mental health of university students during the pandemic. In a study conducted early in the pandemic, USI (2020) found that over a third (33.9%) of students felt that their mental health was worse as a result of COVID-19.
There is also a range of other evidence relating to the impact of the pandemic on the mental health of young people more generally. For example, a recent study by the Central Statistics Office on the social impact of the COVID-19 pandemic found that younger people are much more likely to report low levels of mental health and emotional well-being than older groups. It showed that 74% of people in the 18–34 age group surveyed in February 2021 said that their mental health had been affected negatively by the pandemic, which was the highest proportion of any age group (CSO 2021). Furthermore, 21% of the 18–34 age group reported that they were depressed or downhearted all or most of the time. In a noteworthy study, Murray et al. (Reference Murray, McClintock, McNamara, OʼMahony, Smyth and Watson2021) conducted a special round of the Growing up in Ireland (GUI) longitudinal study in December 2020. Using a sample of over 2000 22-year-olds, they found that almost half (48%) had elevated scores on the CES-D 8 measure of depressive symptoms. This compared with 27% with elevated scores (using the same measure and cutoff point) two years previously, when respondents were aged 20. Interestingly, 55% of female respondents had elevated scores for depressive symptoms compared to 41% of males.
A large number of international studies report similar findings. For instance, Banks et al. (Reference Banks, Fancourt, Xu, Helliwell, Layard, Sachs and De Neve2021) state that the pandemic has been associated with a substantial rise in mental ill health. Data from representative cohort studies across the world showed increases in average scores of psychological distress and a rise in the share of people experiencing clinically significant levels of mental illness in the first few weeks of lockdown, compared to data collected prior to the pandemic (Banks et al. Reference Banks, Fancourt, Xu, Helliwell, Layard, Sachs and De Neve2021). Using sophisticated modeling techniques to take account of underlying trends in mental ill health before the pandemic in the UK, Banks & Xu (Reference Banks and Xu2020) found that the General Health Questionnaire (GHQ) scores of young people aged 18–34 were particularly affected in the initial stages of the pandemic. Data collected around 6 months after the pandemic started showed a slightly different picture with young women no longer showing particularly large reductions in their GHQ scores. Thus, overall it seems likely that the pandemic will lead to increases in the prevalence rates of mental ill health amongst higher education students at an overall level and may have exacerbated already existing disparities.
As with many other national and international studies examining the prevalence of psychological distress amongst higher education students, a number of caveats and limitations should be borne in mind when considering our analysis and findings. The data used is observational in nature with students self-selecting to complete the online survey, which could have introduced selection bias. In addition, the data does not cover all HEIs in Ireland. We also dropped some observations due to short survey completion times and missing data on some key variables. Taken together, these points raise issues in relation to the representativeness of our results. Strengths of the study include the relatively large sample size and the robustness checks undertaken, including the reweighting of our data. However, given the study limitations, in particular the potential for selection bias, further mental health research is needed in this population which will inform necessary resourcing for mental health service delivery in higher education students.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/ipm.2022.2
Acknowledgments
We thank the students and HEIs that participated in this research project.
Author contributions
JC conceived and designed the study, performed the analysis, and led the write-up of the original and revised manuscript. SW designed the survey questionnaire, gathered the data, performed the literature review, and helped undertake the analysis and write parts of the manuscript. DF inputted to the design of the survey questionnaire and helped develop the methodology, interpret the findings, and write the manuscript. BK inputted to the design of the survey questionnaire and helped interpret the findings and write the manuscript.
Financial support
This work was supported by an Irish Research Council (IRC) Research for Policy and Society award to John Cullinan for the project ‘Student Preferences for Mental Health Services in Irish Higher Education Institutions: A Discrete Choice Experiment’ (RfPS/2016/25).
Conflict of interest
The authors declare no conflicts of interest.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation with the Helsinki Declaration of 1975, as revised in 2008. Ethical approval for the study was granted by the NUI Galway Research Ethics Committee. Informed consent was obtained from all participants included in the study.
Role of the Funder/Sponsor
The funders had no role in the design of the study; the collection, analysis, and interpretation of data; the writing of the paper; or the decision to submit the paper for publication.







 Open access
Open access