
6 results
Implementing nasal povidone-iodine decolonization to reduce infections in hemodialysis units: a qualitative assessment
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 23 May 2024, pp. 1-6
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
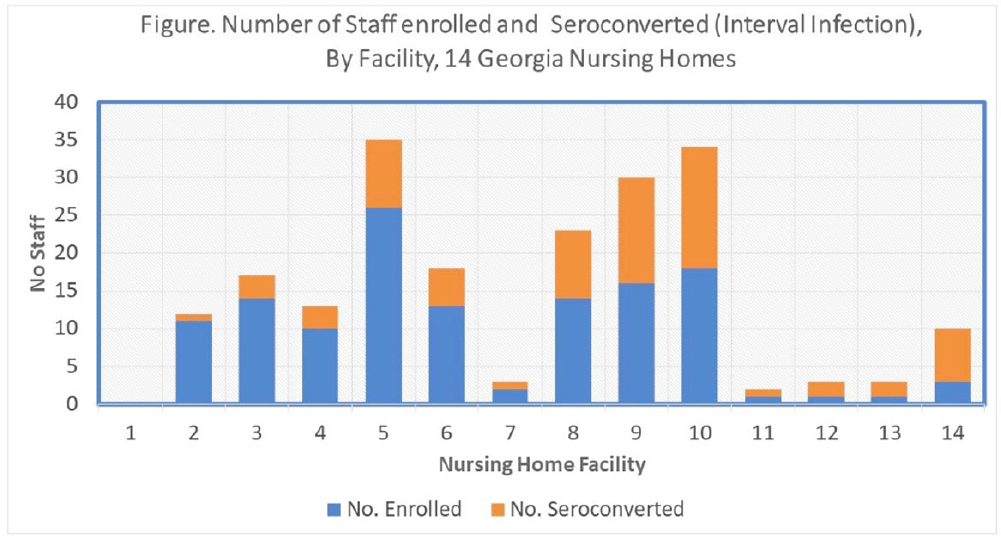
Which nursing home workers were at highest risk for SARS-CoV-2 infection during the November 2020–February 2021 winter surge of COVID-1?
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s7
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Nursing home (NH) residents and staff were at high risk for COVID-19 early in the pandemic; several studies estimated seroprevalence of infection in NH staff to be 3-fold higher among CNAs and nurses compared to other staff. Risk mitigation added in Fall 2020 included systematic testing of residents and staff (and furlough if positive) to reduce transmission risk. We estimated risks for SARS-CoV-2 infection among NH staff during the first winter surge before widespread vaccination. Methods: Between February and May 2021, voluntary serologic testing was performed on NH staff who were seronegative for SARS-CoV-2 in late Fall 2020 (during a previous serology study at 14 Georgia NHs). An exposure assessment at the second time point covered prior 3 months of job activities, community exposures, and self-reported COVID-19 vaccination, including very recent vaccination (≤4 weeks). Risk factors for seroconversion were estimated by job type using multivariable logistic regression, accounting for interval community-incidence and interval change in resident infections per bed. Results: Among 203 eligible staff, 72 (35.5%) had evidence of interval seroconversion (Fig. 1). Among 80 unvaccinated staff, interval infection was significantly higher among CNAs and nurses (aOR, 4.9; 95% CI, 1.4–20.7) than other staff, after adjusting for race and interval community incidence and facility infections. This risk persisted but was attenuated when utilizing the full study cohort including those with very recent vaccination (aOR, 1.8; 95% CI, 0.9–3.7). Conclusions: Midway through the first year of the pandemic, NH staff with close or common resident contact continued to be at increased risk for infection despite enhanced infection prevention efforts. Mitigation strategies, prior to vaccination, did not eliminate occupational risk for infection. Vaccine utilization is critical to eliminate occupational risk among frontline healthcare providers.
Funding: None
Disclosures: None

Risk factors for severe acute respiratory coronavirus virus 2 (SARS-CoV-2) seropositivity among nursing home staff
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 28 October 2021, e35
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Evaluation of Care Interactions Between Healthcare Personnel and Residents in Nursing Homes Across the United States
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s36-s38
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
The Last Interglacial Ocean
-
- Journal:
- Quaternary Research / Volume 21 / Issue 2 / February 1984
- Published online by Cambridge University Press:
- 20 January 2017, pp. 123-224
-
- Article
- Export citation
Preparing Emergency Physicians for Acute Disaster Response: A Review of Current Training Opportunities in the US
-
- Journal:
- Prehospital and Disaster Medicine / Volume 31 / Issue 6 / December 2016
- Published online by Cambridge University Press:
- 19 September 2016, pp. 643-647
- Print publication:
- December 2016
-
- Article
- Export citation
