Contents
Original Research
Health Care Implications of Terrorist Attacks in South Asia
-
- Published online by Cambridge University Press:
- 13 April 2022, pp. 338-342
-
- Article
- Export citation
Weighty Matters: A Real-World Comparison of the Handtevy and Broselow Methods of Prehospital Weight Estimation
-
- Published online by Cambridge University Press:
- 13 September 2022, pp. 616-624
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
An Epidemiological Analysis of Terrorism-Related Attacks in Eastern Europe from 1970 to 2019
-
- Published online by Cambridge University Press:
- 02 June 2022, pp. 468-473
-
- Article
- Export citation
Meeting Abstracts
Establishing a National Emergency Medical Team (EMT) in Papua New Guinea (PNG)
-
- Published online by Cambridge University Press:
- 22 November 2022, p. s59
-
- Article
-
- You have access
- Export citation
Original Research
A Counter-Terrorism Medicine Analysis of Drone Attacks
-
- Published online by Cambridge University Press:
- 31 January 2022, pp. 192-196
-
- Article
- Export citation
Maintaining Prehospital Intubation Success with COVID-19 Personal Protective Precautions
-
- Published online by Cambridge University Press:
- 12 September 2022, pp. 783-787
-
- Article
- Export citation
A New Quantitative Triage System for Hospitalized Neonates to Assist with Decisions of Hospital Evacuation Priorities
-
- Published online by Cambridge University Press:
- 07 April 2022, pp. 343-349
-
- Article
- Export citation
Impact of Specific Emergency Measures on Survival in Out-of-Hospital Traumatic Cardiac Arrest
-
- Published online by Cambridge University Press:
- 17 December 2021, pp. 51-56
-
- Article
- Export citation
Comparison of End-Tidal Carbon Dioxide (ETCO2) Gradient and Vena Cava Collapsibility Index (VCCI) in Response to Intravenous Fluid Therapy in Patients with Moderate and Severe Dehydration and Acute Gastroenteritis
-
- Published online by Cambridge University Press:
- 25 May 2022, pp. 474-479
-
- Article
- Export citation
Needle Cricothyroidotomy by Intensive Care Paramedics
-
- Published online by Cambridge University Press:
- 12 August 2022, pp. 625-629
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Learning Success and Influencing Factors in Out-of-Hospital Placement of Intravenous Catheters
-
- Published online by Cambridge University Press:
- 26 September 2022, pp. 788-793
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Manual versus Mechanical Delivery of High-Quality Cardiopulmonary Resuscitation on a River-Based Fire Rescue Boat
-
- Published online by Cambridge University Press:
- 25 July 2022, pp. 630-637
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Smart Glasses: A New Tool for Assessing the Number of Patients in Mass-Casualty Incidents
-
- Published online by Cambridge University Press:
- 27 June 2022, pp. 480-484
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Iatrogenic Tracheal Rupture Related to Prehospital Emergency Intubation in Adults: A 15-Year Single Center Experience
-
- Published online by Cambridge University Press:
- 11 January 2022, pp. 57-64
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Logistic Red Flags in Mass-Casualty Incidents and Disasters: A Problem-Based Approach
-
- Published online by Cambridge University Press:
- 03 February 2022, pp. 197-204
-
- Article
- Export citation
Meeting Abstracts
Building COVID-19 Capacity with a Simple Tool – “POP-O-MOP” in the Pacific
-
- Published online by Cambridge University Press:
- 22 November 2022, p. s60
-
- Article
-
- You have access
- Export citation
Original Research
The Natural History of Stingray Injuries
-
- Published online by Cambridge University Press:
- 08 April 2022, pp. 350-354
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Emergency Medical Teams’ Responses during the West Japan Heavy Rain 2018: J-SPEED Data Analysis
-
- Published online by Cambridge University Press:
- 28 February 2022, pp. 205-211
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
The Utilization of Handheld Ultrasound Devices in a Prehospital Setting
-
- Published online by Cambridge University Press:
- 18 April 2022, pp. 355-359
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Meeting Abstracts
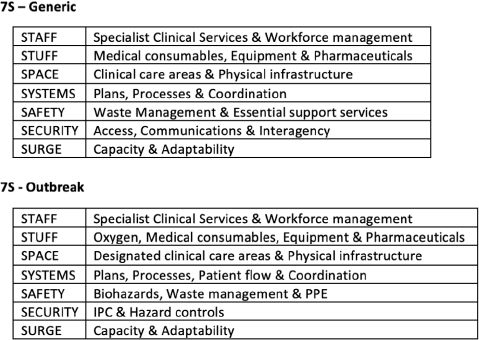
Mapping Acute Care Systems’ Surge Capacity and Response Priorities – the ‘7S’ Framework Tool
-
- Published online by Cambridge University Press:
- 22 November 2022, p. s61
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
During health emergencies, significant disruptions occur concurrently within critical components of acute care systems such as workforce, medical supplies, clinical workflows, patient care pathways, and hospital essential support services. The ability to map both existing and surge capacities across the acute care health system is a complex, nuanced, and often lengthy process which is heavily dependent upon localized knowledge applied in specific, individual contexts.
Objectives:Outline an innovative, “All Hazards” tool developed through a standardized framework approach to rapidly and consistently identify, assess, and prioritize key system-wide health capacity indicators in acute care hospital settings during health emergencies.
Method/Description:Initially designed as a health systems preparedness and planning tool for use in sudden-onset disasters in 2017, the “7S” framework has been successfully applied during recent AUSMAT outbreak emergency responses to assist local Ministries of Health to effectively identify, articulate, rationalize, and prioritize clinical and operational health response priorities.
Results/Outcomes:Multiple operational health leaders found the “7S” framework valuable in efficiently managing both the assessment of and priority allocation of resources in health systems under duress. The tool was simple to understand and explain, time efficient, and comprehensive. Additionally, the tool provided an effective structure for communicating with local health and response leaders.
Conclusion:The “7S” framework has demonstrated excellent utility as a highly effective and scalable, locally adapted “All Hazards” tool for use during health planning, preparedness, and acute care response phases in diverse health emergencies contexts.