



Specific Event Identifiers
Event Type: Mega Mass-Casualty Terrorist Attack
Event Onset Date: October 7, 2023
Location of Event: Southern Israel bordering Gaza including between Zikim, Sderot, Netivot, and Kerem Shalom
Geographic Coordinates: 31°36'35.4''N 34°31'15.4''E 28m; 31°31'22.1''N 34°35'44.1''E 95 m; 31°25'24.2''N 34°35'42.1''E 154 m; 31°13'44.3''N 34°17'03.6''E 88m
Dates of Observation Reported: October 7-8, 2023
Response Type: Prehospital Ambulance Service
Introduction
A mass-casualty event (MCE) presents challenges whether it occurs in a rural or densely populated area. Reference Bloch, Schwartz and Pinkert1 Considerations taken when evacuating victims from the scene include the receiving capacity of the hospitals that are close to the incident, hospital staff capabilities, and the condition of the victims. An MCE that occurs in a rural area can lead to a hospital receiving a large number of casualties that it is unable to handle. Reference Adini, Cohen and Glassberg2 In such cases, secondary transfer of casualties to more distant hospitals is necessary after initial triage is performed at the nearest hospital. Reference Schwartz, Pinkert and Leiba3 A multi-theater MCE is such as occurred in Madrid, Spain on March 11, 2004 when bombs detonated on four separate commuter trains and immediately killed 177 and injured more than 2,000. At the closest receiving hospital, 312 victims were treated without any secondary transfer. One of the lessons was that there was probably over-triage to this hospital to save ambulance response time. Reference Gutierrez de Ceballos, Turégano Fuentes, Perez Diaz, Sanz Sanchez, Martin Llorente and Guerrero Sanz4
Magen David Adom (MDA; Tel Aviv, Israel) is Israel’s National Emergency Pre-Hospital Medical Organization and a member of the International Committee of the Red Cross (Geneva, Switzerland). It operates 169 primary stations and dispatching points in 11 geographical regions. Assets include 1,000 Basic Life Support (BLS) ambulances, 450 Advanced Life Support (ALS) ambulances, 650 motorcycles, three helicopters, and one national command and control truck. Responders from MDA include 2,600 salaried employees (1,000 of which are paramedics and the rest are emergency medical technicians [EMTs]) and 30,000 volunteers (mostly EMTs). There are also 9,500 on-call volunteer first responders who are dispatched through a location-based application and provide initial medical assistance until the arrival of ambulances. All MDA salaried employees and volunteers are trained in mass-casualty response. The MDA ambulances transport patients to one of the 29 emergency departments in Israel, which has a population of 9.8 million. Of these, seven are Level 1 Trauma Centers.
Narrative
At 06:30 on October 7, 2023, a massive missile attack began from Gaza against the Israeli population in southern and central Israel. That morning, approximately 400 ambulance crews were working across the country, and around 15 of them were operating in the area of the attack. When the missile attack began, MDA raised its alert, and within half-an-hour, the number of teams doubled from 400 to 960. Using the missile attack as cover, 3,000 Hamas terrorists invaded from Gaza, shooting at every person in their path, blowing up vehicles and homes, and setting them on fire. Weapons included Kalashnikov automatic rifles and rocket-propelled grenades. The area of this mega terrorist attack is rural with over 25 kibbutzim (communal settlements) and villages, and three cities with a total population of around 100,000. Thousands of calls regarding gunshot victims from the area under attack by Hamas terrorists were received by MDA, with the first one coming in at 06:59. As attacks on civilians grew, so did the number of emergency calls. Many of the wounded suffered from high-velocity bullet wounds, shrapnel injuries, and burns. In addition to civilians, three MDA personnel – one ambulance driver, one paramedic, and one on-call volunteer first responder – were killed. Seven MDA ambulances were intentionally shot and one was burnt, rendering them useless. Approximately 1,200 people were killed in this attack, 239 were taken as hostages, and 1,455 were injured. 5,6 The nature of the injuries required large numbers of ambulances to transport severely injured and dying patients to nearby hospitals. The two hospitals closest to the area are Barzilai Medical Center (BMC) in Ashkelon (20-30km), a Level 2 Trauma Center to the north with 560 beds, and Soroka Medical Center (SMC) in Beer Sheba (30-50km), a Level 1 Trauma Center with 1,123 beds. Due to the fighting, many roads were closed, extending travel and limiting initial regulation between hospitals.
Victims began arriving at SMC at 07:30 and at BMC at 09:00. By 09:00, all MDA ambulances in the organization were manned. During the day, these two hospitals received 650 and 372 casualties, respectively. There were at least 600 patients transferred directly from the scene by MDA to the other hospitals in Israel. Besides MDA, other victims were brought by military helicopters, other ambulance services, or private vehicles.
Because of the overwhelming number of victims taken to SMC and BMC, it became necessary to implement a strategy of secondary transfer. Over a 12-hour period on October 7, 2023, there was a total of 64 patients transferred. The first transfer began from BMC at 12:20, whereas only at 15:37 from SMC, with both hospitals transferring patients until close to midnight (Figure 1). A total of 38 patients from BMC and 26 patients from SMC were secondarily transferred. Fourteen hospitals received patients from the two transferring hospitals; the closest transfer was from BMC to Sheba, Tel-HaShomer Medical Center in Ramat Gan (57km), and the furthest transfer was from SMC to Carmel Medical Center in Haifa (194km). Overall, 16 were transported by ALS ambulance, 34 emergently by a BLS ambulance, and 14 non-emergently by a BLS ambulance (Table 1; Figure 2).
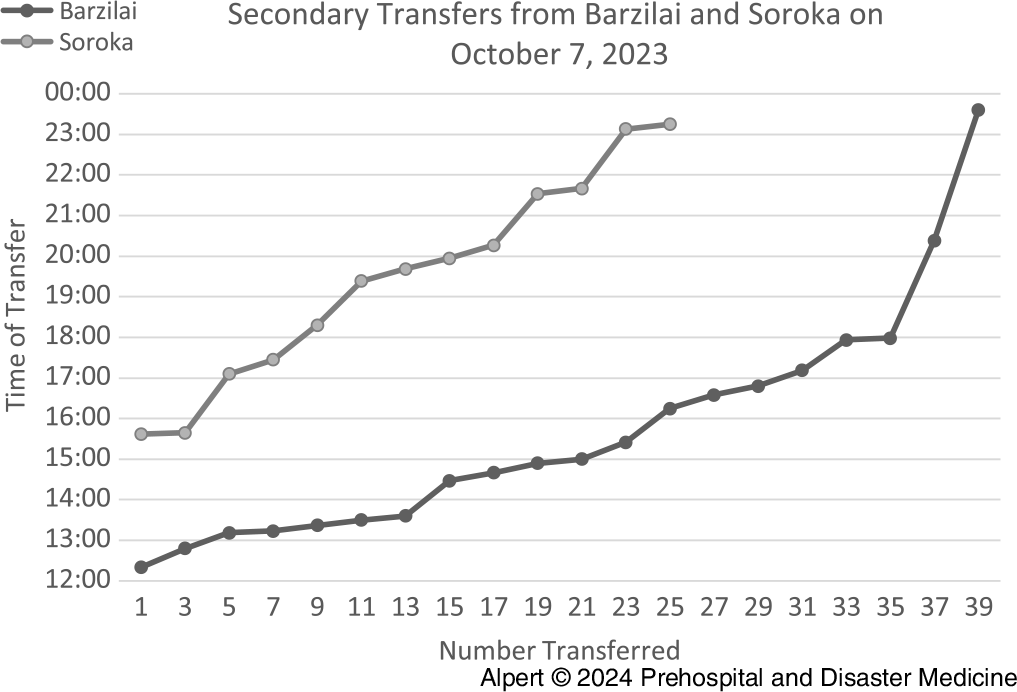
Figure 1. Secondary Transfers Performed by MDA Over a 12-Hour Period on October 7, 2023.
Note: The grey line indicates the transfers from Soroka Medical Center (SMC) and the black line indicates the transfers from Barzilai Medical Center (BMC). There was a total of 64 patients transferred: 38 patients were transferred from Barzilai Medical Center and 26 from Soroka Medical Center.
Abbreviation: MDA, Magen David Adom.
Table 1. Secondary Transfers by MDA of Patients from Barzilai Medical Center (BMC) and Soroka Medical Center (SMC), Including Receiving Hospital, Triage Status, and Distance Between Hospitals Based on Google Maps
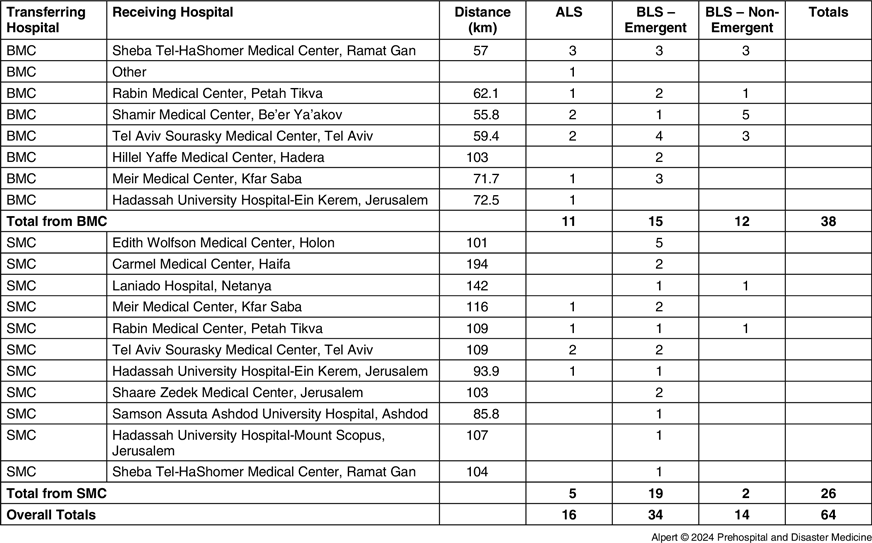
Abbreviations: ALS, Advanced Life Support; BLS, Basic Life Support; BMC, Barzilai Medical Center; SMC, Soroka Medical Center; MDA, Magen David Adom.
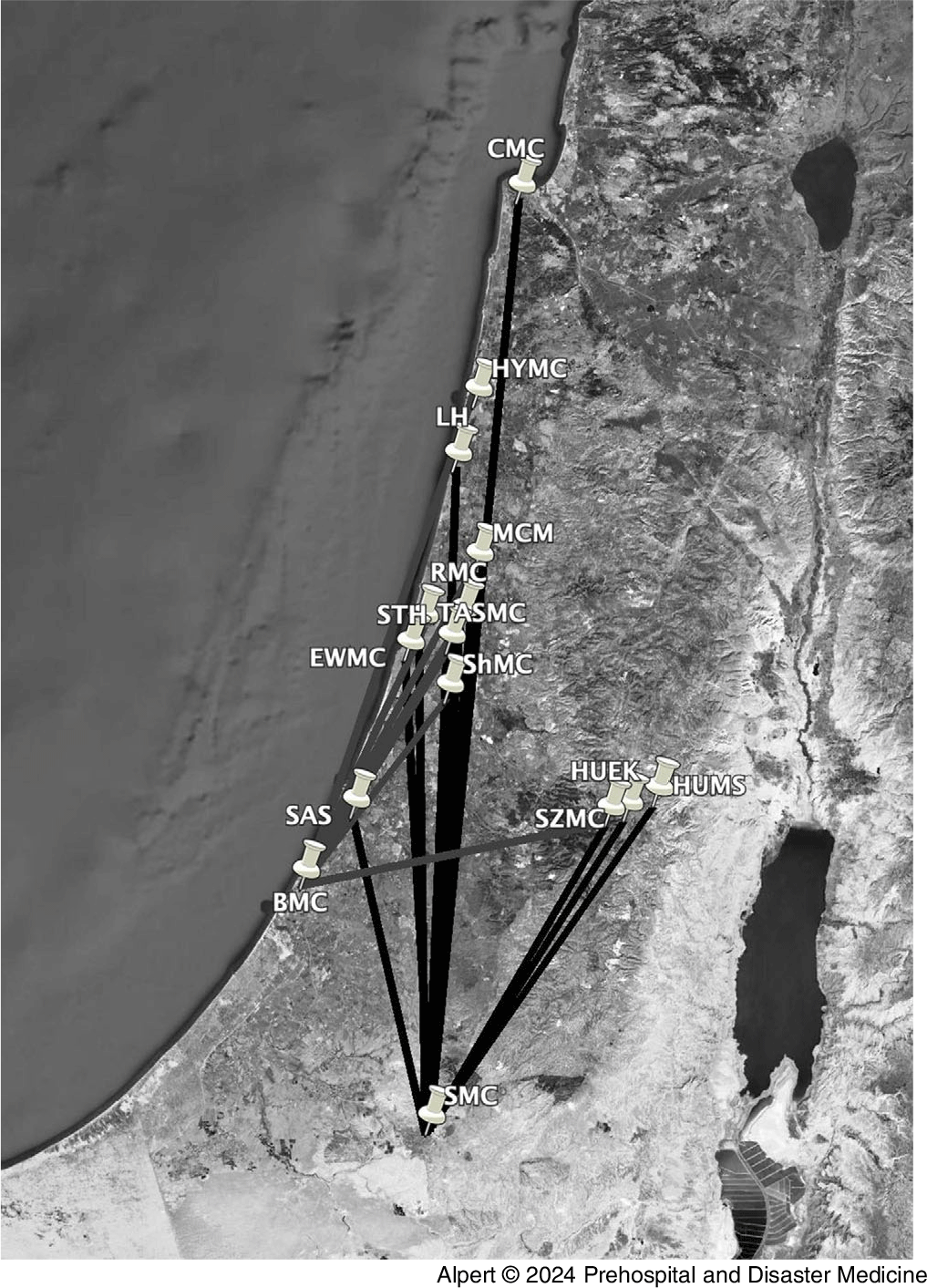
Figure 2. Map Based on Google Earth Depicting the Secondary Transfers from Soroka Medical Center (SMC) and Barzilai Medical Center (BMC) on October 7, 2023.
Abbreviations: BMC, Barzilai Medical Center; SMC, Soroka Medical Center; STH, Sheba Tel HaShomer Medical Center; RMC, Rabin Medical Center; ShMC, Shmair Medical Center; TASMC, Tel Aviv Sourasky Medical Center; HYMC, Hillel Yaffe Medical Center; MCM, Meir Medical Center; HUEK, Hadassah University Hospital-Ein Kerem; EWMC, Edith Wolfson Medical Center; CMC, Carmel Medical Center; LH, Laniado Hospital; SZMC, Shaare Zedek Medical Center; HUMS, Hadassah University Hospital Mount Scopus; SAS, Samson Assuta Ashdod University Hospital.
Discussion
Israel unfortunately has had years of experience with MCEs due to terror which includes suicide bombing, stabbings, and vehicle rammings. Reference Almogy, Belzberg, Mintz, Pikarsky, Zamir and Rivkind7–Reference Tsur, Nadler and Sorkin9 Israel defines a mega terrorist attack whereby there are more than 500 victims. Until now, this has been theoretical rather than reality. Reference Leiba, Blumenfeld and Hourvitz10 Any MCE presents multiple challenges, particularly with the treatment of patients at the scene, and a mega terrorist attack even more so. The concept of a triage or evacuation hospital is whereby only the most emergent patients are treated at the closest hospital and all others are transferred. Reference Klausner and Rozin11 Actual studies describing secondary transfers are quite sparse. In 2009, a Turkish airline crashed near Amsterdam resulting in 126 surviving casualties. Only three were secondarily transferred – all from either Level 2 or Level 3 Trauma Centers to a Level 1 Trauma Center. Reference Postma, Weel and Heetveld12 In Israel in 2005, a suicide bomber detonated explosives outside a major metropolitan area in Israel. Four victims died at the scene and a total of 58 wounded were evacuated. Two with significant head injuries were secondarily evacuated from the local Level 2 Trauma Center to a more distant Level 1 Trauma Center – one by helicopter and one by ambulance. Reference Schwartz, Pinkert and Leiba3 In a study of 33 mass-casualty terror attacks in Israel from 2000-2002, out of 1,156 injured patients, only 27 underwent secondary transfer within two hours to a different facility. Most of these were from a lower-level facility to a trauma center. Reference Einav, Feigenberg and Weissman13
The prehospital response to the MCE from October 7, 2023 is unique in a few aspects. It was the first mega terrorist attack in Israel’s history – resulting in combat-type injuries in a civilian population. The secondary transfers may have occurred first from BMC as it is a smaller hospital and a Level 2 Trauma Center as opposed to SMC which is much larger and a Level 1 trauma facility. It should be noted that because of the overwhelming numbers of injuries, even those that were less severe were secondarily transferred to other centers. Another unique aspect is that the secondary transfers were carried out while the MCE was on-going – including continuous missile fire at Israel and terrorists who were still active. It should be noted that there was no lack of ambulances, and that throughout the MCE, vehicles from regions throughout the country participated. One critique of the emergency management on October 7, 2023 is that even more patients should have been secondarily transferred.
By providing a post-hoc analysis of a mega MCE, one can incorporate lessons to provide better care in future events. These lessons include the earlier implementation of secondary transfers and the importance of conducting secondary transfers even from a Level 1 Trauma Center when the sheer number of victims overwhelms the system.
Conflicts of interest
There are no conflicts of interest.




 Open access
Open access