
Contents
Poster Presentation - Poster Presentation
Diagnostic/Microbiology
Assessment of endotracheal aspirate culture appropriateness among adult ICU patients at an academic medical center
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s63
-
- Article
-
- You have access
- Open access
- Export citation
-
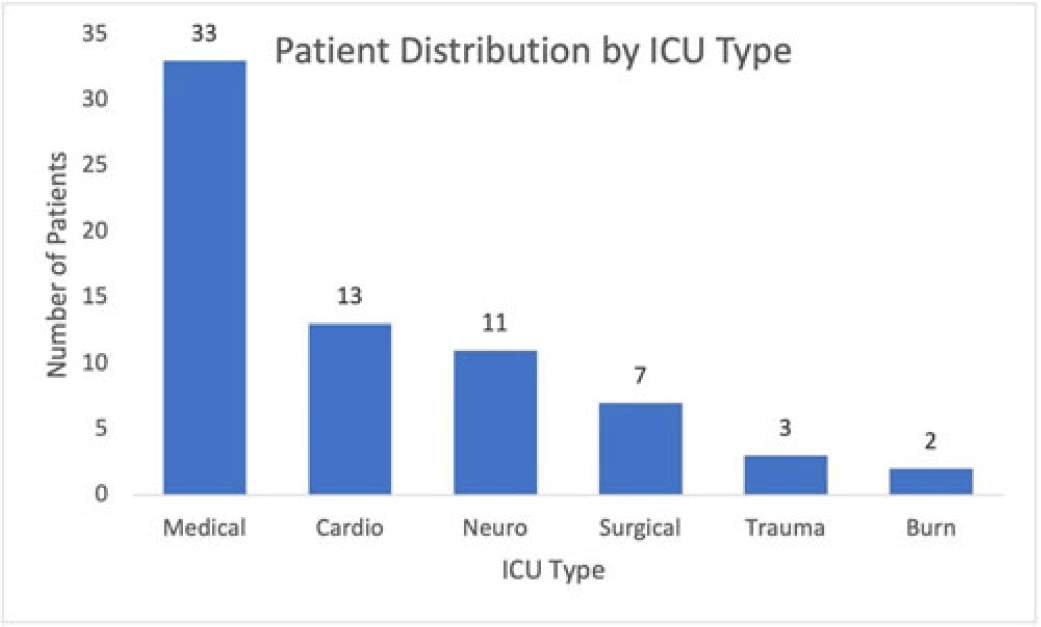
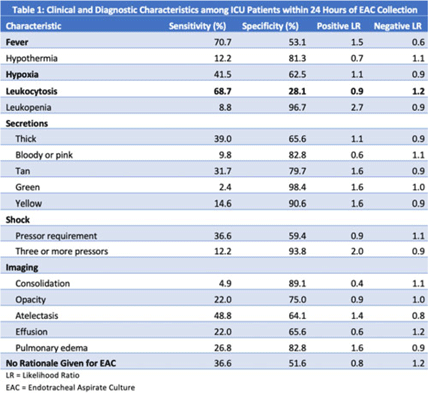
Background: Ventilator-associated pneumonia (VAP) is a significant cause of mortality in intensive care units (ICUs), but minimal research exists regarding the appropriateness of ordering endotracheal aspirate cultures (EACs). We evaluated the diagnostic utility of rationales given for EAC collection in ICUs at an academic medical center to assess potentially inappropriate EAC ordering. Methods: The study population comprised all adult patients admitted to an ICU in 2019 who underwent EAC collection. A random 10% sample from this population, stratified by ICU type, was selected. Clinical and diagnostic characteristics within 24 hours of EAC collection were identified by chart review. Clinical documentation was reviewed to identify ICU provider rationales for ordering EAC. Results: In total, 749 patients underwent EAC collection. Among them, 75 patients comprised the random sample, of whom 7 (9.3%) were excluded due to extubation before culture collection. Figure 1 shows patient distribution by ICU type. From these 68 patients, 105 EACs were collected. Of these, 41 (39%) were positive for potential pathogens, and 59 (56.2%) had explicit rationales for EAC collection, including fever (44.1%), hypoxia (18.6%), leukocytosis (16.9%), secretions (11.9%), shock (10.2%), and radiologic findings (8.5%). Also, 43.8% of EACs had no explicit rationale for collection. Table 1 shows sensitivities, specificities, positive likelihood ratios (LRs), and negative LRs for these rationales and related characteristics. Conclusions: EACs were commonly ordered without clear clinical indications. Of the noted rationales for EAC collections, most performed poorly at predicting positive cultures, which challenged common rationales for ordering EAC. This study could serve as a foundation for diagnostic stewardship interventions for EAC, potentially decreasing unnecessary cultures.
Disclosures: None


Dialysis
Developing a statewide infection prevention program assessment service for dialysis settings using a six-sigma framework
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s63-s64
-
- Article
-
- You have access
- Open access
- Export citation
Characterization of negative health outcomes for dialysis events by vascular access type—Tennessee, 2015–2019
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s64
-
- Article
-
- You have access
- Open access
- Export citation
-
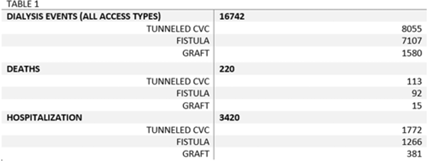
Background: The dialysis patient population is at a higher risk for nosocomial infections as well as related negative consequences including hospitalization and death. The CMS and the state of Tennessee mandate reporting of 3 types of dialysis events: positive blood culture, intravenous antimicrobial starts, and pus, redness, or increased swelling at the access site. We explored hospitalization and death outcomes by vascular access types for dialysis events reported to the NHSN for licensed outpatient hemodialysis clinics in Tennessee from 2015 to 2019. Methods: We looked at the frequency of hospitalization and death among those who experienced a dialysis event for 3 types of vascular access: arteriovenous fistula, arteriovenous graft, and tunneled central venous catheter (CVC). Other vascular-access types were excluded due to low usage rates. Odds ratios and confidence intervals were used to quantify the relationship between access type and hospitalization, and access type and death. Pooled analysis was used due to the stable rates of death and hospitalization among access types from 2015 to 2019. Results: From 2015 to 2019, 16,742 dialysis events were reported for the 3 access types: 8,055 dialysis events (48.1%) occurred among those with tunneled CVCs, 7,107 (42.5%) occurred among those with fistulas, and 1,580 (9.4%) occurred among those with grafts. Of the 16,742 dialysis events, 3,420 patients (20.4%) were hospitalized either due or related to their dialysis event; 220 (1.3%) deaths occurred either due to or related to the patient’s dialysis event. The odds of being hospitalized was 1.47 (95% CI, 1.29–1.67) times greater in those with grafts compared to those with fistulas. Patients with tunneled CVCs were 1.30 (95% CI, 1.20–1.41) times greater to be hospitalized compared to those with fistulas. The odds of death was 1.09 (95% CI, 0.9–2.5) times greater in those patient with tunneled CVCs compared to those with fistulas, whereas the odds of death among patients with grafts was 0.73 (95% CI, 0.82–1.43) times the odds of death compared to patients with fistulas. Conclusions: Overall, our findings conclude hemodialysis patients with tunneled CVCs have an increased risk for the negative health outcomes of hospitalization and death when compared to the other access types, supporting previous studies. Additionally, grafts had a higher risk of hospitalization compared to fistulas, but patients with grafts had lower odds of death than those with fistulas. Further investigation is needed to study how the COVID-19 pandemic may have affected the trends of negative health outcomes related to dialysis events.
Disclosures: None

Disinfection/Sterilization
Measuring the efficacy of routine disinfection methods on frequently used physical therapy equipment
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s64-s65
-
- Article
-
- You have access
- Open access
- Export citation
-
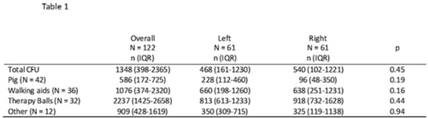
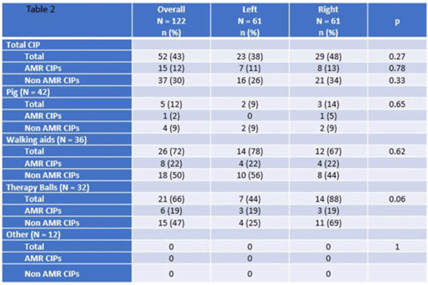
Background: Frequently used physical therapy (PT) equipment is notably difficult to disinfect due to equipment material and shape, however, the efficacy of standard disinfection of PT equipment is poorly understood. Methods: We completed a prospective observational microbiological analysis of fomites used in adult or pediatric PT at Duke University Health System, Durham, North Carolina, from September to December 2022. Predetermined study fomites were obtained after being used during a clinical shift and standard disinfection had been completed by clinical service staff. Fomites were split into 2 halves, left and right, for sampling. Samples were taken with premoistened cellulose sponges processed using the stomacher technique and were incubated on appropriate selective and general medias. We defined antimicrobial-resistant, clinically important pathogens (AMR-CIP) as MRSA, VRE, and MDR-gram-negative isolates, and non–AMR-CIP as MSSA, VSE, and gram-negative species. Study fomites were grouped as follows: (1) pediatric pig toy, (2) walking aids (walkers or canes), (3) balls (medicine, dodge, etc), and (4) other (foam roller, sliding board, etc). Results: In total, 47 patients, 61 fomites, and 122 were analyzed. Of the study patients, 24 (51%) were female, 13 (27%) had active infections, and 15 (32%) were on contact precautions. Because fomites were split in half, patients in the left and right study arms were identical. Overall, the median total colony-forming-units (CFU) of study fomites was 1,348 (IQR, 398–2,365): 468 (IQR, 161–1,230) for the left side study arm and 540 (IQR, 102–1,221) for the right study arm (P = .45). At the sample level, 52 (43%), 15 (12%), and 37 (30%) of 122 samples harbored any CIPs, AMR CIPs, or non-AMR CIPs, respectively. At the fomite level, 27 (44%), 5 (8%), 15(25%), and 7 (11%) of 61 fomites harbored any CIPs, only AMR-CIPs, only non-AMR CIPs, or both AMR and non-AMR CIPs, respectively. Generally, therapy balls were the most contaminated study fomites (n = 2,237; IQR, 1,425–2,658), and walking aids were most frequently contaminated with any CIPs (n = 26, 72%), AMR CIPs (n = 8, 22%), and non-AMR CIPs (n = 15, 47%). Discussion: Following routine disinfection, frequently used PT equipment remained heavily contaminated and harbored AMR and non-AMR CIPs, supporting the notion that PT equipment is difficult to disinfect via standard disinfection. Additionally, left-, and right-side fomite divisions had similar pathogens, suggesting that this sampling model of intrapatient comparisons may be helpful for resolving case-mix issues in future studies. Future work should focus on PT-specific enhanced disinfection strategies to improve the disinfection of PT equipment.
Financial support: This study was funded by PURioLABS.
Disclosures: None


Decontamination of bedding reduces the risk for contamination of personnel changing bedding: A simulation study
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s65
-
- Article
-
- You have access
- Open access
- Export citation
-
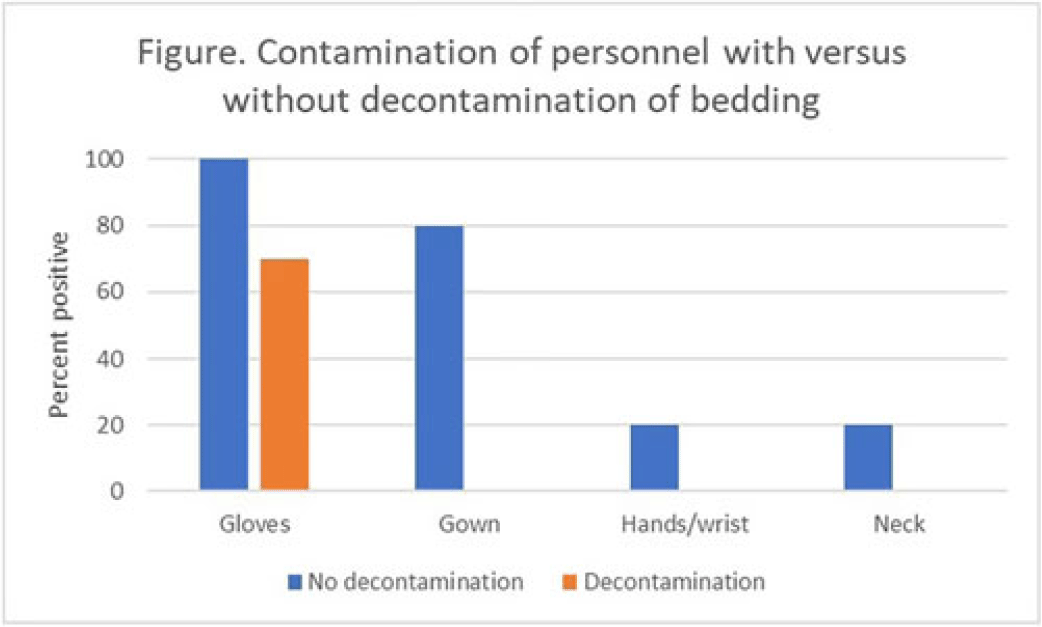
Background: The recent worldwide outbreak of Mpox virus infections has raised concern about the potential for nosocomial acquisition during handling of contaminated bedding or clothing. We conducted simulations to test the hypothesis that decontamination of bedding prior to handling could reduce the risk for contamination of personnel. Methods: We conducted a crossover trial to test the effectiveness of spraying contaminated bedding with a hydrogen peroxide disinfectant in reducing contamination of personnel during handling of the contaminated bedding. Bedding was contaminated on top and bottom surfaces with aerosolized bacteriophage MS2. Personnel (N = 10) wearing a cover gown and gloves removed the bedding from a patient bed and placed it into a hamper both with and without prior hydrogen peroxide spray decontamination. After handling the bedding, samples were collected to assess viral contamination of gloves, cover gown, neck or chest, and hands or wrists. Results: Contamination of the gloves and cover gown of personnel occurred frequently during handling of bedding and 20% of participants had contamination of their hands or wrists and neck after the simulation (Fig.). Decontamination of the bedding reduced contamination of the gloves and eliminated contamination of the cover gown, hands or wrists, or neck. Conclusion: Decontamination of bedding prior to handling could be an effective strategy to reduce the risk for nosocomial acquisition of Mpox by healthcare personnel.
Disclosures: None

Emerging Pathogens
Healthcare personnel with laboratory-confirmed mpox in California
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s65-s66
-
- Article
-
- You have access
- Open access
- Export citation
Genetic relatedness among Neisseria gonorrhoeae isolates in southeastern Michigan
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s66-s67
-
- Article
-
- You have access
- Open access
- Export citation
-
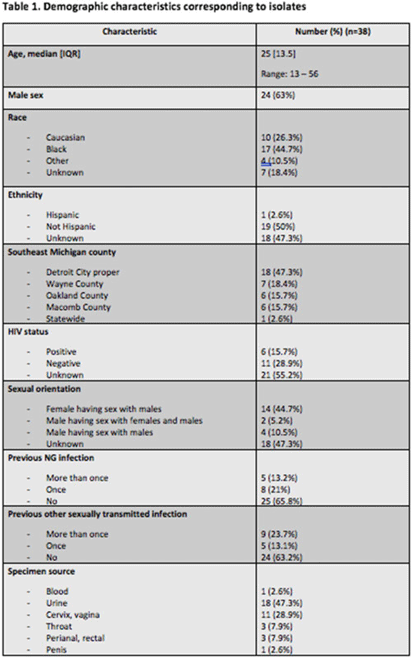
Background: Antimicrobial resistance (AMR) in Neisseria gonorrhoeae (NG) is an emerging public health crisis. Whole-genome sequencing (WGS) is an efficient way of predicting AMR determinants and their spread in the population. In a previous study, genotype–phenotype correlation analyses among NG isolates to determine antimicrobial resistance revealed discordance for azithromycin (AZM) and ceftriaxone (CRO) compared to other antibiotics. We investigated the evolutionary relatedness of NG isolated from patients with sexually transmitted infection (STI) using WGS in southeastern Michigan. Methods: Isolates, corresponding demographic data, and minimum inhibitory concentrations (MIC) via E-test (CRO) and broth microdilution (AZM) were obtained from the Michigan Department of Health and Human Services. Whole-genome libraries were prepared using the QIAseq FX kit followed by sequencing on a NovaSeq6000 (>200X Coverage); samples were aligned to NG reference strain TUM19854 (NZ_AP023069.1) using Snippy before phylogenetic tree generation using Neighbor-joining clustering on the core.aln files. Phylogenetic trees were visualized using ATGC:PRESTO. Results: In total, 38 isolates were analyzed. Demographic data and susceptibility testing results are noted in Table 1. Most isolates were from males (63%), Blacks (44.7%), individuals living in Detroit City proper (47.3%), and those with unknown HIV status (55.2%). More than one-third had prior STI, including NG. All isolates were susceptible to CRO (CLSI susceptible breakpoint MIC, 1). Within the phylogenetic tree, 8 main branches were identified (Fig. 1). Moreover, 1 branch contained a cluster with 12 closely related isolates, which included the 9 isolates with nonsusceptible AZM. Nearly all isolates in that cluster had been collected from Detroit City proper and Wayne County, suggesting epidemiological overlap and potential spread of resistant strains in those counties.
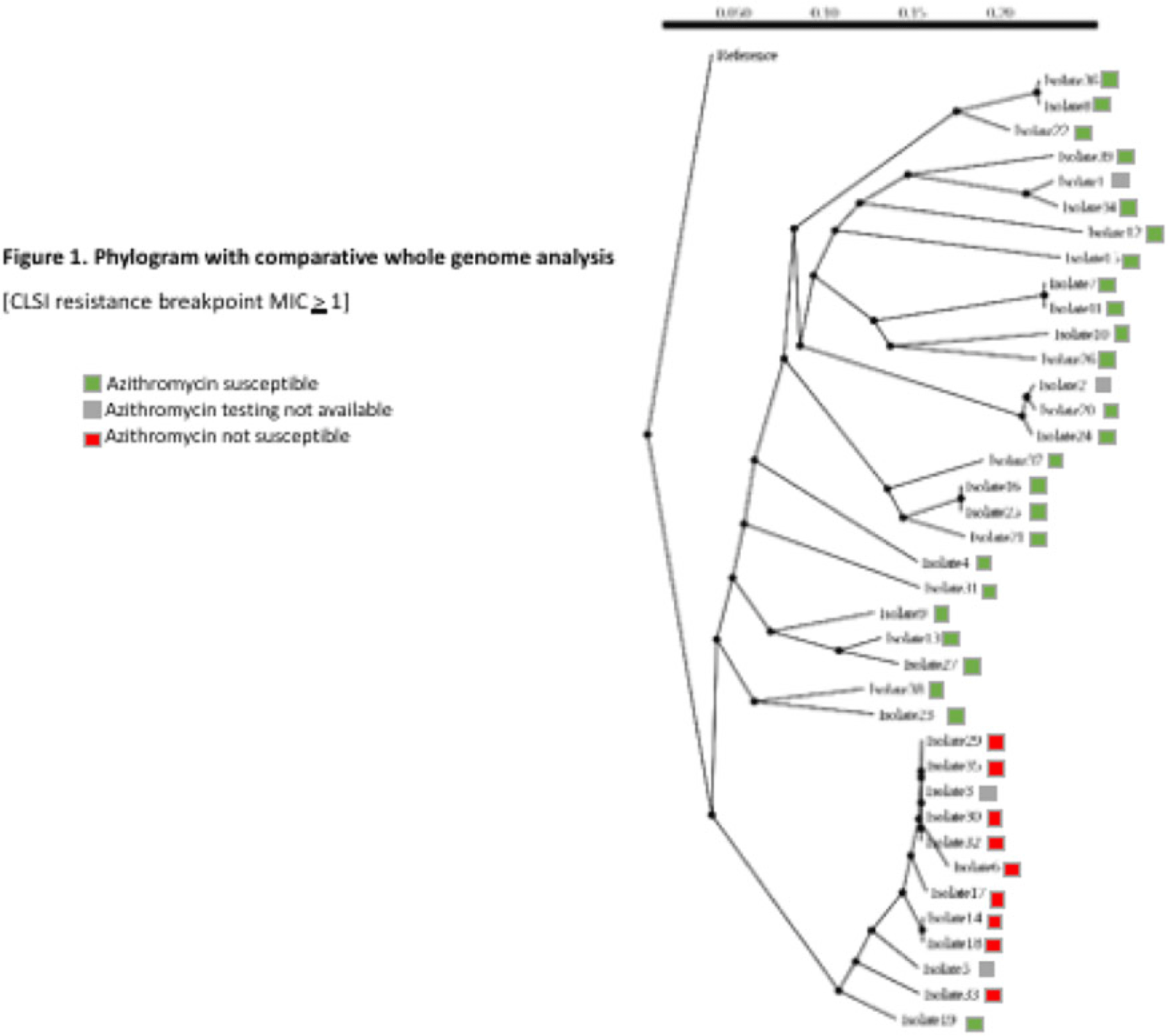 Conclusions: Comparative whole-genome and phylogenetic analyses among a subset of NG isolates revealed clustering of AZM resistance strains, suggesting a genomic component to AMR. Further studies are needed to determine the utility of WGS in diagnosis, outbreak investigations, and management of NG infections.
Conclusions: Comparative whole-genome and phylogenetic analyses among a subset of NG isolates revealed clustering of AZM resistance strains, suggesting a genomic component to AMR. Further studies are needed to determine the utility of WGS in diagnosis, outbreak investigations, and management of NG infections.Disclosures: None


Mpox exposure on a congregate inpatient psychiatry unit: Description of the investigation and outcomes—New York City, 2022
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s67
-
- Article
-
- You have access
- Open access
- Export citation
Environmental Cleaning
Effect of dry hydrogen peroxide on Candida auris environmental contamination
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s67-s68
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Candida auris is an emerging pathogen that exhibits broad antimicrobial resistance and causes highly morbid infections. Prolonged survival on surfaces has been demonstrated, and standard disinfectants may not achieve adequate disinfection. Persistent patient colonization and constant environmental recontamination poses an infection risk that may be mitigated by no touch disinfection systems. We evaluated the efficacy of continuous dry hydrogen peroxide (DHP) exposure on C. auris environmental contamination. Methods: The study was conducted in a large tertiary-care center where multiple patients were identified as either infected or colonized with C. auris. DHP-emitting systems were installed in the ventilation systems dedicated to the adult burn intensive care and children’s cardiac intensive care units. Composite surface samples were collected in a sample of patient rooms and shared clinical workspaces among units with current C. auris patients, before and after installation of the DHP system, and from areas with and without exposure to DHP. The samples included “high touch” surfaces near the patient, the general area of the patient room, shared medical equipment for the unit, shared staff work areas, and equipment dedicated to individual staff members (Table 1). Presence of C. auris was determined by polymerase chain reaction (PCR). Association between DHP exposure and C. auris contamination was determined using the Fisher exact test. Results: In the presence of C. auris patients, 5 baseline samples per unit were taken before DHP was installed, and then 5 samples per unit were taken on days 7, 14, and 28 after installation. Prior to initiation of DHP, 7 (70%) of 10 samples were PCR positive for C. auris. After DHP installation, a statistically significant decrease to 5 (16.7%) of 30 samples (P <.05) was observed. In total, 20 samples (5 before installation and 15 after installation) were collected from units without DHP on the same days. At baseline, 2 (40%) of 5 samples were PCR positive for C. auris. During subsequent periods, 4 (27%) 15 samples were positive (P = .66). No adverse effects were reported by patients, visitors, or personnel in association with the operation of the DHP systems. Conclusions: These findings suggest that DHP is effective in reducing surface C. auris contamination in a variety of patient and healthcare worker surfaces.
Disclosures: None

Environmental cleaning in operating rooms: A systematic review from the human factors engineering perspective
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s68-s70
-
- Article
-
- You have access
- Open access
- Export citation
-
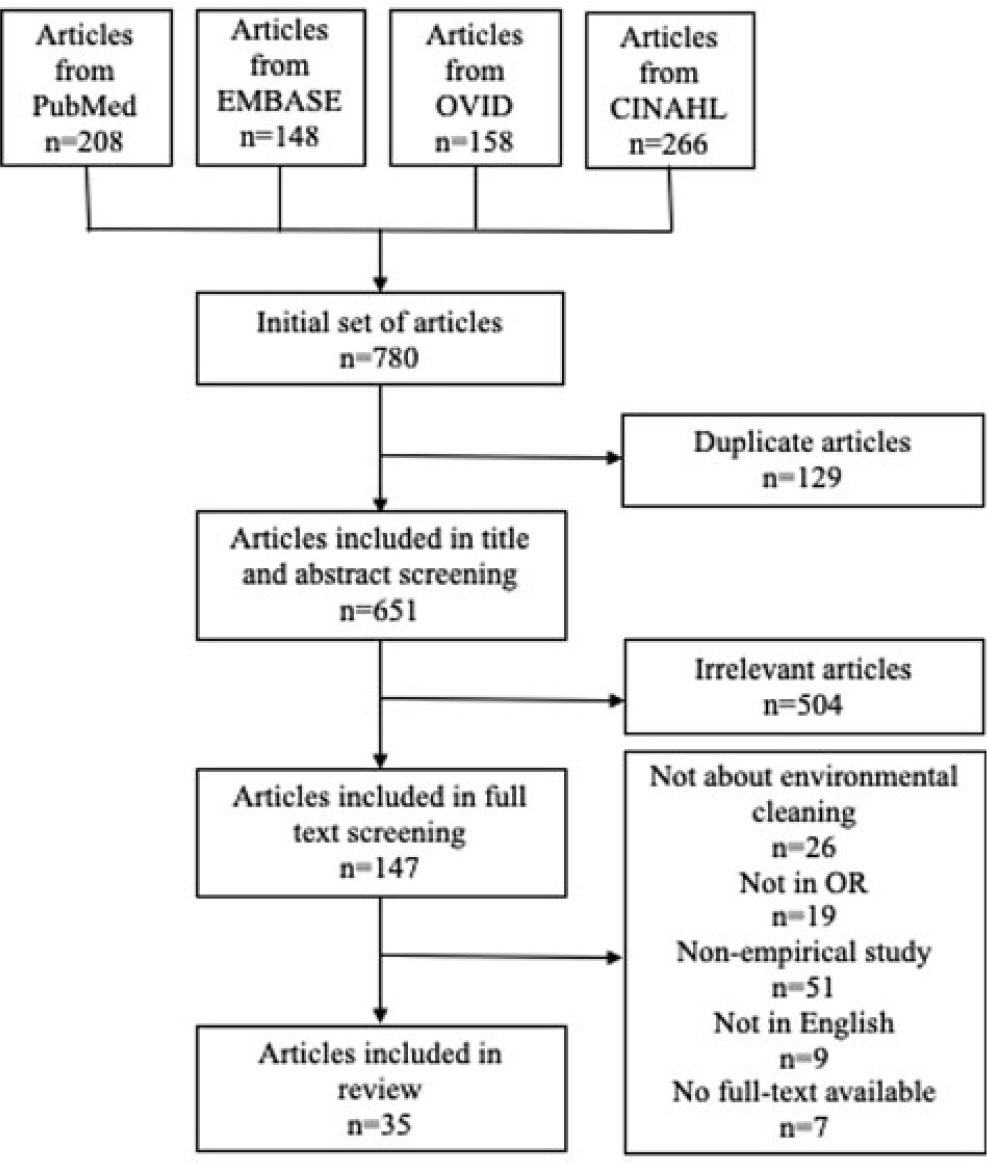
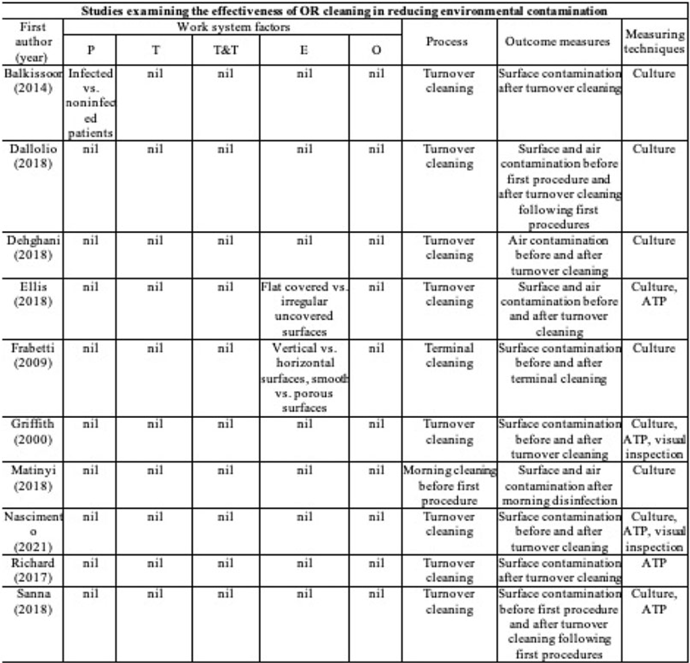
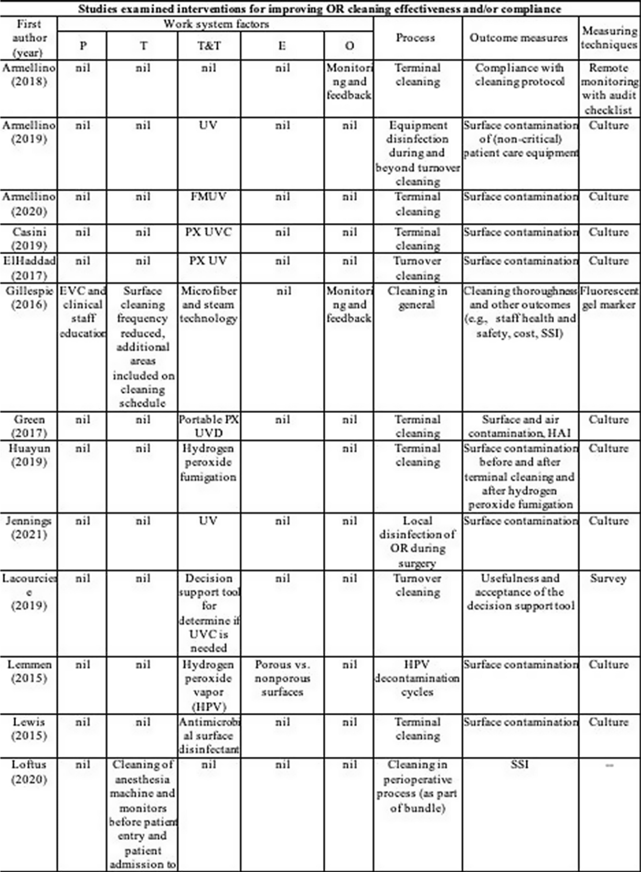
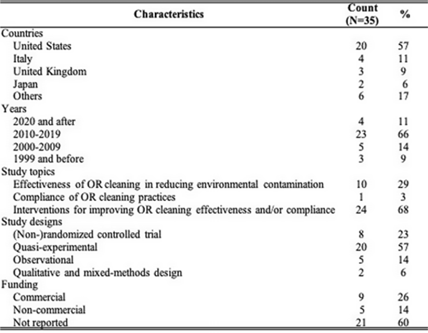
Background: Environmental cleaning is critical in preventing pathogen transmission and potential consecutive healthcare-acquired infections. In operating rooms (ORs), multiple invasive procedures increase the infectious risk for patients, making proper cleaning and disinfection of environmental surfaces of paramount importance. A human-factors engineering (HFE) approach emphasizing the impact of the entire work system on care processes and outcomes has been proposed to improve environmental cleaning. Using the lens of this HFE approach, we conducted a systematic review to synthesize existing evidence and identify gaps in the literature on OR cleaning. Methods: The systematic review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and limited to English-written, peer-reviewed journal articles reporting empirical studies on OR cleaning. Figure 1 shows the flowchart of study search and screening. The following data were extracted from each included article: (1) general information of the article (eg, first author, title, journal, year of publication) and (2) characteristics of the study (eg, country, objectives, design, outcome measures and measuring techniques, findings, funding source). In addition, work-system elements (eg, people, tasks, tools and technologies, physical environment, organizational conditions) and cleaning processes (eg, turnover cleaning, terminal cleaning) addressed in each included studywere coded based on the Systems Engineering Initiative for Patient Safety (SEIPS) model. The methodological quality of included studies using a (non)randomized controlled design was assessed using the version 2 of the Cochrane risk-of-bias tool for randomized trials. Results: In total, 35 studies were included in this review, among which 10 examined the effectiveness of OR cleaning in reducing environmental contamination (Fig. 2), 1 examined the compliance of OR cleaning practices (Fig. 3), and 24 examined interventions for improving OR cleaning effectiveness and/or compliance (Fig. 4). Figure 5 summarizes the characteristics of the included studies. Conclusions: In this review, OR cleaning was inconsistently performed in practice, and mixed findings were reported regarding the effectiveness of OR cleaning in reducing environmental contamination. No study has systematically examined work-system factors influencing OR cleaning. Efforts to improve OR cleaning focused on cleaning tools and technologies (eg, ultraviolet light) and staff monitoring and training. Interventions targeting the broader work system influencing the cleaning processes are lacking. The scientific rigor of the included studies was modest. Most studies were either commercially funded or did not reveal their funding sources, which might introduce a desirability bias.
Financial support: This study was funded by the Centers for Disease Control and Prevention.

Disclosures: None





Some like it hot: Variable impact of a tailpiece heating device on different gram-negative bacteria
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s70
-
- Article
-
- You have access
- Open access
- Export citation
-
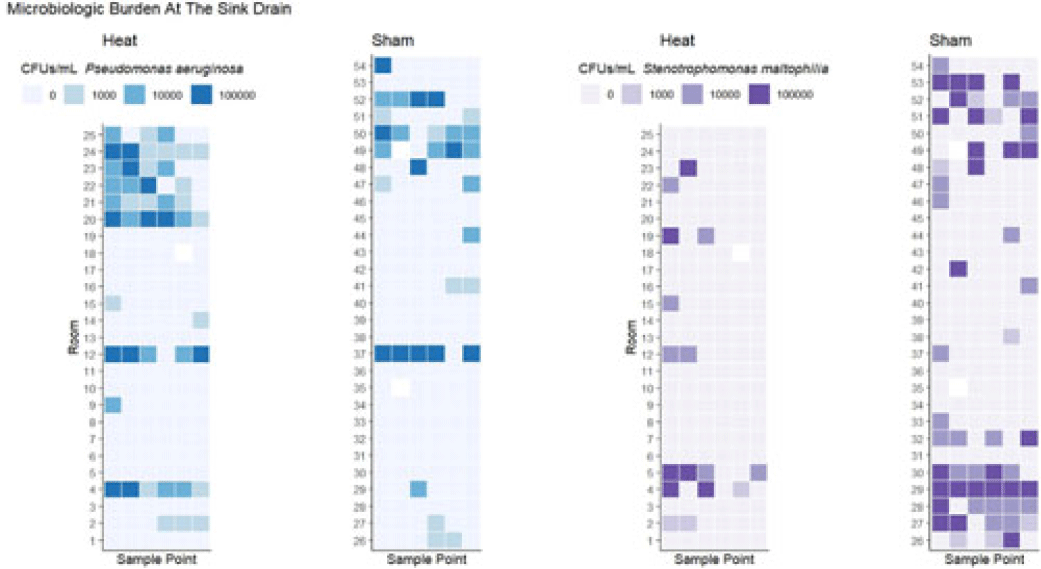
Background: Transmission of multidrug-resistant bacteria to patients from colonized hospital sink drains has prompted attempts to interrupt transmission through a variety of interventions directed at the wastewater environment. We previously found that use of a heating device designed to disrupt biofilm formation between the P trap and the sink drain, which is the major point of dispersal of bacteria to the patient-care environment, was associated with reduced risk of detectable gram-negative organisms on hospital sink drains. However, there was no observed effect on some important pathogens, including Pseudomonas aeruginosa and Stenotrophomonas maltophilia. We hypothesized that heating to a higher temperature would provide additional efficacy in preventing drain colonization. Methods: As part of a previous randomized study, 54 tailpiece heaters were installed in 3 intensive care units in an academic hospital and 2 acute-care units in an associated regional hospital; half of these devices were shams (ie, no heat). The devices were programmed to heat for 1 hour every fourth hour. Prior to this study, a device update increased the heating temperature (during the previous study the median heated temperature was 65.9°C). Sink drains and P traps were sampled monthly. Samples were assessed for semiquantitative growth of gram-negative bacteria on MacConkey agar, looking especially for P. aeruginosa and S. maltophilia. Frontline personnel were blinded to device assignment. Results: The mean heated temperature reached was 74.4°C. Based on proportional odds logistic regression (wherein the odds ratio reflects the likelihood of a given sample falling in a lower microbiologic burden level versus the levels above it), the heating device was associated with increased likelihood of lower microbiologic burden at the drain level for general growth on MacConkey agar (OR, 2.47; 95% CI, 1.11–5.51) and for growth of S. maltophilia (OR, 5.39; 95% CI, 2.20–13.18). The device did not have an effect on burden of Enterobacterales (OR, 1.38; 95% CI, 0.58–3.24). For P. aeruginosa, there was a trend toward decreased likelihood of lower microbiologic burden (OR, 0.41; 95% CI, 0.18–1.07) that did not reach statistical significance at the drain level, and the heating device was associated with decreased likelihood of lower microbiologic burden of P. aeruginosa at the P-trap level (OR, 0.20; 95% CI, 0.10–0.39). Conclusions: Heat disruption of biofilm between the P trap and sink may be a promising strategy for prevention of hospital sink drain colonization; however, the impact is variable across different bacterial species. Further understanding of the dynamics of the microbiome within wastewater is needed.
Disclosures: None

Hand Hygiene
Measuring hand hygiene opportunities per hour across two neonatal intensive care units
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s70-s71
-
- Article
-
- You have access
- Open access
- Export citation
-
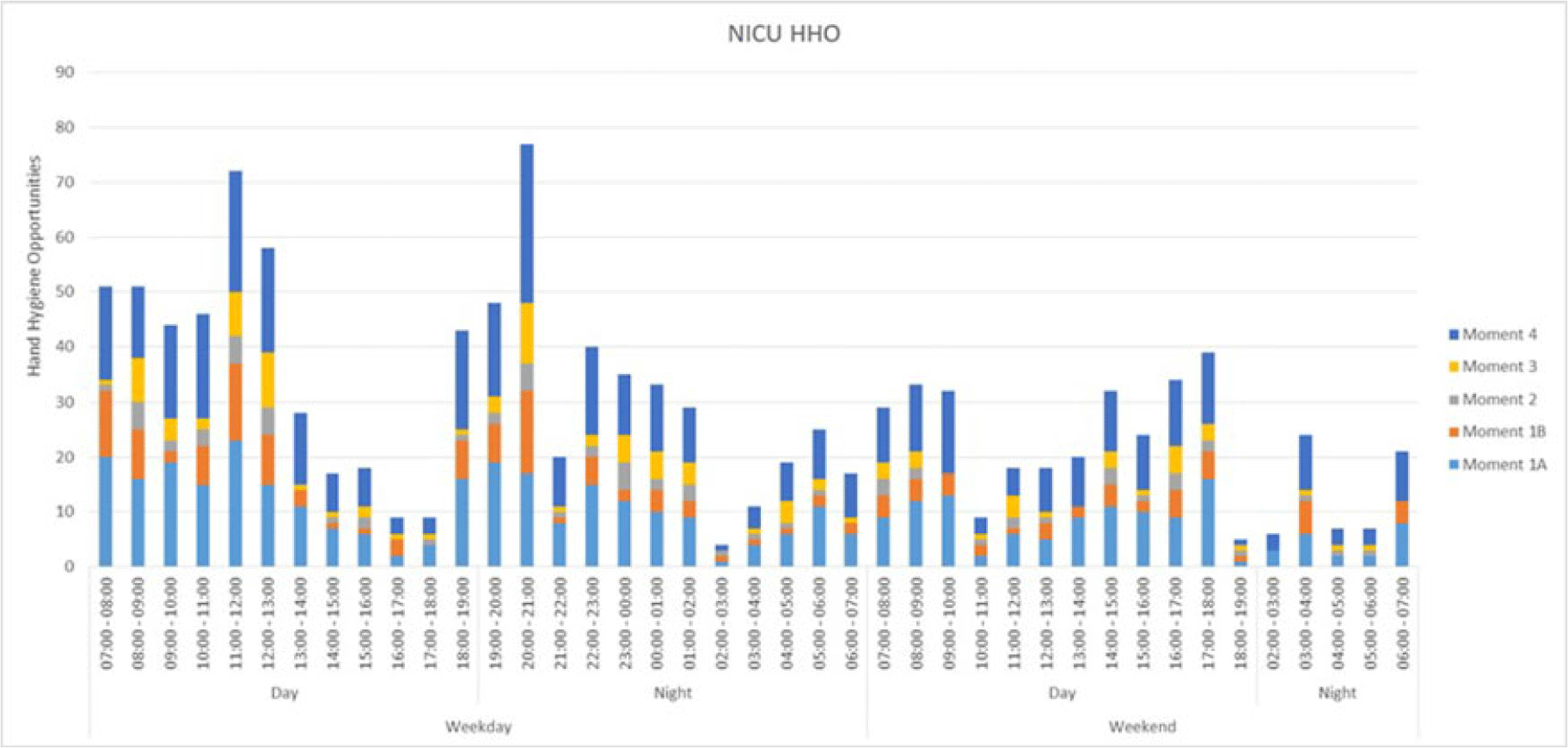
Background: To estimate hand hygiene compliance using electronic hand hygiene monitoring, the number of hand hygiene opportunities (HHOs) per period must be known in a given setting. Data on the number of HHOs in a neonatal ICU (NICU) are limited. We measured HHOs per hour and identified factors that may influence the number of HHOs per hour to calibrate compliance estimates for electronic hand hygiene monitoring. Methods: The study was conducted in 2 large NICUs in Ontario, Canada (72 and 42 beds, respectively). We centrally trained observers to identify HHOs using the Ontario-based “Four Moments of Hand Hygiene,” which is similar to combining moments 4 and 5 of the WHO “Five Moments of Hand Hygiene.” To apply the moments of hand hygiene to the NICU setting, the following modifications were made: moment 1 was entering the incubator or contact with anything within the ‘baby space’ directly around the incubator, and moment 4 was when hands exited the incubator and, as such, the ‘baby space.’ Using a standardized tool, the investigators conducted direct observation of HHOs during randomized observation periods from July 1, 2022, to January 9, 2023. In addition to HHOs, data on covariables potentially associated with the frequency of HHOs were collected: time and day of the week, acuity, additional precautions, corrected gestational age, and private versus multibed room or open pod. Results: We audited HHOs for 146 hours including 26 at site A and 120 at site B. Overall, 804 HHOs (69.2%) occurred during weekdays and 739 (63.6%) occurred during day shifts from 7:00 a.m. to7:00 p.m. The most frequent moments of hand hygiene were moment 1 (47.8%, before contact) and moment 4 (36.8%, after contact). The average numbers of HHOs were 7.8 per hour overall, 7.6 per hour on weekdays, 7.7 per hour on weekends, 8.8 per hour on day shifts, and 6.8 per hour on night shifts. The breakdown of HHOs by profession was 92.8% nurses, 0.6% physicians, 4.5% allied health, and 2.1% for others. Discussion: The rate of HHOs in NICU varied over a 24-hour period and was similar between 2 different NICUs. Evenings and weekends had considerably fewer average HHOs, and peaks were observed following nursing shift changes. The rate of HHOs may be influenced by other factors including unit design, patient acuity, and use of transmission-based precautions. Further analysis using a Poisson regression model will help to explore these factors and to calibrate electronic monitoring for this population.
Disclosures: None

Functional dependence as a contributing factor for patient hand contamination by multidrug-resistant organisms in acute care
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s71-s72
-
- Article
-
- You have access
- Open access
- Export citation
-
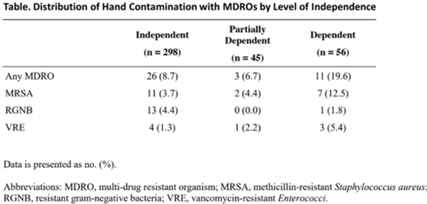
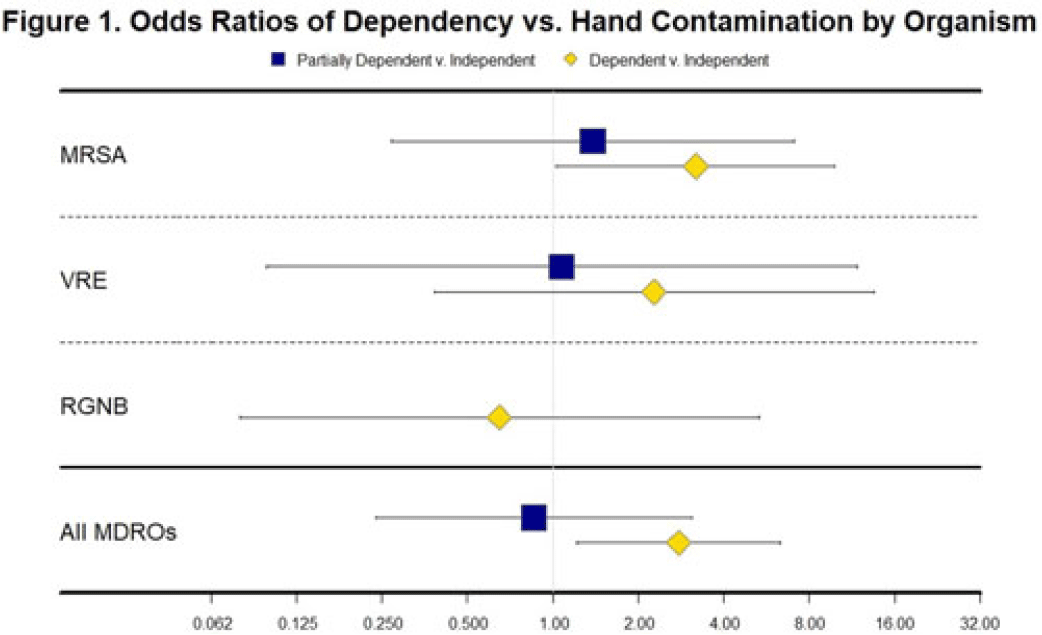
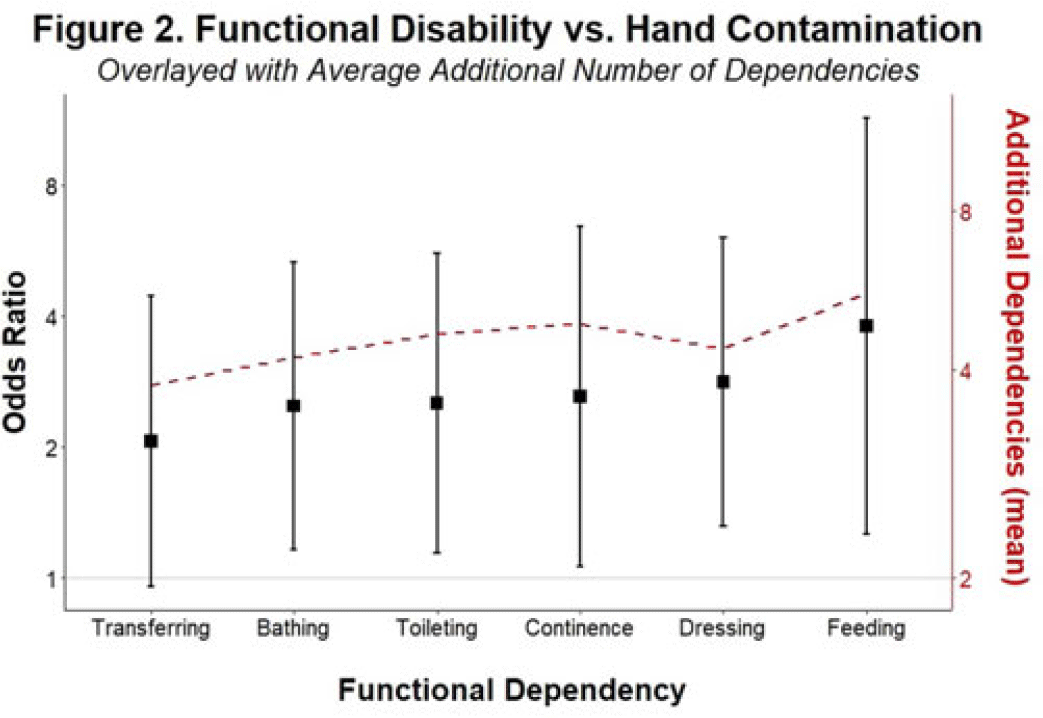
Background and objectives: Patients with functional disabilities are at higher risk of adverse outcomes, including infections. Although healthcare worker hand contamination has long been recognized as an important source of pathogen acquisition, the role of patient hands has been less clearly defined. We sought to determine whether the presence of functional disabilities is correlated with patient hand contamination by multidrug-resistant organisms (MDROs) and thus a potential target for patient hand hygiene (PHH) interventions. Methods: Case–control study of hand contamination with methicillin-resistant S. aureus, vancomycin-resistant enterococci, and gram-negative bacilli resistant to cephalosporins, fluoroquinolones, and/or carbapenems in 2 acute-care hospitals in southeastern Michigan. Cases (n = 40) and controls (n = 359) were defined as patients with or without hand contamination by MDROs, respectively. We assigned 3 exposure categories based on Katz activities of daily living scores: no functional disabilities (independent, reference group), 1–3 functional disabilities (partially dependent), and 4+ functional disabilities (dependent). We used stepwise logistic regression to identify confounding variables. Logistic regression was then used to establish the relationship between a patient’s functional dependence level and their hand contamination by MDROs. Results: The distribution of hand contamination of each target MDRO by level of patient dependence is shown in the Table. Overall, methicillin-resistant Staphylococcus aureus (MRSA) was the most represented, followed by resistant gram-negatives and vancomycin-resistant enterococci (VRE). Hospital site, sex, and history of MDROs were included in the model based on stepwise regression. The odds ratio (OR) of MRSA hand contamination in the dependent category was 3.19 (95% CI, 1.18–5.54) compared to the independent category, and for any MDRO the OR was 2.77 (95% CI, 1.22–6.32) (Fig. 1). The OR of MRSA hand contamination in the partially dependent category was 1.38 (95% CI, 0.27–7.07) compared to the independent group, and for any MDRO the OR was 0.86 (95% CI, 0.24–3.10) (Fig. 1). Feeding dependence had the highest single association with hand contamination (OR, 3.79, 95% CI, 1.26–11.43), with dressing dependence having the second highest association with hand contamination (OR, 2.82; 95% CI, 1.31–6.05) (Fig. 2). Conclusions: Patients with more functional dependencies were more likely to have MDRO hand contamination. This finding suggests a need for targeted PHH interventions in patients with functional disabilities to help prevent the spread of MDROs in the acute-care setting.
Disclosures: None



Addressing frontline healthcare worker perspectives on hand-hygiene monitoring badges
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s72
-
- Article
-
- You have access
- Open access
- Export citation
-
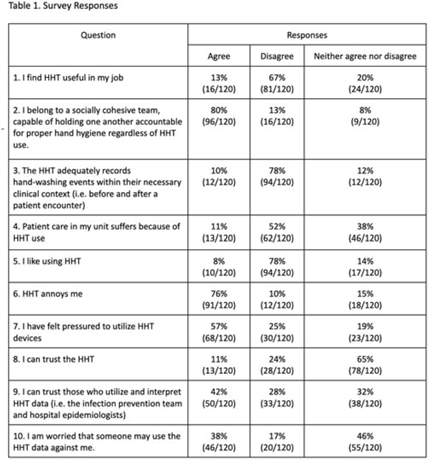
Background: Hand-hygiene technology (HHT) intends to monitor and promote hand washing by healthcare workers, a critical measure of infection control. Healthcare worker noncompliance with HHT is a major limitation to its implementation and utility in clinical settings. We assessed perspectives on HHT in an academic hospital system. Methods: Hand-hygiene team members created an anonymous, 37-question, Likert-scale survey to assess healthcare worker attitudes toward HHT. Surveys targeted nursing staff, advanced practice providers, care partners, and internal medicine physicians. Clinical coordinators from 5 distinct nursing units and 1 physician department emailed surveys to eligible employees. Research coordinators and clinical coordinators also posted a QR code for survey fliers at nursing stations. Results: Overall, 120 surveys were completed. Most surveys were completed by nurses and physicians (66.4% and 14.0%). Most respondents (67.5%) do not find HHT useful. Additionally, 78.3% of respondents believe that HHT does not accurately record hand-washing events. Most (78.3%) do not like using HHT, and 75.8% find it annoying. Only 10.8% believe that patient care suffers because of HHT. Conclusions: Most healthcare workers dislike the HHT badges, primarily due to perceived inaccuracies, lack of utility, burden of use, and pressure to comply. Distrust and effect on patient care do not appear to be substantial factors contributing to negative perceptions of HHT. Weaknesses of the study include overrepresentation of nursing staff and potential bias because respondents may have provided exceptionally negative responses believing it could lead to the removal of HHT.
Disclosures: None

Longitudinal effects of direct observation of hand hygiene practices and monitoring of alcohol-based handrub consumption
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s72-s73
-
- Article
-
- You have access
- Open access
- Export citation
Implementation Science
Factors associated with high influenza vaccination among healthcare workers in Tennessee acute-care hospitals, 2014–2022
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s73
-
- Article
-
- You have access
- Open access
- Export citation
Exploring the relationship between the reduction of floor microbial burden and the impact on healthcare-associated infections
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s73-s74
-
- Article
-
- You have access
- Open access
- Export citation
-
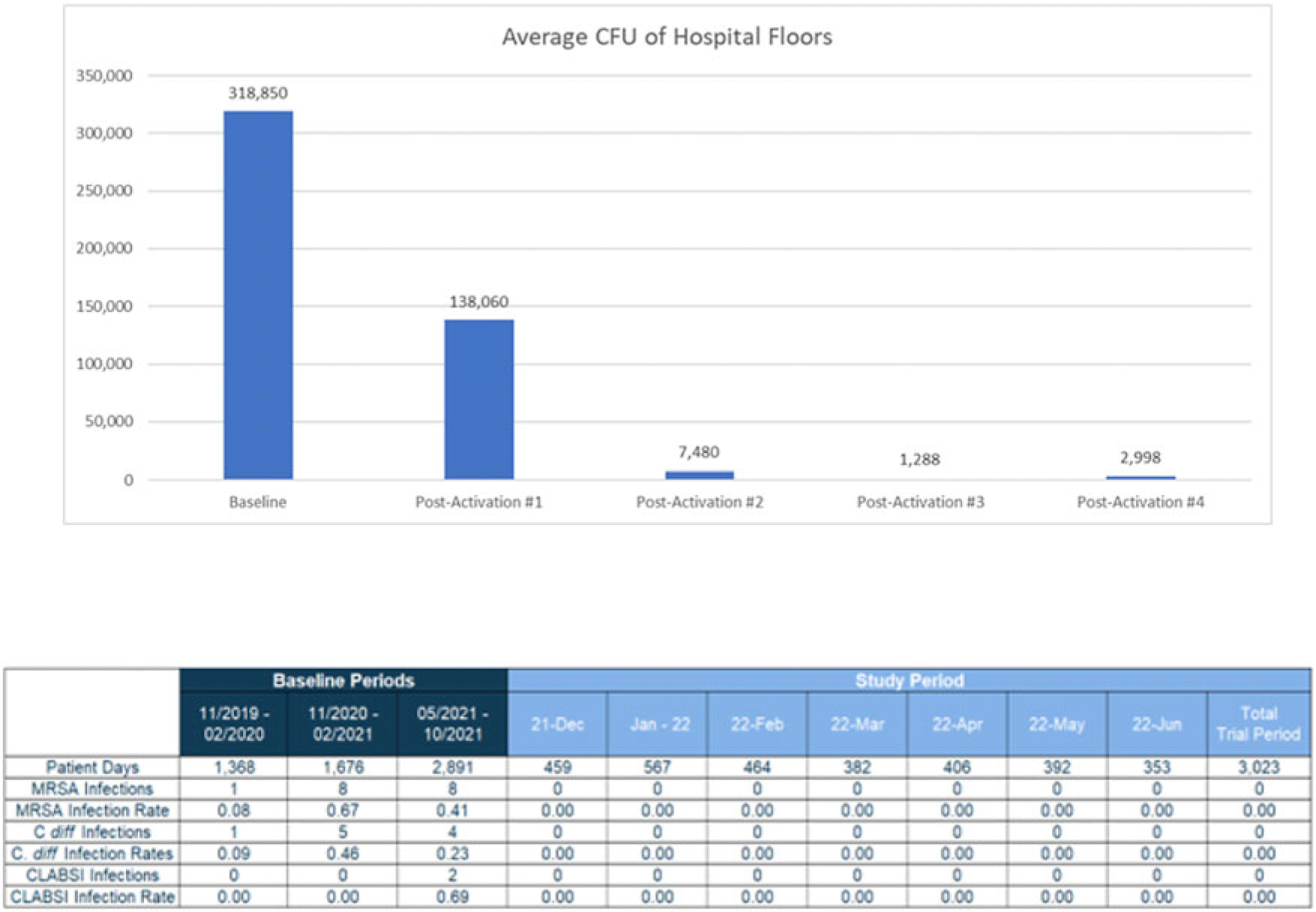
Background: Healthcare floors are a vehicle and/or source for potential pathogens that cause healthcare associated infections, and hospital floors are often heavily contaminated with pathogens such as Clostridioides difficile and methicillin-resistant Staphylococcus aureus. However, definitive research linking reductions in floor burden to reductions in HAIs has not yet been established. We sought to evaluate emerging technology for continuous disinfection and its potential impact on HAIs. This study was designed to explore the potential relationship between the reduction of microbial burden of floors and healthcare associated infections. Methods: A prospective study was conducted in a 22-bed medical-surgical intensive care unit in a 180-bed suburban hospital near New Orleans, Louisiana, from November 2021 to June 2022. Using sterile, premoistened sponges, samples were collected from the floors of 10 areas throughout the unit including 2 nurses’ stations, the physician charting area, and 7 patient rooms. The advanced photocatalytic oxidation (aPCO) equipment was then installed in the HVAC ductwork throughout the ICU and activated. Environmental surface sampling of the same floor surfaces was then repeated every 4 weeks for the first 5 months of the study. HAIs were also tracked throughout the entire study period. The facility’s normal cleaning floor protocols using a neutralizing floor cleaner were unchanged and followed during the study. Changes in surface burden were calculated using a repeated-methods ANOVA with post hoc analyses as appropriate. Rates of healthcare associated infections were compared using χ2 analyses. Results: Overall, there was a 99.6% statistically significant decrease in floor environmental surface burden from the baseline to the final postactivation test (Fig. 1). The average colony forming unit count (CFU) decreased from 318,850 CFU per 100 cm2 to just 2,988 CFU per 100 cm2. The unit also saw a statistically significant decrease in publicly reported healthcare associated infections (HO-MRSA, CLABSI, HO-CDI) during the study period compared to the same period a year prior and in the 6 months immediately prior to the beginning of the study (Fig. 2). Conclusions: Advanced photocatalytic oxidation technology resulted in a reduction of microbial burden on the floors of a high-traffic intensive care unit. Statistically significant decreases in healthcare-associated infections was also seen. This study highlights a novel aPCO technology and its efficacy at reducing microbial burden and healthcare-associated infections despite no change in practice.
Disclosures: None

Comparison of a standard environmental surface sampling method and a composite approach for select healthcare pathogens
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s74
-
- Article
-
- You have access
- Open access
- Export citation
Infection Control in Low and Middle-Income Countries
Infection prevention and control perspective and practices among healthcare workers in Bangladesh: A multicenter cross section
-
- Published online by Cambridge University Press:
- 29 September 2023, pp. s74-s75
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Infection prevention and control (IPC) is a critical feature of preventing the spread of healthcare-associated infections (HAIs) in hospitals. IPC practices are particularly important in resource-constrained and crowded hospital settings. The successful implementation of infection prevention measures depends on healthcare worker (HCW) knowledge of, attitude toward, and practice (KAP) of IPC. In this project, we assessed the KAP of HCWs and identified factors associated with IPC compliance at tertiary-care hospitals in Bangladesh. Methods: From September 2020 to January 2021, we conducted this hospital-based cross-sectional assessment at 11 tertiary-care hospitals. A semistructured questionnaire was used to conduct face-to-face interviews with physicians, nurses, and cleaning staff who were directly involved in patient care. Based on >75% of the total score, each KAP component was divided into adequate knowledge, favorable attitude, and safe practice. We performed descriptive analysis and multivariate logistic regression to determine the KAP score and associated factors influencing IPC compliance in hospital settings. Results: In total, 1,728 HCWs were interviewed; 76.8% of the participants had adequate knowledge on IPC and 54.6% reported safe practices. However, only 16.2% of HCWs had a favorable attitude toward IPC. Among the 3 HCW groups, nurses had the highest KAP scores (76.07±12.7) followed by physicians (69.8±16.2), and cleaning staff (34.4±27.3). Only 29.2% of HCWs reported having received IPC training, and they cited heavy workload as a barrier to IPC guideline adherence. HCWs having adequate knowledge showed 9 times higher odds of safe IPC practice (AOR, 9.36; 95% CI, 5.47–16.04). HCWs who had a favorable attitude toward IPC were 16 times as likely to perform safe practice toward IPC activities (AOR, 15.5; 95% CI, 10.27–23.42). Conclusions: Knowledge of safe practices and having a favorable attitude toward IPC are key components of a successful IPC program. Significant improvements are required among all levels of HCWs in Bangladesh tertiary-care hospitals, especially cleaning staff. Educational interventions to train on IPC guidelines, plus monitoring, could improve HCW safe practices.
Disclosures: None


Infection Control in Low- and Middle-Income Countries
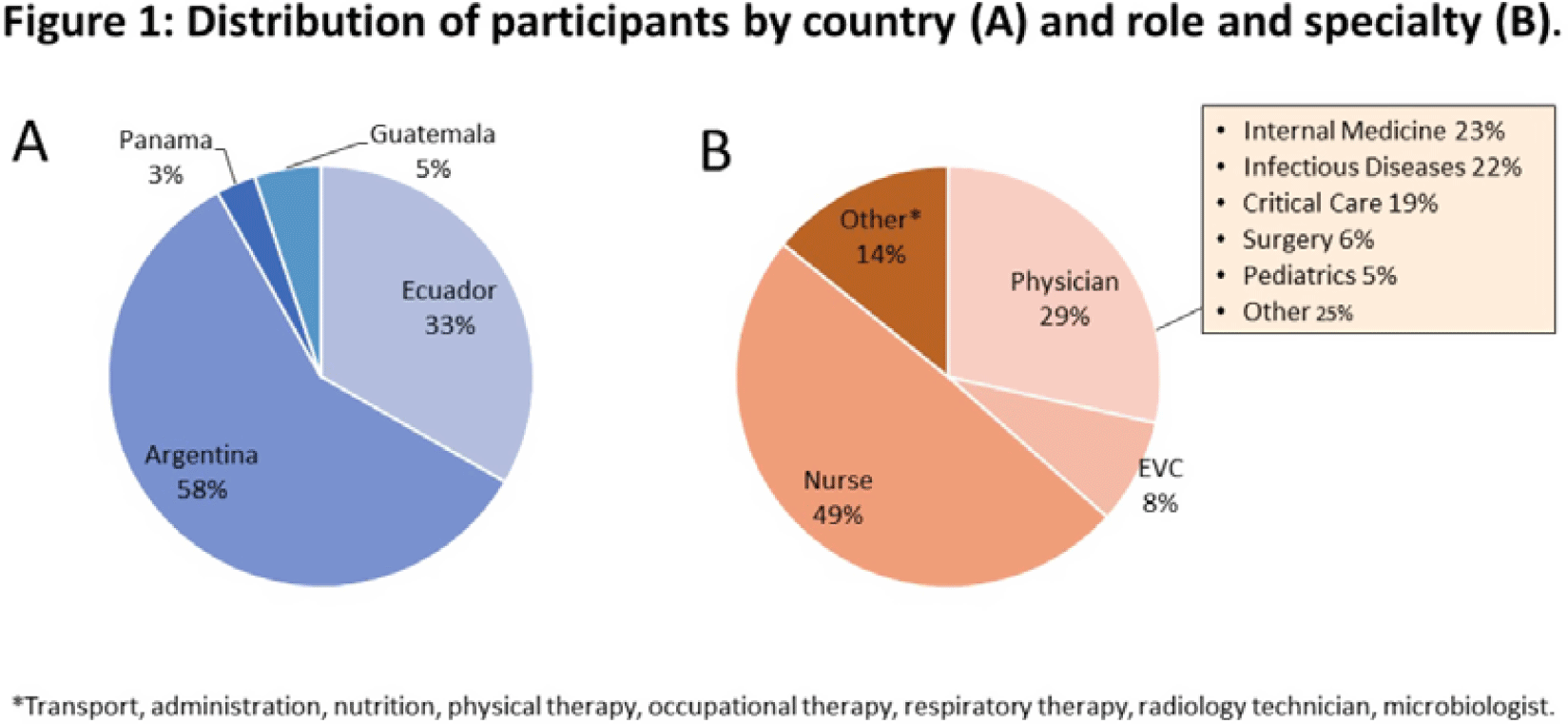
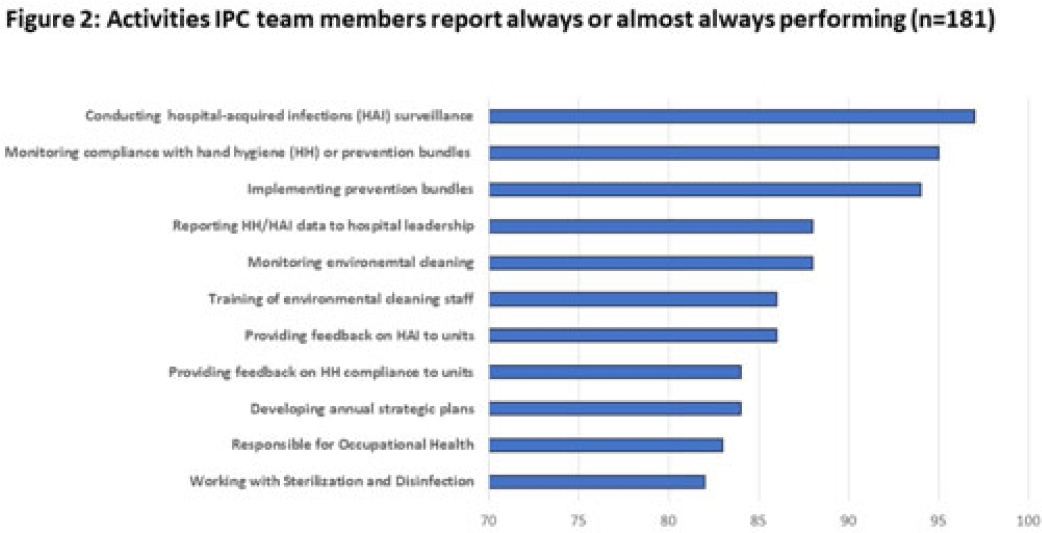
Healthcare worker perceptions about infection prevention and control processes and practices in Latin America
-
- Published online by Cambridge University Press:
- 29 September 2023, p. s75
-
- Article
-
- You have access
- Open access
- Export citation