
Contents
Poster Presentation - Top Poster Award
Other
Overview of infection control in nursing research in Korea over the last 10 years: Text network analysis and topic modeling
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s14-s15
-
- Article
-
- You have access
- Open access
- Export citation
-
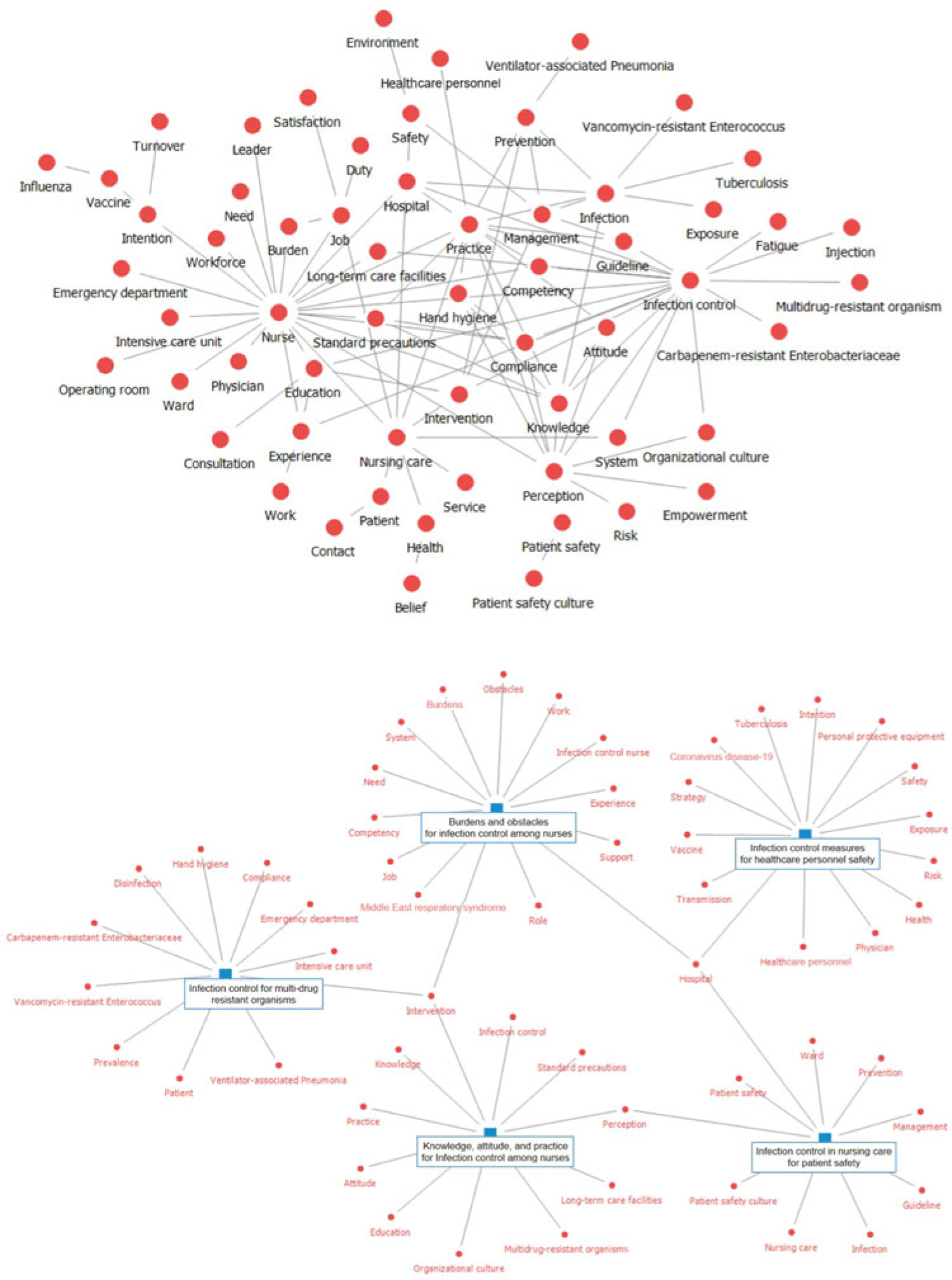
Background: With the emergence of new infectious diseases, infection control nursing (ICN) in hospitals has become increasingly significant. Consequently, research on ICN has been actively performed. We examined the knowledge structure and trends addressed in Korean ICN research. Methods: From 5 web-based Korean academic databases (DBpia, KISS, KMbase, KoreaMed, and RISS), 2,244 studies published between 2013 and 2022 were retrieved using ICN-related search terms (eg, “nurse” or “nursing” along with “infection control,” “infection prevention,” “healthcare-associated infection,” or “standard precautions”). After deleting duplicates, the authors assessed titles and abstracts and included 250 research abstracts in this study. Using NetMiner 4.4 software (Cyram, Seoul, Korea), words from abstracts of published articles were extracted and refined, then text network analysis and topic modeling were performed. A text network was structured based on the co-occurrence matrix of key words (semantic morphemes) and was analyzed to identify the main key words. Through topic modeling using the Latent Dirichlet Allocation algorithm, latent topics in the research abstracts were extracted. The authors verified the key words comprising the topic and the result of classifying the documents by topic and named topics. Results: The number of studies, which increased following the outbreak of Middle East respiratory syndrome in 2015, has declined over time but peaked in 2021 with the COVID-19 pandemic. The text network composed of the key words of the research abstracts was generated and visualized (Fig. 1). As a result of text network analysis, the 5 most common key words were ‘nurse,’ ‘infection control,’ ‘nursing care,’ ‘practice,’ and ‘perception’ in terms of degree and betweenness centrality. Other prominent main keywords were also identified: ‘knowledge,’ ‘compliance,’ ‘education,’ ‘intervention,’ ‘intention,’ and ‘safety.’ With the application of topic modeling to the research abstracts, 5 topics were derived and named as follows (Fig. 2): “infection control in nursing care for patient safety,” “infection control measures for healthcare personnel safety,” “burdens and obstacles for infection control among nurses,” “infection control for multidrug-resistant organisms,” and “knowledge, attitude, practice for infection control among nurses.” Conclusions: By applying text-network analysis and topic modeling, we obtained insights into Korean ICN research trends. To explore global ICN research trends, further study is necessary to analyze internationally published studies reflecting each country’s nursing work conditions.
Disclosure: None

Screening infection prevention policies for equity impacts
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s15
-
- Article
-
- You have access
- Open access
- Export citation
Outbreaks
Mycobacterium chimaera infections in cardiothoracic surgery patients exposed to heating and cooling devices despite infection control measures
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s15-s16
-
- Article
-
- You have access
- Open access
- Export citation
-
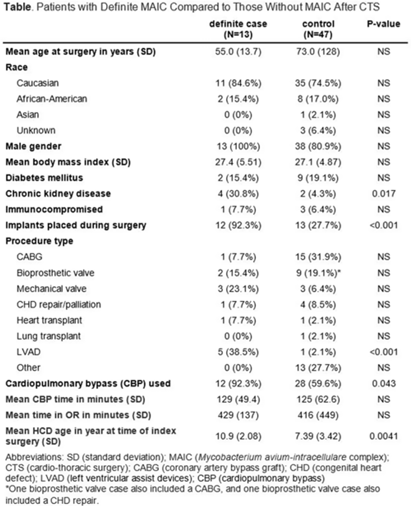
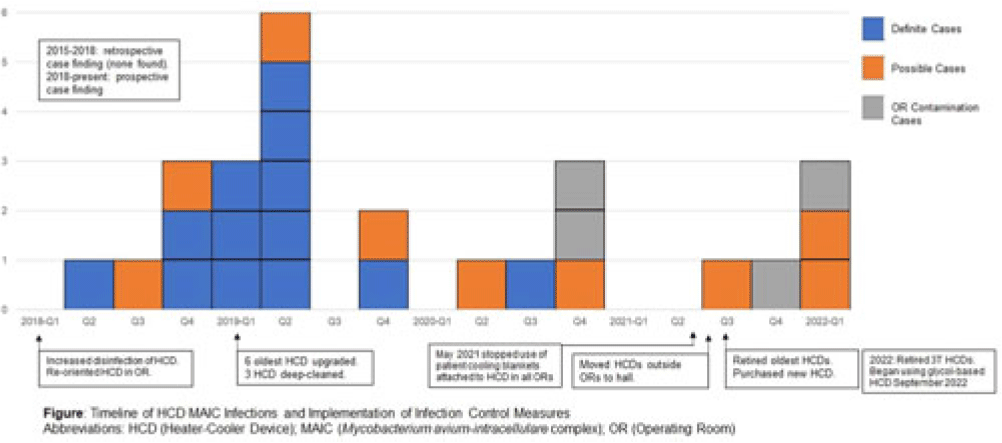
Background: LivaNova 3T heating and cooling devices (HCDs) have been associated with Mycobacterium chimaera, a Mycobacterium avium-intracellulare (MAIC) species, infections after cardiothoracic surgery. We describe our outbreak, which persisted despite escalating infection control measures. Methods: We identified patients with a positive MAIC culture following cardiothoracic surgery from January 2015 to the present at our institution. We classified these as “definite,” “possible,” or “operating room contamination” cases based on positive cultures from sterile sites, airway, or surgical specimens without evidence of infection. To identify patient or surgery characteristics associated with risk for MAIC infection, we conducted a case–control study comparing definite cases to randomly selected unmatched controls of patients over the same period without a positive MAIC culture after cardiothoracic surgery. Results: We identified 26 patients with a positive MAIC culture after cardiothoracic surgery: 13 definite, 9 possible, and 4 contamination cases. Among definite cases, the most common surgeries were valve replacements and left ventricular assist devices (5 cases each). The mean time from cardiothoracic surgery to diagnosis was 525 days. Overall, 10 (77%) cases occurred after exposure to our oldest HCDs (manufactured in 2013 or earlier). To date, 16 (62%) have undergone or are undergoing treatment for MAIC infection, and 4 (15%) have died due to NTM infection or complications. Compared to 47 controls, definite cases were associated with chronic kidney disease, implants, procedure type, use of cardiopulmonary bypass, and HCD age. Cases were not associated with time on bypass, time in the operating room, or other comorbid conditions (Table). All cases occurred despite enhanced disinfection and reorienting the HCD within the operating room, according to manufacturer recommendations. Moreover, 18 cases, including 7 definite cases, occurred after most HCDs were either deep cleaned or upgraded by the manufacturer. Also, 5 cases, including 3 possible cases and 2 contamination cases, occurred after physical separation of the HCD from the operating room. In August 2022, we purchased a fleet of glycol-cooled HCDs, and we have not identified additional MAIC cases since their deployment (Fig.). Conclusions: MAIC infections after cardiothoracic surgery were associated with procedure type, especially implants, use of cardiopulmonary bypass, and HCD age. Contrary to prior reports, neither operative nor CPB time was associated with MAIC infection after cardiothoracic surgery. The outbreak persisted despite disinfection and/or deep cleaning and reorienting HCDs within the operating room; some possible and contamination cases occurred even after moving HCDs outside the operating room. Thus, HCD water contamination events in the operating room (eg, spills from HCD tubing) may be a route of exposure, and different infection prevention measures are needed.
Disclosure: None


Pediatrics
Epidemiology of carbapenem-resistant and extended-spectrum beta-lactamase-producing Enterobacterales in US children, 2016–2020
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s16
-
- Article
-
- You have access
- Open access
- Export citation
Product Evaluation
Evaluation of four environmental sampling methods for the recovery of multidrug-resistant organisms
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s16-s17
-
- Article
-
- You have access
- Open access
- Export citation
-
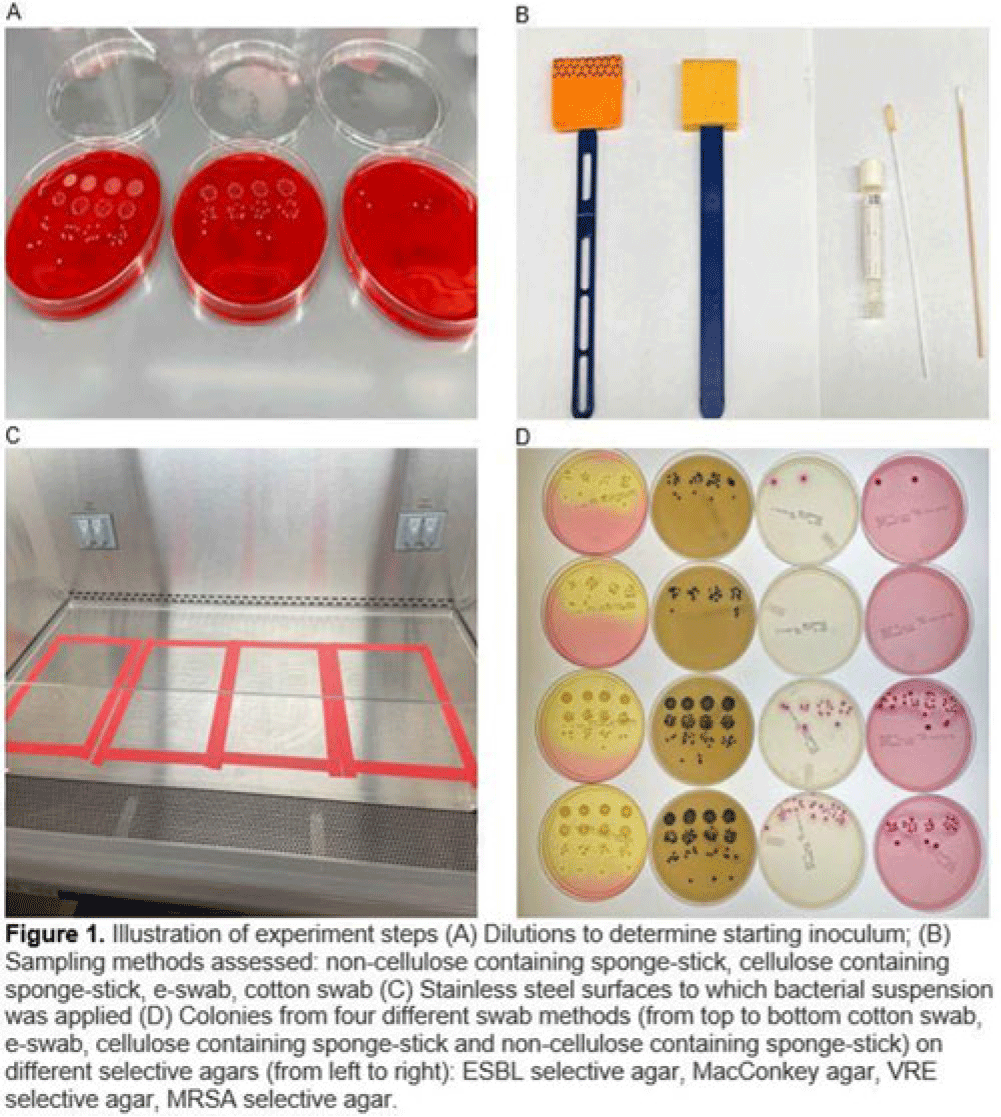
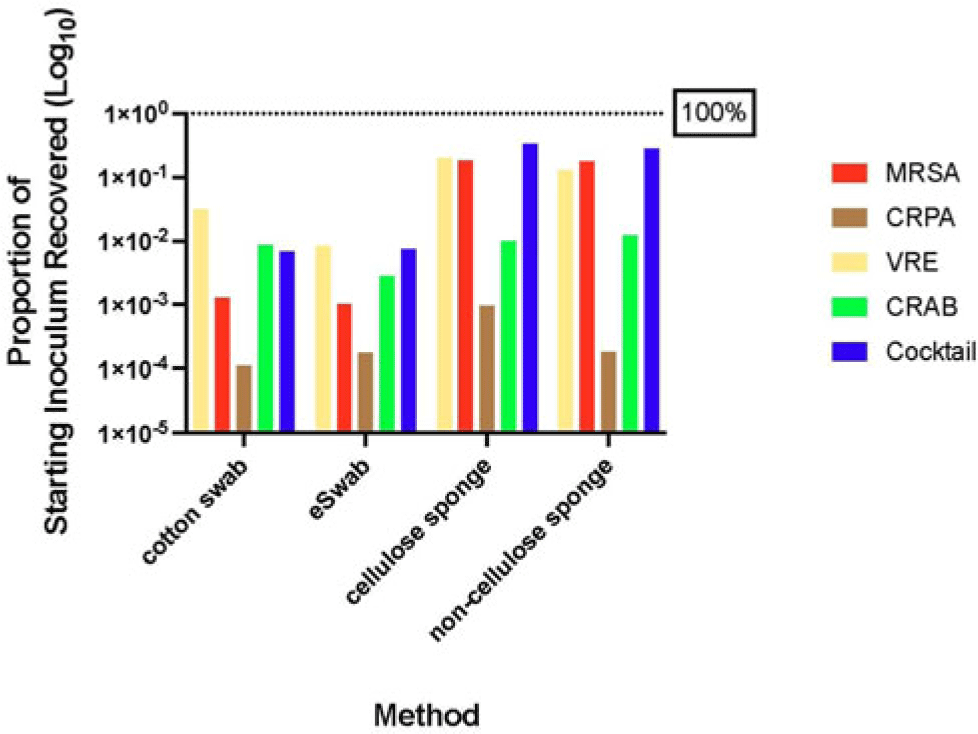
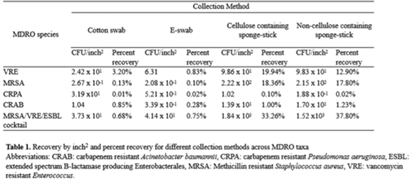
Background: Environmental contamination is a major risk factor for multidrug-resistant organism (MDRO) exposure and transmission in the healthcare setting. Sponge-stick sampling methods have been developed and validated for MDRO epidemiological investigations, leading to their recommendation by public health agencies. However, similar bacteriological yields with more readily available methods that require less processing time or specialized equipment have also been reported. We compared the ability of 4 sampling methods to recover a variety of MDRO taxa from a simulated contaminated surface. Methods: We assessed the ability of (1) cotton swabs moistened with phosphate buffer solution (PBS), (2) e-swabs moistened with e-swab solution, (3) cellulose-containing sponge sticks (CSS), and (4) non–cellulose-containing sponge sticks (NCS) to recover extended-spectrum β-lactamase (ESBL)–producing Escherichia coli, carbapenem-resistant Pseudomonas aeruginosa (CRPA), carbapenem-resistant Acinetobacter baumannii (CRAB), methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus faecium (VRE), and a mixture that contained VRE, MRSA, and ESBL organisms. A solution of known bacterial inoculum (~105 CFU/mL) was made for each MDRO. Then, 1 mL solution was pipetted on a stainless-steel surface (8 × 12 inch) in 5 µL dots and allowed to dry for 1 hour. All samples were collected by 1 individual to minimize variation in technique. Sponge sticks were expressed in PBS containing 0.02% Tween 80 using a stomacher, were centrifuged, and were then resuspended in PBS. Cotton and e-swabs were spun in a vortexer. Then, 1 mL of fluid from each method was plated to selective and nonselective media in duplicate and incubated at 35°C for 24 hours (MRSA plates, 48 hours) (Fig. 1). CFU per square inch and percentage recovery were calculated. Results: Table 1 shows the CFU per square inch and percentage recovery for each sampling method–MDRO taxa combination. The percentage recovery varied across MDRO taxa. Across all methods, the lowest rate of recovery was for CRPA and the highest was for VRE. Regardless of MDRO taxa, the percentage recovery was highest for the sponge stick (CSS and NCS) compared to swab (cotton and E-swab) methods across all taxa (Table 1 and Fig. 2).
Conclusions: These findings support the preferential use of sponge sticks for the recovery of MDROs from the healthcare environment, despite the additional processing and equipment time needed for sponge sticks. Further studies are needed to assess the robustness of these findings in noncontrived specimens as well as the comparative effectiveness of different sampling methods for non–culture-based MDRO detection.
Disclosure: None



SSI
The effectiveness of the appropriate prophylactic antibiotic use program for surgery
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s17-s18
-
- Article
-
- You have access
- Open access
- Export citation
-
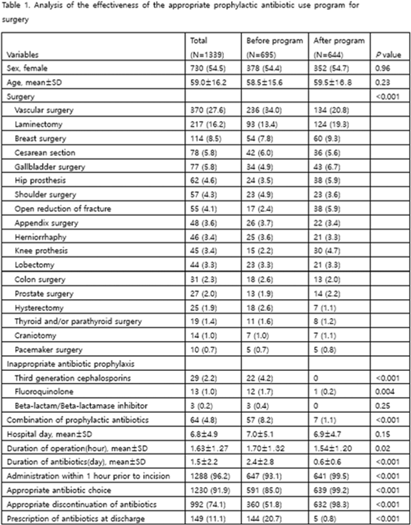
Background: Evaluation of the adequacy of prophylactic antibiotics in surgery has been implemented as a national policy in Korea since August 2007, and the appropriate use of prophylactic antibiotics has improved. However, antibiotic prescriptions that are not recommended or discontinuation of prophylactic antibiotic administration within 24 hours after surgery are still not well done. This study introduced a program to improve the adequacy of prophylactic antibiotics for surgery and analyzed its effects. Methods: We retrospectively analyzed the effectiveness of the appropriate prophylactic antibiotic use program for surgery conducted at a university hospital in Seoul. The participants were patients aged ≥18 years who underwent any of 18 types of surgery. The program started was implemented in June 2020. First, a computer system was used to confirm the antibiotic prescription recommended for each surgery. It also assessed whether the number of days of administration was exceeded, whether antibiotics were prescribed in combination, and whether antibiotics prescribed for discharge medicine were checked in 4 steps. A pop-up window appeared in each patient record to enter the reason for the prescription. If the reason was appropriate, the prescription was allowed, but if not, the prescription was restricted. In addition, infectious diseases physicians and an insurance review team visited each department to conduct an education session. To analyze the effect 3 months before activity (January–March 2020) and 3 months after activity (October–December 2020), we compared the first antibiotic administration rate within 1 hour prior to skin incision, the recommended prophylactic antibiotic administration rate, and surgery type. The rate of discontinuation of prophylactic antibiotics within 24 hours after administration and the rate of prescription of prophylactic antibiotics at discharge were compared. Results: In total, 1,339 surgeries during the study period were included in the analysis. There were 695 cases before the introduction of the program and 644 cases after the introduction. The rate of first antibiotic use within 1 hour prior to skin incision was 93.1%–99.5% (P < .001), the rate of recommended prophylactic antibiotic administration was 85.0%–99.2% (P < .001), and the rate of discontinuation of antibiotic administration within 24 hours after surgery improved from 51.8% to 98.3% (P < .001), respectively. The prescription rate of antibiotics at discharge improved from 20.7% to 0.8% (P <.001) (Table 1). Conclusions: A computerized program to improve the adequacy of prophylactic antibiotic use in surgery combined with education of medical staff was very effective.
Disclosure: None

Surveillance/Public Health
Modeling the impacts of influenza antiviral prophylaxis strategies in nursing homes
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s18-s19
-
- Article
-
- You have access
- Open access
- Export citation
-
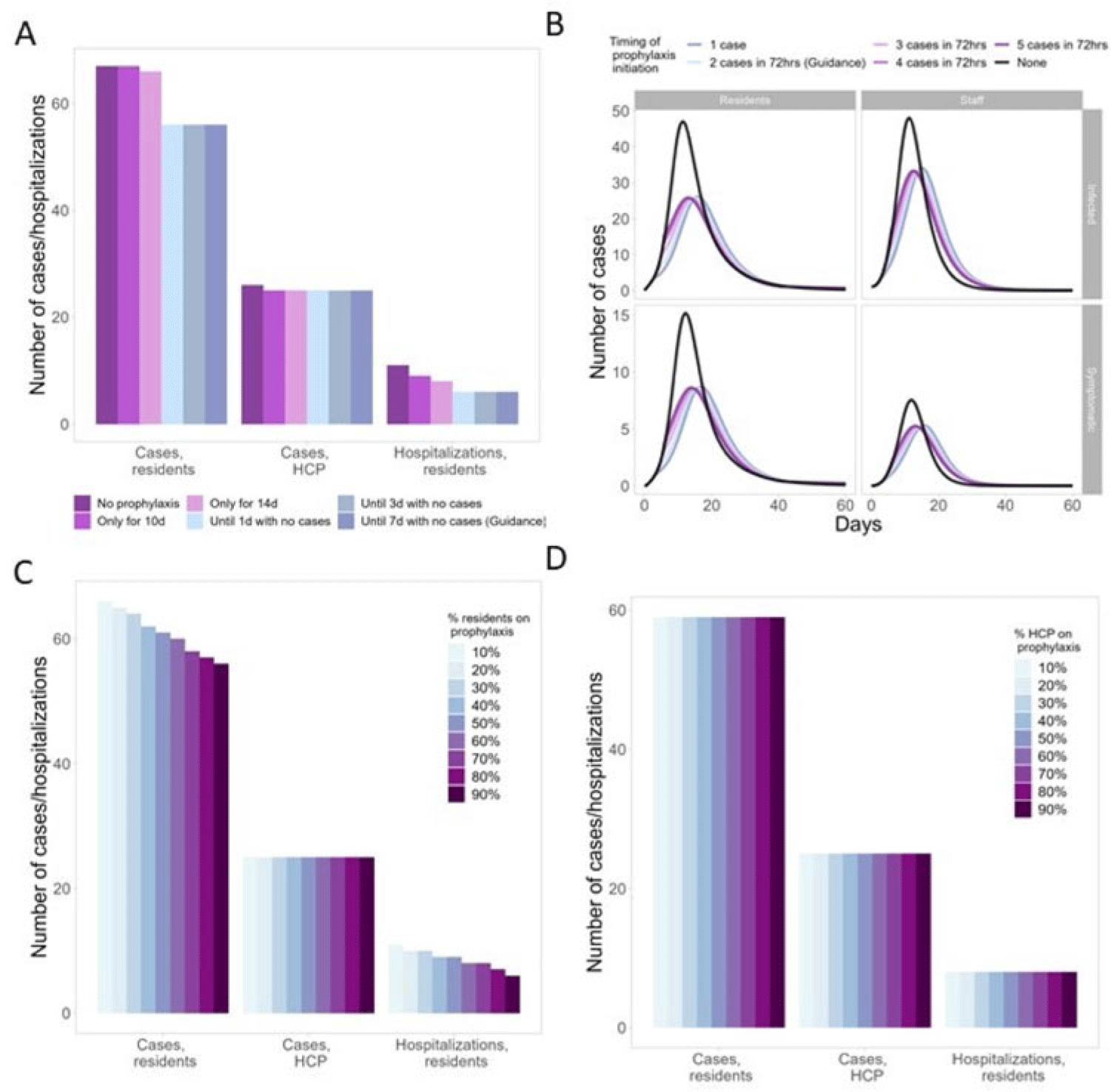
Background: Antiviral chemoprophylaxis for influenza is recommended in nursing homes to prevent transmission and severe disease among residents with higher risk of severe influenza complications. Interim CDC guidance recommends that long-term care facilities initiate antiviral chemoprophylaxis with oral oseltamivir for all non-ill residents living in the same unit following the start of an outbreak in a facility (ie, ≥2 patients ill within 72 hours and of whom at least 1 resident has laboratory-confirmed influenza). Prophylaxis continues for a minimum of 2 weeks and for at least 7 days after the last laboratory-confirmed case. However, facilities may not strictly adhere to this guidance, with 1 study showing up to 68% of facilities were nonadherent to national guidance (Silva et al 2020). Here, we model the potential impacts of different antiviral prophylaxis strategies. Methods: We developed a susceptible–exposed–asymptomatic–infected–recovered (SEAIR) compartmental model of an average-sized nursing home comprising short-stay residents, long-stay residents, and healthcare personnel (HCP). Persons treated with antiviral chemoprophylaxis were less susceptible to infection, had a lower probability of symptoms if infected, a reduced viral load, and a shortened duration of infectiousness. We included influenza vaccination for residents and HCP through reduced probability of symptomatic infection. Coverage rates were estimated from CDC FluVaxView and CMS COVID-19 nursing home data. As a base case, we modeled a scenario with prophylaxis implemented according to guidance. We varied uptake by residents and HCP (from 10% to 90%), case thresholds for prophylaxis initiation (1–5 cases identified), and timing of prophylaxis cessation: either time dependent (ie, 10–14 days of prophylaxis) or case-dependent (ie, continuing prophylaxis for 1–7 days with no cases). Results: In the scenario based on current guidance, prophylaxis reduced resident cases by 16% and resident hospitalizations by 45%, compared to no prophylaxis (Fig. 1A). Scenarios that differed from the guidance altered case burden and timing: Time-dependent prophylaxis cessation increased resident cases and hospitalizations (Fig. 1A). Timing of prophylaxis initiation had slight effects on the timing of the epidemic and minimal effects on resident cases and hospitalizations (Fig. 1B). High resident uptake was important for reducing resident cases and hospitalizations (Fig. 1C), but increasing HCP uptake had minimal effect (Fig. 1D). Conclusions: Our findings support the current prophylaxis guidance. Promptly implementing prophylaxis reduces resident cases and hospitalizations. Continuing prophylaxis until cases are no longer identified reduces cases and hospitalizations.
Disclosure: None

Detection of carbapenem-resistant Enterobacterales from nursing home wastewater effluent from September 2021 to November 2021
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s19
-
- Article
-
- You have access
- Open access
- Export citation
VAE
A national survey of PICU clinician practices and perceptions about respiratory cultures for invasively ventilated patients
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s19
-
- Article
-
- You have access
- Open access
- Export citation
Poster Presentation - Top Oral Abstract
Antibiotic Stewardship
Perspectives on nonprescription antibiotic use among Hispanic patients in the Houston metroplex: A qualitative study
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s20
-
- Article
-
- You have access
- Open access
- Export citation
-
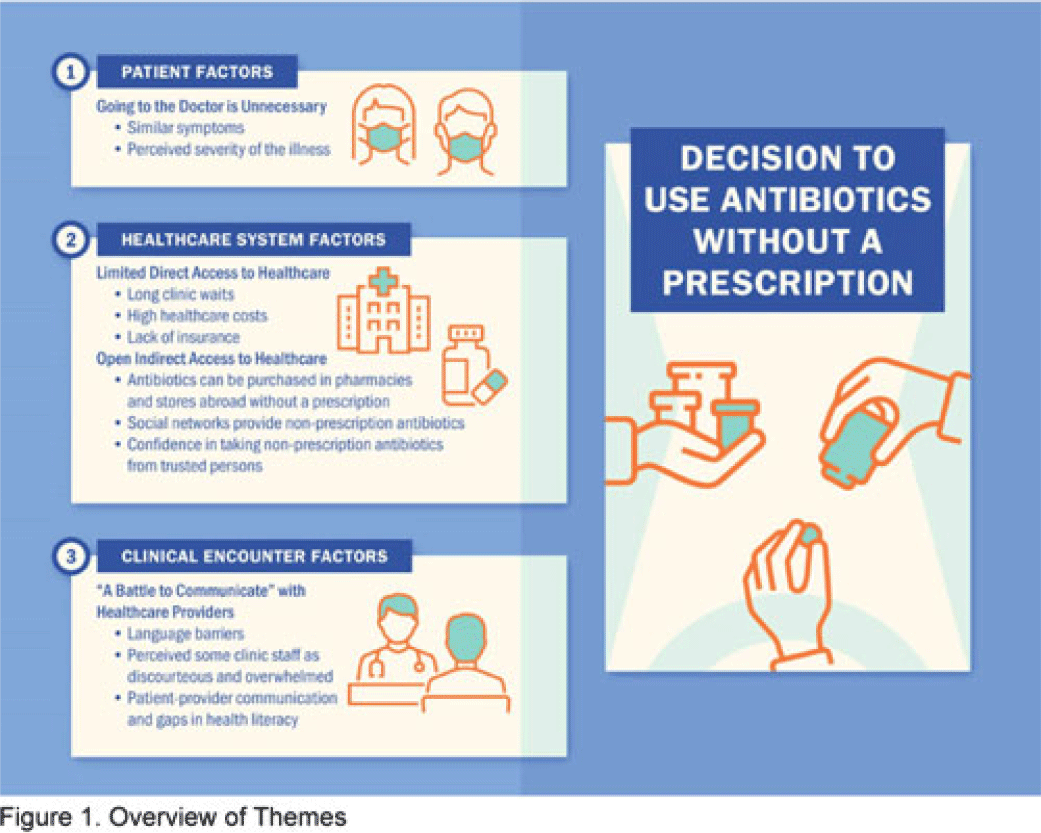
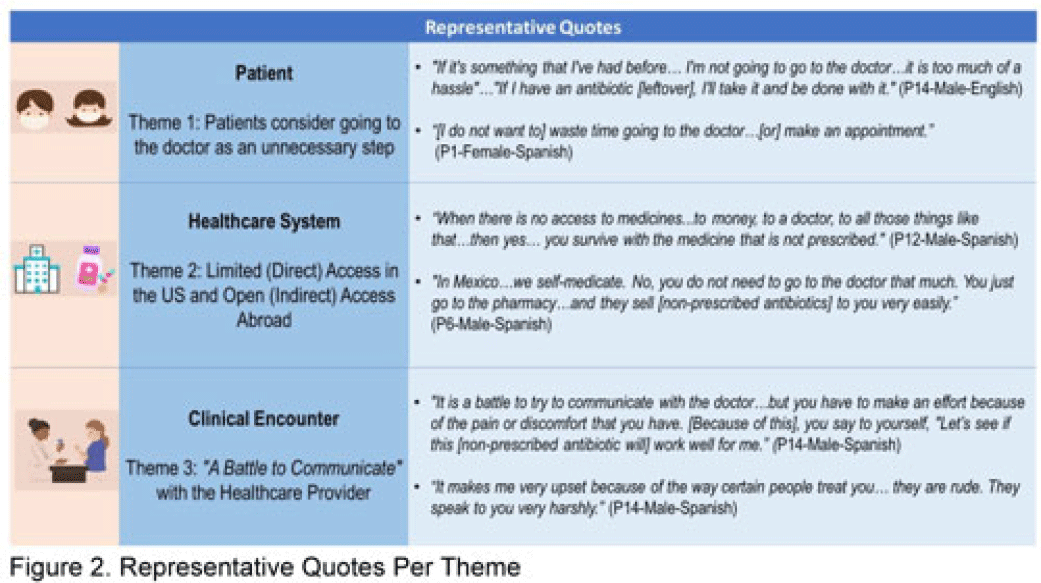
Background: Nonprescription antibiotic use includes taking an antibiotic without medical guidance (eg, leftover antibiotics, antibiotics from friends or relatives, or antibiotics purchased without a prescription). Nonprescription use contributes to antimicrobial resistance, adverse drug reactions, interactions, and superinfections such as Clostridioides difficile colitis. Qualitative studies exploring perspectives regarding nonprescription use among Hispanic patients are lacking. We used the Kilbourne Framework for Advancing Health Disparities Research to identify factors influencing Hispanic patients’ nonprescription use and to organize our findings. Methods: Our study includes Hispanic primary-care clinic patients with different types of health coverage in the Houston metroplex who endorsed nonprescription use in a previous quantitative survey. Semistructured interviews explored the factors promoting nonprescription use in Hispanic adults. Interviews were conducted remotely, in English or Spanish, between May 2020 and October 2021. We used inductive coding and thematic analysis to identify the factors and motives for nonprescription use. Results: Of the 35 Hispanic participants surveyed, 69% were female and between the ages of 27 and 66. All participants had some form of healthcare coverage (eg, Medicare or private insurance, Medicaid, or the county financial assistance program). Participants reported obtaining antibiotics from their own leftover prescriptions and through trusted persons (eg, herbalists, pharmacists, friends/relatives, and others), buying them under the counter in US markets, and purchasing them without a prescription outside the United States. Thematic analysis revealed the factors contributing to nonprescription use (Fig. 1). Themes included beliefs that the ‘doctor visit was unnecessary,’ ‘limited direct access to healthcare’ in the United States (due to limited insurance coverage, high costs of the doctor’s visits and medications, and long clinic wait times), ‘more open indirect access to healthcare’ abroad and under the counter in the United States, and communication difficulties (eg, language barriers with clinicians, perceived staff rudeness, and gaps in health literacy). Figure 2 shows representative quotes across thematic domains. Participants expressed having confidence in medical recommendations from pharmacists and trusted community members in their social networks. Conclusions: Antibiotic stewardship interventions that include pharmacist-driven patient education regarding appropriate antibiotic use may decrease nonprescription antibiotic use in Hispanic communities. Additionally, improving access to care while addressing communication barriers and cultural competency in clinics may improve primary care delivery and reduce potentially unsafe antibiotic use.
Disclosure: None


Identifying nonprescription antibiotic users with screening questions in a primary care setting
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s20-s21
-
- Article
-
- You have access
- Open access
- Export citation
-
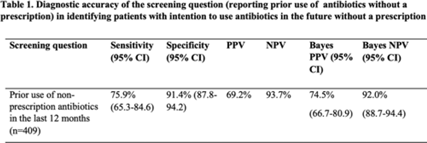
Background: Antibiotic use without a prescription (nonprescription use) leads to antibiotic overuse, with negative consequences for patient and public health. We studied whether screening patients for prior nonprescription antibiotic use in the past 12 months predicted their intentions to use them in the future. Methods: A survey asking respondents about prior and intended nonprescription antibiotic use was performed between January 2020 and June 2021 among patients in waiting rooms of 6 public clinics and 2 private emergency departments in economically and socially diverse urban and suburban areas. Respondents were classified as prior nonprescription users if they reported previously taking oral antibiotics without contacting a doctor, dentist, or nurse. Intended use was defined as answering “yes” or “maybe” to the question, “Would you use antibiotics without contacting a doctor, nurse, or dentist?” We calculated the sensitivity, specificity, and positive and negative predictive value (PPV and NPV) of prior nonprescription antibiotic use in the past 12 months for future intended nonprescription use. Bayes PPV and NPV were also calculated, considering the prevalence of nonprescription antibiotic use (24.8%) in our study. Results: Of the 564 patients surveyed, the median age was 51 years (SD, 19–92), with 72% of patients identifying as female. Most were from the public healthcare system (72.5%). Most respondents identified as Hispanic or Latino(a) (47%) or African American (33%), and 57% received Medicaid or the county financial assistance program. Prior nonprescription use was reported by 246 (43%) of 564 individuals, with 91 (16%) reporting nonprescription use within the previous 12 months. Intention to use nonprescription antibiotics was reported by 140 participants (25%). The sensitivity and specificity of prior nonprescription use in the past 12 months to predict the intention to use nonprescription antibiotics in the future were 75.9% (95% CI, 65.3–84.6) and 91.4% (95% CI, 87.8–94.2), respectively. After the Bayes’ adjustment, the PPV and NPV of prior use to predict future intention were 74.5% (95% CI, 66.7–80.9) and 92.0% (95% CI, 88.7–94.4) (Table 1). Conclusions: These results show that prior nonprescription antibiotic use in the past 12 months predicted the intention to use nonprescription antibiotics in the future (PPV of 75%). As a stewardship effort, we suggest clinicians use a simple question about prior nonprescription antibiotic use in primary-care settings as a screening question for patients at high risk for future nonprescription antibiotic use.
Financial support: HSQR-R 5R01HS026901-04
Disclosure: None

Molecular Epidemiology
Real-time whole-genome sequencing surveillance for outbreak detection and intervention
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s21
-
- Article
-
- You have access
- Open access
- Export citation
-
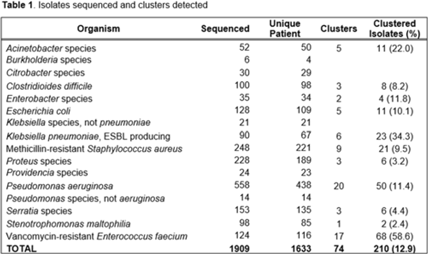
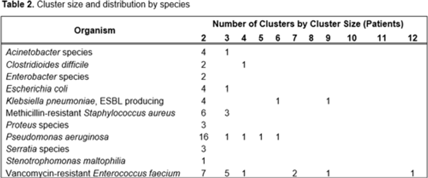
Background: Detecting healthcare-associated transmission and outbreaks often relies on reactive whole-genome sequencing (WGS), which occurs after the suspected transmission has occurred. Additionally, reactive WGS frequently misidentifies transmission and misses transmission when it has occurred. We initiated weekly real-time WGS to detect bacterial transmission and direct infection prevention interventions. We describe our experience after 1 year of real-time WGS surveillance at the University of Pittsburgh Medical Center–Presbyterian Hospital, a large, tertiary-care facility. Methods: Weekly WGS surveillance was performed from November 1, 2021, to October 31, 2022. Cultured isolates of select bacterial pathogens from patients who were hospitalized for ≥3 days or had a recent healthcare exposure in the prior 30 days were collected and sequenced. Isolates that were ≤15 single-nucleotide polymorphisms (SNPs) were considered genetically related clusters except for Clostridioides difficile (≤2 SNPs). Genetically related clusters were investigated for epidemiological links and interventions to interrupt transmission were implemented at the discretion of the infection prevention team. We analyzed subsequent infections that occurred within an outbreak after an intervention was in place. Results: In total, 1,909 isolates were sequenced. Of 1,633 unique patient isolates clustered by sequence type, 74 clusters were identified comprising 210 (12.9%) patient isolates (Table 1). The median time from culture date to sequencing was 14 days (IQR, 5.25). The median cluster size was 2 (IQR, 1) (Table 2). Overall, 118 patient isolates (56.2%) had an epidemiological link to a prior isolate, indicating potential transmission. Of 74 clusters, 66 (89.2%) received infection prevention interventions after notification based upon epidemiological data. The infection prevention team performed 69 total interventions, which included unit education (n = 28), hand hygiene observations (n = 16), enhanced cleaning (n = 16), environmental cultures or removal of endoscope (n = 7), and enhanced microbiology surveillance (n = 2). The 59 subsequent infections after infection prevention notification included 17 (28.8%) with no clear epidemiological link, and 41 (69.5%) with an epidemiological link either to a new transmission route (n = 37) or the same route prior to infection prevention intervention (n = 4). Only 1 (1.7%) subsequent infection within a cluster occurred after an infection prevention intervention from the same potential route, which was a suspected unit-based transmission of vancomycin-resistant Enterococcus faecium. Conclusions: Real-time WGS was effective at detecting genetically related clusters, finding potential sources, and halting further transmission after interventions by the infection prevention team. Quick turnaround times from patient culture to sequencing and analysis were vital for successful WGS surveillance. Real-time WGS surveillance has the potential to substantially shift the infection prevention paradigm for outbreak detection.
Disclosure: None


Outbreaks
Patient and facility characteristics of an NDM-producing Acinetobacter baumannii outbreak in California, 2020–2022
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s21-s22
-
- Article
-
- You have access
- Open access
- Export citation
-
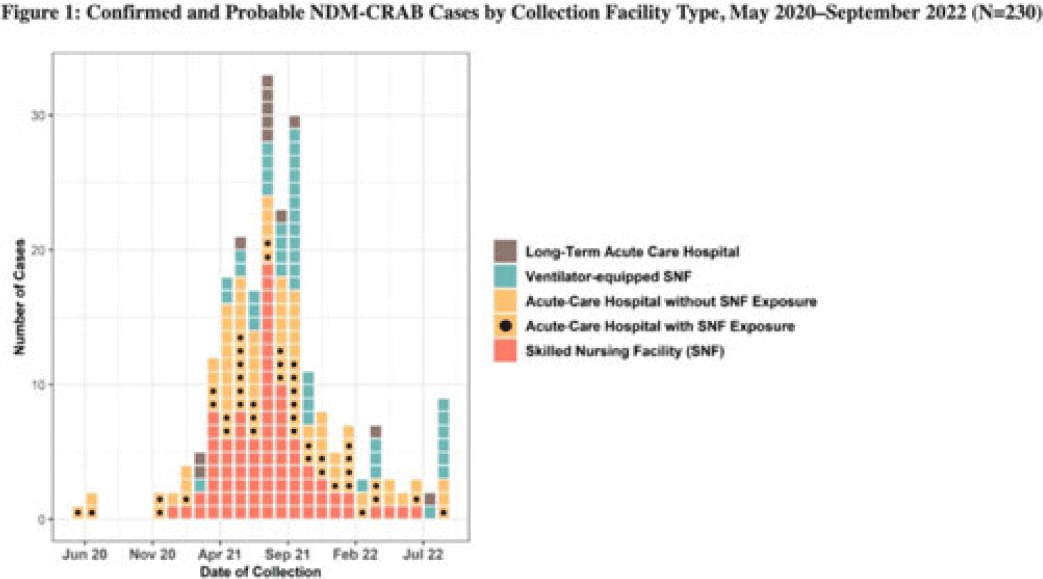
Background: Carbapenem-resistant Acinetobacter baumannii (CRAB) are bacteria that cause healthcare-associated infections and outbreaks. Most produce carbapenemases like New Delhi metallo-β-lactamase (NDM), which are more commonly found in carbapenem-resistant Enterobacterales but rarely in CRAB. In 2018, selected laboratories began participating in a public health sentinel surveillance program by routinely submitting CRAB and other antimicrobial-resistant isolates to the AR Laboratory Network for specialized testing. In May 2020, the Antimicrobial Resistance Laboratory Network detected the first NDM-CRAB case in California, triggering an investigation. Initial whole-genome sequencing of subsequent isolates indicated high relatedness. Methods: We defined confirmed cases as patients with NDM detected in CRAB isolates and probable cases as NDM detected in a screening swab from a patient epidemiologically linked to a known case(s) with specimens collected during May 2020–September 2022. We defined outbreak facilities as having (1) 1 or more newly identified cases during a point-prevalence survey in response to a known case or (2) at least 2 cases identified within 4 weeks of each other that were epidemiologically linked. We analyzed demographic and specimen characteristics, as well as healthcare exposure history using R Studio version 1.3.959 software. Results: Of 230 total patients, 176 (77%) were confirmed and 54 (23%) were probable cases; 150 (65%) were identified through colonization screening. Among 176 NDM-CRAB isolates, the most common specimen sources were respiratory (n = 29), wound (n = 28), and urine (n = 24), and 87 (49%) of 176 isolates were nonsusceptible to all antimicrobials tested. Among patients, median age was 65 years (range, 24–97), 127 (55%) were male, 37 (15%) were Hispanic or Latino, and 100 (43%) were White. We identified 37 outbreak facilities across 13 counties, including 25 acute-care hospitals (ACHs), 6 skilled nursing facilities (SNFs), 5 ventilator-equipped SNFs (vSNFs), and 1 long-term ACH. We identified 125 cases (54%) in SNFs and vSNFs and 93 cases (40%) in ACHs; among ACH patients, 43 (46%) had been SNF or vSNF residents within the prior year. No patients reported international exposure. Conclusions: The first known case of NDM-CRAB in California was detected by sentinel surveillance. In this extensive regional outbreak, most cases were identified by screening at public health and clinical laboratories. Transmission occurred across healthcare settings connected by patient sharing, underscoring the importance of communication, active surveillance, and implementation of infection prevention and control practices to mitigate spread within and between facilities. Expanding these efforts, with support and resources from public health departments, is key to detecting, characterizing, and containing future outbreaks of antimicrobial-resistant pathogens.
Disclosure: None

Poster Presentation - Poster Presentation
Antibiotic Stewardship
Three-day antibiotic duration in patients with pneumonia: A sixty-eight–hospital cohort
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s22
-
- Article
-
- You have access
- Open access
- Export citation
-
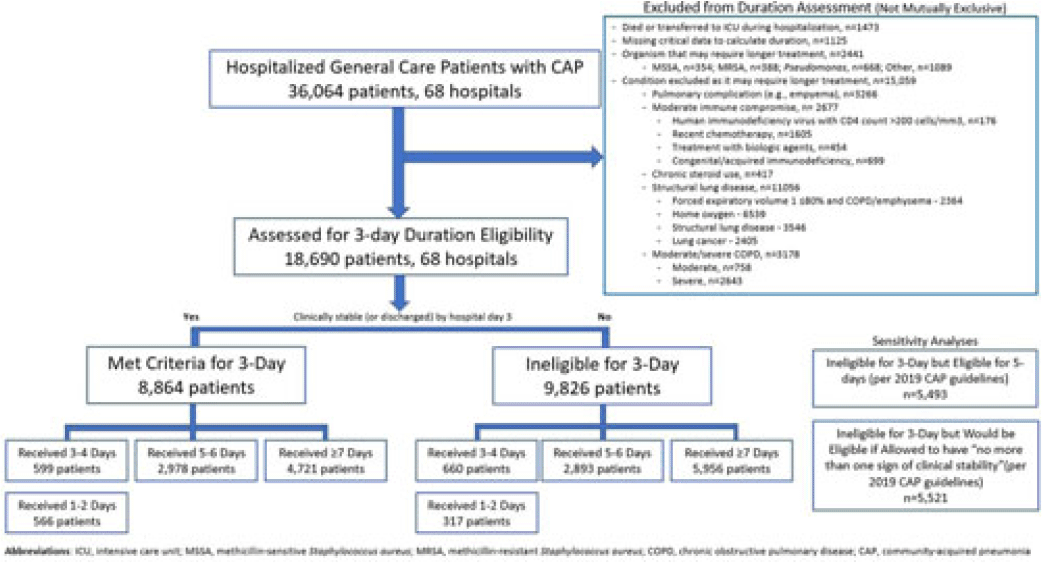
Background: Since 2019, community-acquired pneumonia (CAP) guidelines have recommended hospitalized patients be treated until clinical “stability and for no less than 5 days.” However, randomized trials have reported that, in patients who stabilize by hospital day 3, very short antibiotic durations (eg, 3 days) are noninferior to longer durations. How these trial results relate to real-world practice is unknown. Methods: Using a 68-hospital cohort study of hospitalized, general-care adults with CAP, we aimed to (1) quantify the percentage of patients who—according to trial criteria—qualify for a 3-day antibiotic duration, (2) quantify the percentage who actually received a 3-day duration, and (3) assess 30-day outcomes. Patients were considered to have CAP if they had a pneumonia discharge diagnosis and met clinical criteria for CAP. Patients with concomitant infections (including COVID-19), admission to intensive care, or severe immunocompromise were not included. Results: Between February 23, 2017, and August 3, 2022, 36,064 patients with CAP were included. Of those, 48.2% (9,826 of 36,064) were excluded due to a condition or organism ineligible for the 3-day treatment (Fig. 1). Of the 18,690 patients remaining, 52.6% (9,826) were unstable on day 3 and thus were ineligible for the 3-day treatment. Therefore, of all 36,064 patients, only 8,864 (24.6%) would be eligible under trial criteria for a 3-day treatment. Notably, 5,493 (55.9%) of 9,826 patients unstable on day 3 would be eligible for 5 days of treatment under national guidelines. In practice, use of 3–4-day treatment was rare, occurring in 599 (6.8%) of 8,864 patients eligible for a 3-day treatment versus 660 (6.7%) of 9,826 patients unstable on day 3 (P = .945). Use of 3–4-day treatment increased over time and comorbidities that could mimic CAP or a negative procalcitonin were more common in patients who received a 3–4-day treatment whereas specific symptoms of CAP were less common (Fig. 2). After adjustments, patients eligible for a 3-day duration who received a 3–4 day treatment versus a ≥5-day treatment had higher 30-day mortality (aOR, 1.87; 95% CI, 1.32–2.64) and readmission (aOR, 1.35; 95% CI, 1.17–1.56). Conclusions: Across 68 hospitals, <25% of patients hospitalized with CAP would be eligible for a 3-day antibiotic treatment. Though increasing over time, there was little use of 3–4-day treatments and, when prescribed, outcomes were worse, potentially due to CAP misdiagnosis. Given the small number of patients eligible for 3-day treatment, and the potential harm with too-short durations, it may be prudent to focus on increasing the use of 5-day treatments.
Disclosures: None

High prevalence of antibiotic use in a tertiary-care hospital in Sierra Leone: We need to handle antibiotics with care
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s22-s23
-
- Article
-
- You have access
- Open access
- Export citation
-
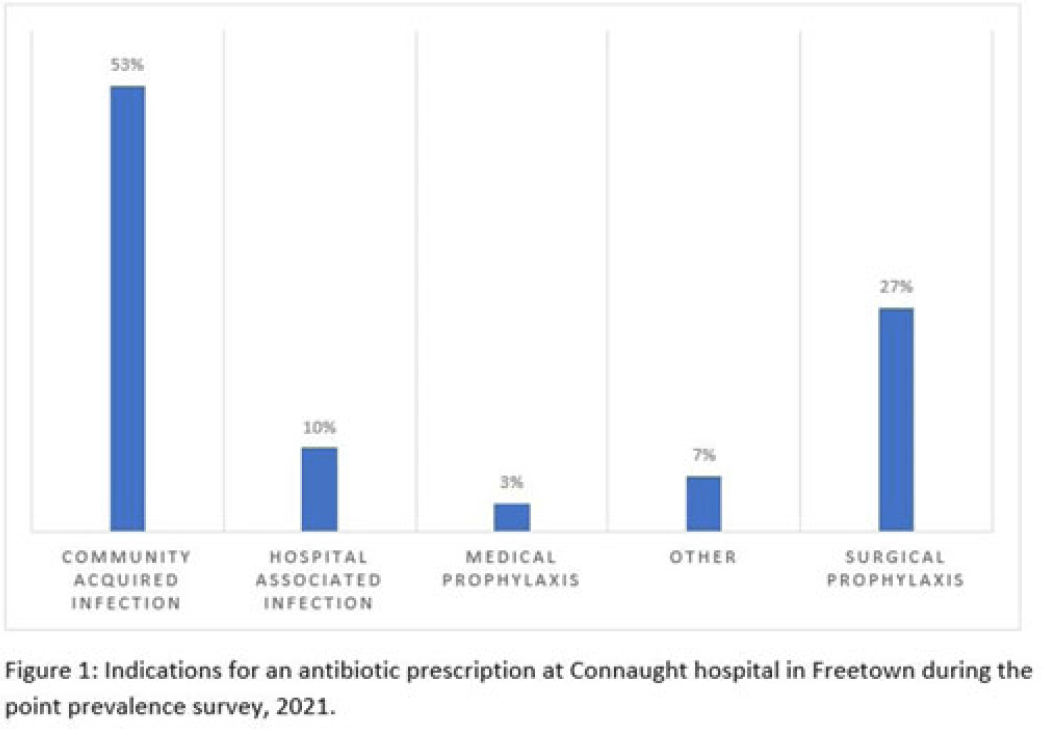
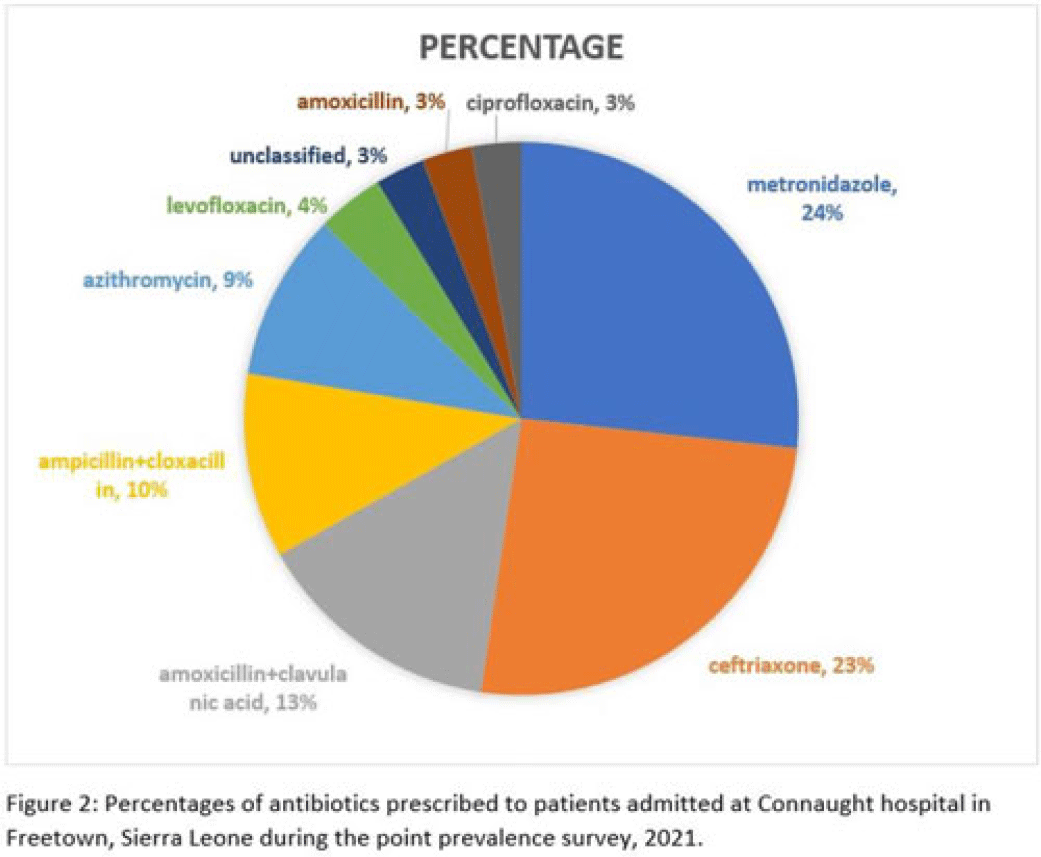
Background: Antimicrobial resistance (AMR) is a global public health concern that has the potential to reverse decades of progress aimed at decreasing morbidity and mortality attributed to infectious diseases. In 2019, ~5 million deaths were associated with AMR, of which 1.2 million were attributed to antibacterial-resistant infections. Healthcare facilities where antimicrobials are frequently used are high-risk settings for the selection and spread of resistant bacteria, and they further contribute to the increase in the burden of AMR. We have documented the prevalence and indication of antibiotic use in a tertiary-care referral hospital in Freetown, Sierra Leone. Methods: This point-prevalence survey was conducted at Connaught hospital, a tertiary-care hospital in Sierra Leone, in November 2021. The hospital offers a range of medical and surgical services through 25 units and has 16 wards with >300 beds. Data on patient-level antibiotic use, including indications for use, were extracted from medical records using WHO point-prevalence survey (PPS) forms that had been pretested and validated. Data collection was conducted in all the wards over a 10-day period by trained healthcare personnel. On the day of the survey, only the medical records of patients on admission before 8:00 a.m. on that day were included in the study. Data entry, cleaning, and analysis were conducted using the WHO PPS platform. Ethical approval was obtained. Results: In total, 87 patient records were included in the survey. Most (71%) were women, and the average age was 30.6 years. The prevalence of antibiotic use was 66%, and the average number of antibiotics prescribed to patients since admission was 2. The 5 most prescribed antibiotics were metronidazole, ceftriaxone, amoxicillin and clavulanic acid, ampicillin and cloxacillin, and azithromycin. The parenteral route of drug administration was the mainstay. The most frequent indications for antibiotic prescription were community-acquired infection and surgical prophylaxis. Blood-culture requests were not ordered before the initiation of antibiotic treatment. Conclusions: This study was the first study to be conducted in Connaught hospital using the WHO PPS methodology. The survey reports a high prevalence (60%) of antibiotic use, and most treatment was done empirically. This finding is contrary to the WHO recommendation of <30% antibiotic use. This high prevalence of antibiotic use has the potential to increase the burden of AMR in the country. Therefore, there is an urgent need to strengthen Connaught hospital’s antibiotic stewardship program.
Disclosures: None



Sex differences in knowledge and practices regarding antibiotics and antibiotic resistance in the Puerto Rican population
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s23-s24
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Antibiotic resistance is one of the biggest threats to global health, and by 2050 it is expected to cause 10 million deaths per year globally. Sex differences depend on context and sociodemographic factors; therefore, studies addressing sex differences have been inconclusive. Furthermore, to our knowledge, sex differences in the Puerto Rican population have not been analyzed. We sought to understand whether knowledge and practices regarding antibiotic use and antibiotic resistance in the Puerto Rican population differ by sex. Methods: A convenience sampling was performed at outpatient clinics across Puerto Rico. Those who agreed to participate completed a self-report questionnaire aimed to address demographics, antibiotic knowledge, and experiences. Bivariate analyses were performed using Stata version 17.0 software. Results: In total, 252 participants received the questionnaire, and 250 completed it. Most of the participants were female (71.2%), aged >56 years (40.0%), and had a high school diploma (40.4%). Women had 2.71 (95% CI, 1.1–6.8, P). Conclusions: Women perceived themselves to be more knowledgeable regarding antibiotic use and resistance than men. However, no difference in actual knowledge could be identified. Similarly, antibiotic-related practices did not differ by sex except for using previously saved antibiotic treatment, and men had higher odds of conducting this practice. Further studies should be conducted to understand the factors that influence these behavioral practices, and educational interventions should focus on addressing misconceptions regarding antibiotics and antibiotic resistance.
Disclosures: None

Reducing the rate of guideline-discordant therapy for inpatients with community-acquired pneumonia
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s24
-
- Article
-
- You have access
- Open access
- Export citation
Determining trends of respiratory tract infections in a long-term care facility pilot surveillance project
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s24
-
- Article
-
- You have access
- Open access
- Export citation
Pharmacist interventions for appropriate COVID-19 antiviral therapy in long-term care facilities: A public health initiative
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s24-s25
-
- Article
-
- You have access
- Open access
- Export citation
-
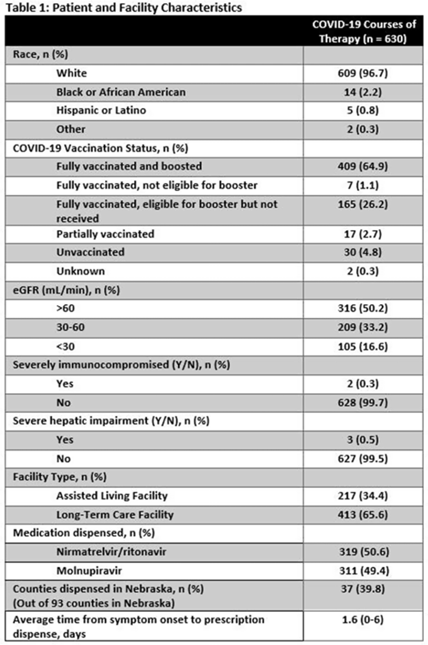
Background: Prescribing errors related to the COVID-19 oral antiviral agent nirmatrelvir-ritonavir have been reported and are primarily due to improper renal dosing and significant drug–drug interactions. These patient safety issues are particularly concerning in the long-term care facility (LTCF) population. The Nebraska Antimicrobial Stewardship Assessment and Promotion Program (ASAP) is a unique collaborative partnership involving the University of Nebraska Medical Center, Nebraska Medicine, and the Nebraska Department of Health and Human Services (DHHS). ASAP is funded through the Nebraska DHHS healthcare-associated infections and antimicrobial resistance (HAI/AR) program and was established in 2016, with a primary focus of promoting safe and effective antimicrobial use in Nebraska. In 2022, ASAP developed a statewide pharmacist-led service to assist LTCFs in evaluating prescriptions for COVID-19 oral therapeutics. We studied the impact of ASAP pharmacist intervention on COVID-19 oral antiviral prescriptions. Methods: ASAP created a centralized LTCF treatment request process for oral antivirals. A REDCap survey hosted on a dedicated program webpage was used to collect requests for treatment submitted by any LTCF in Nebraska, including assisted living facilities. An ASAP pharmacist reviewed each survey submission for renal and hepatic function, drug–drug interactions, date of symptom onset, and ability to take oral medications. After pharmacist approval, delivery of the appropriate COVID-19 therapeutic to the LTCF was coordinated with the dispensing pharmacy. The pharmacists recorded the specific interventions for each treatment in the program database. Descriptive analyses were used to study the program impact. Results: In total, 630 courses of oral COVID-19 antivirals were administered to Nebraska LTCF residents through the ASAP program in 2022. The median patient age was 84 years, and 59% were female. Most dispensed courses (n = 410, 65%) needed pharmaceutical interventions upon review for 506 individual interventions. The most frequent intervention was to hold or adjust doses of concomitant medications in 205 patients (33%), followed by antiviral dose adjustment for renal function in 117 patients (19%), and selecting an alternative COVID-19 therapy due to drug–drug interactions in 108 patients (17%). COVID-19 therapeutic agents were changed upon ASAP intervention to be in compliance with the National Institute of Health COVID-19 treatment guidelines in 37 patients (6%). Conclusions: Pharmacist review of oral antiviral prescriptions for COVID-19 through a public health–supported initiative identified and prevented potential patient safety issues in LTCF residents. Future studies should analyze the impact of similar interventions on patient outcomes.
Disclosures: None

Antibiotic practice and stewardship in the management of neutropenic fever: A survey of US institutions
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s25
-
- Article
-
- You have access
- Open access
- Export citation