
Contents
Abstract
426 - FindMyApps: Protocol for a randomized controlled trial with community-dwelling people with dementia, evaluating the effectiveness and cost-effectiveness of an intervention to improve self-management and social participation
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 142
-
- Article
-
- You have access
- Export citation
427 - HARMONY study: pimavanserin significantly reduces risk of relapse of dementia-related psychosis
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 143
-
- Article
-
- You have access
- Export citation
428 - DEMENTIA INPATIENT THERAPEUTIC INTERVENTIONS IN A SCOTTISH HEALTH REGION
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 144
-
- Article
-
- You have access
- Export citation
429 - Relationship between agitation and social isolation as a dimension of quality of life in residents with dementia living in German nursing homes – a secondary data analysis
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 145
-
- Article
-
- You have access
- Export citation
430 - The Puzzled and Puzzling Self: Self-Perception of People With Dementia in the Residential Care Homes of Hong Kong
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 146
-
- Article
-
- You have access
- Export citation
431 - DEMENTIA IN PRIMARY CARE AND DOCTOR-PATIENT-CARER INTERACTIONS: PRELIMINARY FINDINGS
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 147
-
- Article
-
- You have access
- Export citation
432 – Correlation between regional brain volume and olfactory function in very mild amnestic patients
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 148
-
- Article
-
- You have access
- Export citation
433 - Burden of Disease Associated with Dementia-related Psychosis and Dementia-related Agitation & Aggression Using a National Long-term Care US Database
-
- Published online by Cambridge University Press:
- 04 November 2020, pp. 149-150
-
- Article
-
- You have access
- Export citation
434 - Treatment Patterns and Needs for Dementia-related Psychosis Described by Patients and Care Partners (Caregivers): an Observational, Prospective Study to Describe the Patient Experience
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 151
-
- Article
-
- You have access
- Export citation
435 - Perspectives of the general public on dementia risk reduction (DRR) and implications for implementation: a qualitative evidence synthesis
-
- Published online by Cambridge University Press:
- 04 November 2020, pp. 152-153
-
- Article
-
- You have access
- Export citation
437 - COGNITIVE, PATHOLOGICAL, GENETIC AND NEURO-RADIOLOGICAL CORRELATES OF CEREBRAL AMYLOID ANGIOPATHY
-
- Published online by Cambridge University Press:
- 04 November 2020, pp. 154-155
-
- Article
-
- You have access
- Export citation
438 - Nigerian women are more susceptible to the impact of diabetes-and-dementia: State-of-art, Future perspectives and Directions
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 156
-
- Article
-
- You have access
- Export citation
439 - Sex-dependent increase of cerebral blood flow in cortex and hippocampus as a compensatory mechanism in end-of-life dementia: A MRI-ASL translational approach in models of normal and pathological aging
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 157
-
- Article
-
- You have access
- Export citation
440 - Dementia villages: rethinking dementia care
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 158
-
- Article
-
- You have access
- Export citation
441 - Treatment adequacy for depression and anxiety disorders affects quality of life in older adults consulting in primary care
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 159
-
- Article
-
- You have access
- Export citation
442 - Neurocognitive markers of passive suicidal ideation in late life depression
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 160
-
- Article
-
- You have access
- Export citation
443 - Measuring frailty in older psychiatric patients
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 161
-
- Article
-
- You have access
- Export citation
444 - A Picture is worth a thousand words! Adventure beyond the MMSE
-
- Published online by Cambridge University Press:
- 04 November 2020, p. 162
-
- Article
-
- You have access
- Export citation
445 - The factors associated with the presence of psychotic symptoms in the HELIAD Greek community study of older adults
-
- Published online by Cambridge University Press:
- 04 November 2020, pp. 163-164
-
- Article
-
- You have access
- Export citation
446 - Persistent Delusional Disorder (Late Paraphrenia) - An innovative and cost effective clinical model in the community by older adult‘s mental health crisis and home treatment team
-
- Published online by Cambridge University Press:
- 04 November 2020, pp. 165-166
-
- Article
-
- You have access
- Export citation
-
Aims
To review the various available clinical models of care delivery for patients with persistent delusional disorder (PDD) in community and economically evaluate the REACT model of safe care delivery- REACT’s Assertive and Prudent- Model of Safe Care (RAP–MoSC).
MethodsREACT (Response Enhanced Assessment Crisis and Home Treatment Team) is the only bespoke crisis and home treatment team for older adults with mental health problems in the whole of Wales available only for the residents of Cardiff and Vale of Glamorgan through Cardiff and Vale University Health Board..
It was set up on 28 February 2012. The cases of PDD in REACT service since its inception to 31 Dec 2016 were studied in relation to the assertive and prudent health care model. The economic evaluation of this service model for PDD patients was studied in detail.
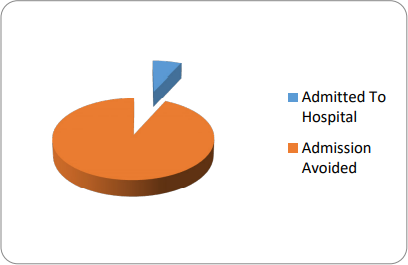
Results of the studyThe RAP-MoSC model is economically effective in avoiding patients getting admitted to hospital under Mental Health Act by managing them safely in the community.
During the period between 28 February 2012 and 31 December 2016 there were 44 patients with a diagnosis of PDD in REACT’s case load. Only 3 patients got admitted to mental health assessment ward with the average length of stay period of 120 days. 41 patients were safely managed in the community with REACT with an average length of stay period of 21 days in REACT.
A PDD patient will cost NHS £21,000 if admitted to a mental health bed. If the patient is managed in the community with RAP-MoSC model of care the cost will be £1533.
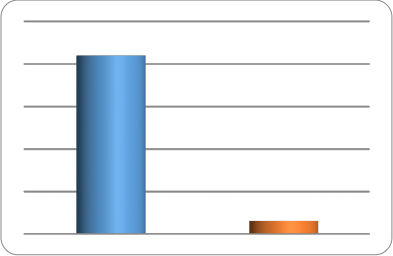
REACT saved £793,548 by avoiding 41 PDD patients being admitted into hospital during an episode of delusional intensification in the period February 2012 to December 2016. PDD patients need under the RAP-MoSC model a bespoke MDT approach with better communication between secondary mental health and primary care services. Assertive and Prudent Clinical leadership is needed to sustain the RAP-MoSC in the community. Clinical reflections of this model of care will be presented in the conference.
ConclusionsOn reflection REACT found that the key points in working with PDD are;
Using a ‘foot in the door approach’
Mental health professionals introducing themselves as Health professionals
Remote prescribing

