
Contents
Poster Presentation
Antibiotic Stewardship
Prospective Audit for Antimicrobial Use and Stewardship Practices in Intensive Care Unit at a Tertiary-Care Center in India
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s40
-
- Article
-
- You have access
- Open access
- Export citation
-
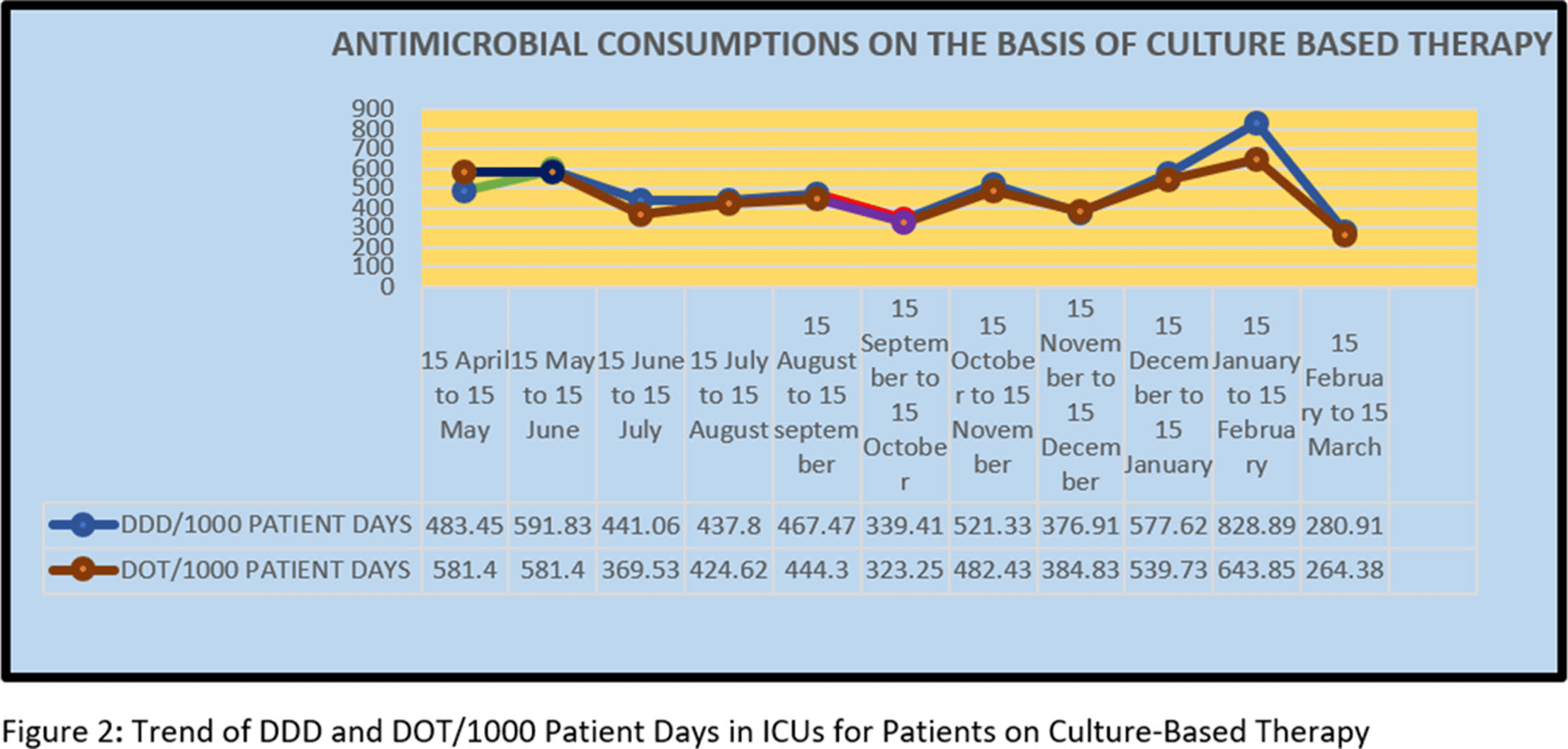
Background: Antimicrobial decision making in the ICU is challenging. Injudicious use of antimicrobials contributes to the development of resistant pathogens and drug-related adverse events. However, inadequate antimicrobial therapy is associated with mortality in critically ill patients. Antimicrobial stewardship programs are increasingly being implemented to improve prescribing. Methods: This prospective study was conducted over 11 months, during which the pharmacist used a standardized survey form to collect data on antibiotic use. Evaluation of antimicrobial use and stewardship practices in a 12-bed polytrauma ICU and a 20-bed neurosurgery ICU of the 248-bed AIIMS Trauma Center in Delhi, India. Antimicrobial consumption was measured using WHO-recommended defined daily dose (DDD) of given antimicrobials and days of therapy (DOT). Results: Antibiotics were ranked by frequency of use over the 11-month period based on empirical therapy and culture-based therapy. The 11-month DDD and DOT averages when empiric antibiotics were used were 532 of 1,000 patient days and 484 per 1,000 patient days, respectively (Figure 1). When cultures were available, DDD was 486 per 1,000 patient days and DOT was 442 per 1,000 patient days (Figure). Conclusions: The quantity and frequency of antibiotics used in the ICUs allowed the AMSP to identify areas to optimize antibiotic use such as educational initiatives, early specimen collection, and audit and feedback opportunities.
Funding: No
Disclosures: None
Figure 1.
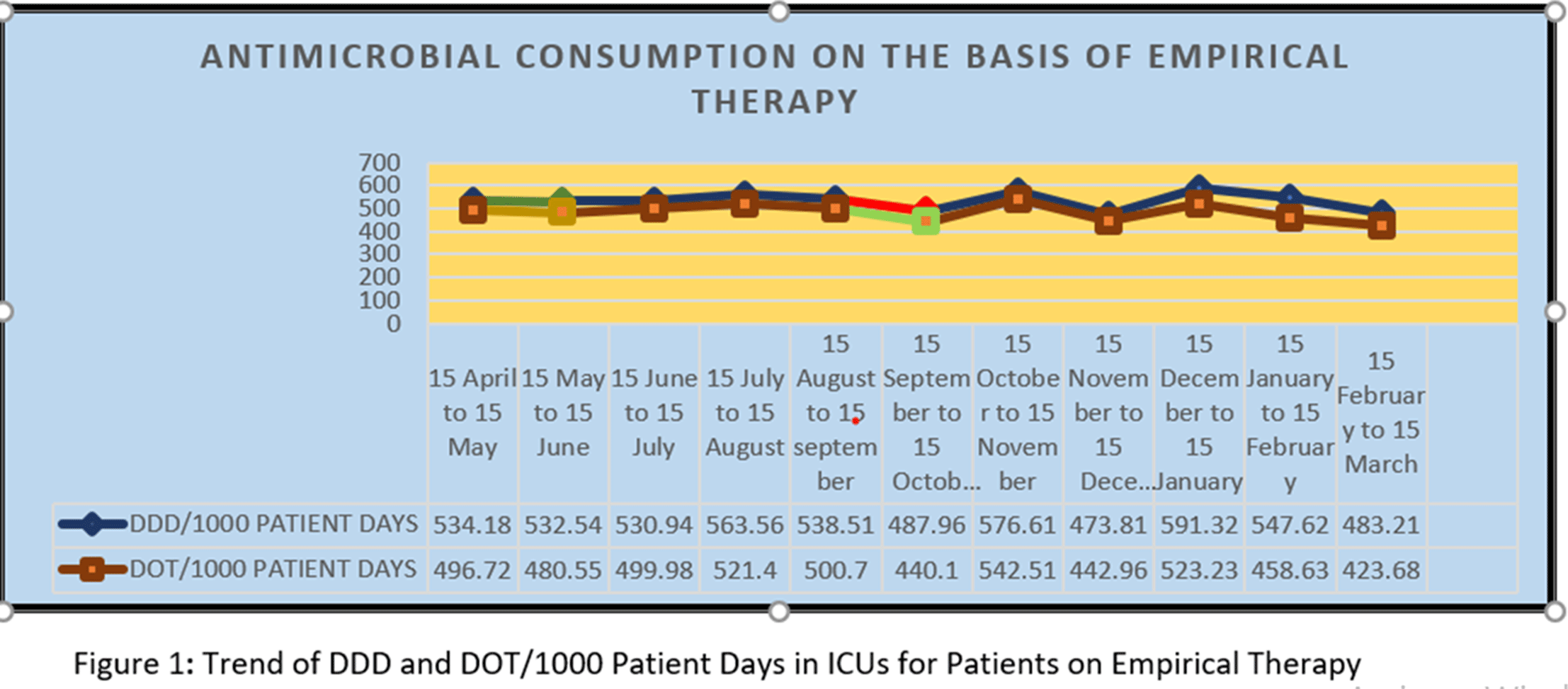
Figure 2.


Evaluating the Prevalence of Leading Practices in Antimicrobial Stewardship
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s41
-
- Article
-
- You have access
- Open access
- Export citation
C. difficile
Clostridioides difficile Is Not Difficult to Predict in Hospital Settings
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s41
-
- Article
-
- You have access
- Open access
- Export citation
Clinical Characteristics and Fecal Microbiome in Recurrent Versus Nonrecurrent Clostridioides difficile Infection
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s41-s42
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Up to 30% of patients with Clostridioides difficile infection (CDI) develop recurrent infection, which is associated with a 33% increased risk of mortality at 180 days. The gut microbiome plays a key role in initial and recurrent episodes of CDI. We examined the clinical characteristics and gut microbial diversity in patients with recurrent (rCDI) versus nonrecurrent CDI at a tertiary-care academic medical center. Methods: Stool samples were collected from 113 patients diagnosed with CDI between 2018 and 2019. Clinical and demographic data were extracted from the electronic medical record (Table 1), and 16S rRNA sequencing of the v4 region was carried out on the Illumina MiSeq using 2×250 paired-end reads. Sequences were binned into operational taxonomic units (OTUs) using mothur and were classified to the genus level whenever possible using the ribosomal database project data set version 16. Alpha diversity was calculated using the Shannon diversity index. Β diversity was calculated using the Bray-Curtis dissimilarity matrix. Differential abundance testing was done using DESeq to assess taxonomic differences between groups. A P value of .05 was used to assess significance. Results: In total, 55 patients had rCDI (prior positive C. difficile polymerase chain reaction in last 7–365 days) and 58 had nonrecurrent CDI (Table 1). Patients with rCDI had a higher frequency of organ transplant and comorbidity. No differences in α not β diversity were observed between groups. Also, 4 OTUs were more abundant in those with rCDI: Ruminococcus (n = 2), Odoribacter, and Lactobacillus. Patients with rCDI had microbiomes with greater proportions of Bacteroidetes (27% of OTUs) compared to the nonrecurrent group (18%) as well as fewer OTUs belonging to the Firmicutes phyla compared to the nonrecurrent patients (56% vs 59%). Among the rCDI patients, those experiencing 2 or more recurrences had greater abundances of Bacteroides and Ruminococcus, while those experiencing only 1 recurrence had significantly greater abundances of Akkermensia, Ruminococcus, Streptococcus, Roseburia, Clostridium IV, and Collinsella compared to those with only 1 recurrence (Table 2). Conclusions: Patients with rCDI had a more impaired microbiome than those with initial CDI. Ruminococcus OTUs have been previously indicated as a risk factor for recurrence and treatment failure, and they were significantly more abundant in those with rCDI and among those with multiple recurrences. The greatest differences in the microbiome were observed between those with 1 recurrence compared to those with multiple recurrences. Interventions for gut microbiome restoration should focus particularly on those with recurrent CDI.
Funding: No
Disclosures: None
Table 1. 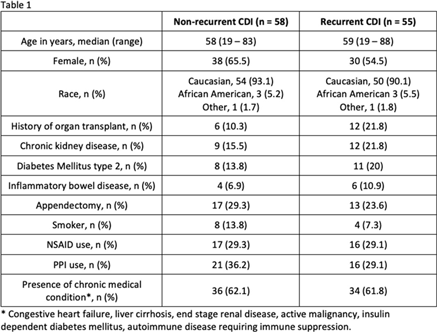
Table 2. 


Impact of Two-Step Testing Algorithm on Reducing Hospital-Onset Clostridioides difficile Infections
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s42-s43
-
- Article
-
- You have access
- Open access
- Export citation
-
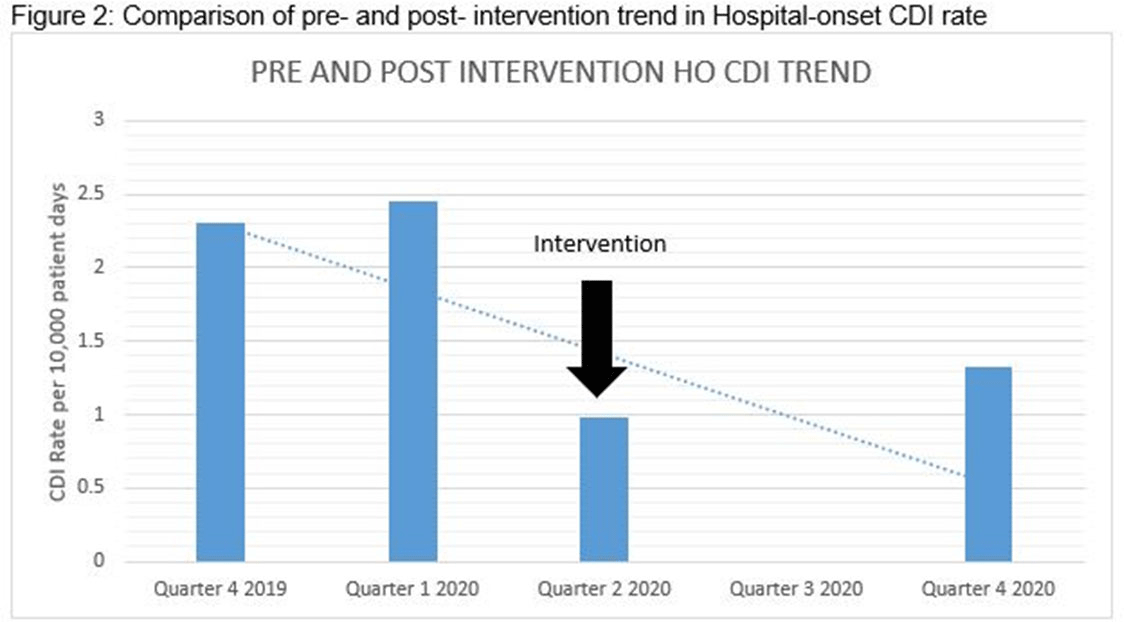
Clostridioides difficile infection (CDI) is one of the leading causes of hospital–onset infections. Clinically distinguishing true CDI versus colonization with C. difficile is challenging and often requires reliable and rapid molecular testing methods. At our academic center, we implemented a 2-step testing algorithm to help identify true CDI cases. The University of Mississippi Medical Center is a 700+ bed academic facility located in Jackson, Mississippi. Hospital-onset (HO) CDI was defined based on NHSN Laboratory Identified (LabID) event as the last positive C. difficile test result performed on a specimen using a multistep testing algorithm collected >3 calendar days after admission to the facility. HO-CDI data were collected from all inpatient units except the NICU and newborn nursery. HO-CDI outcomes were assessed based on standardized infection ratio (SIR) data. In May 2020, we implemented a 2-step testing algorithm (Figure 1). All patients with diarrhea underwent C. difficile PCR testing. Those with positive C. difficile PCR test were reflexed to undergo enzyme immunoassay (EIA) glutamate dehydrogenase antigen (Ag) testing and toxin A and B testing. The final results were reported as colonization (C. difficile PCR+/EIA Ag+/Toxin A/B−) or true CDI case (C. difficile PCR+/EIA +/Toxin A/B +) or negative (C. difficile PCR−). All patients with colonization or true infection were placed under contact isolation precautions until diarrhea resolution for 48 hours. During the preintervention period (October 2019–April 2020), 25 HO-CDI cases were reported compared to 8 cases in the postintervention period (June 2020–December 2020). A reduction in CDI SIR occurred in the postintervention period (Q3 2020–Q4 2020, SIR 0.265) compared to preintervention period (Q4 2019–Q1 2020, SIR 0.338) (Figure 2). We successfully reduced our NHSN HO-CDI SIR below the national average after implementing a 2-step testing algorithm for CDI. The 2-step testing algorithm was useful for antimicrobial stewardship to guide appropriate CDI treatment for true cases and for infection prevention to continue isolation of infected and colonized cases to reduce the spread of C. difficile spores.
Funding: No
Disclosures: None
Figure 1.
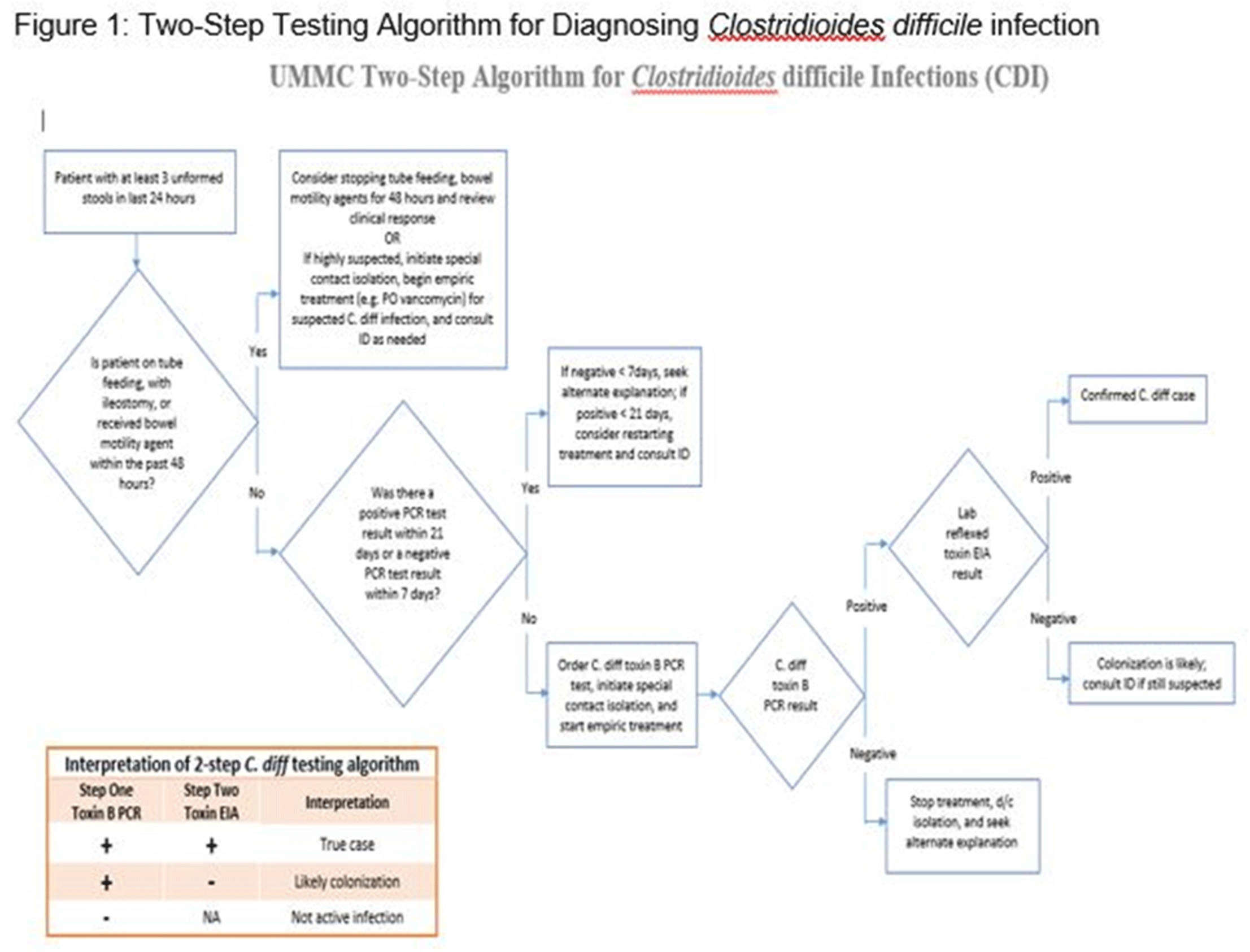
Figure 2.


Did Clostridioides difficile Testing and Infection Rates Change During the COVID-19 Pandemic?
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s43
-
- Article
-
- You have access
- Open access
- Export citation
-
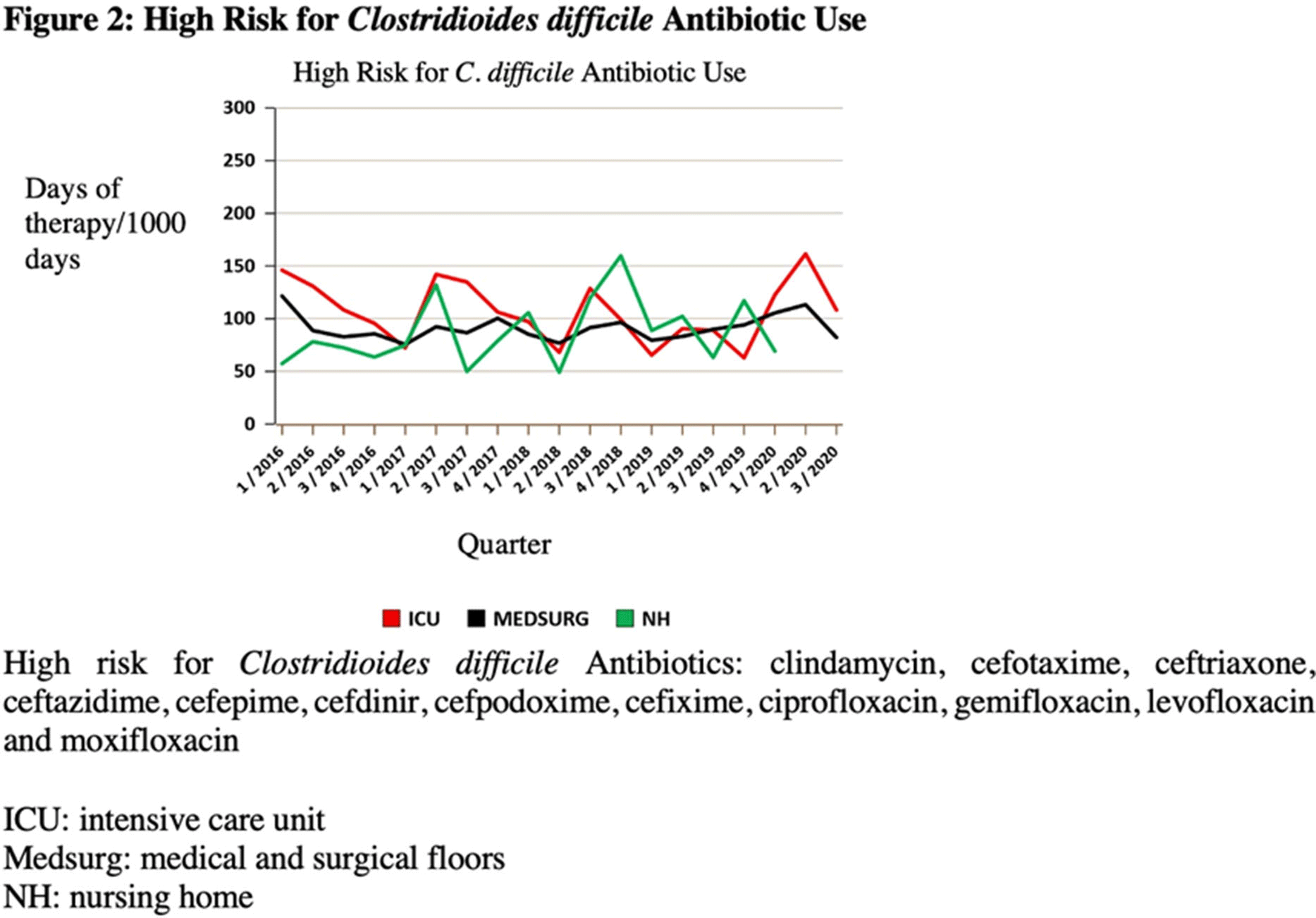
Background: The COVID-19 pandemic has underscored the importance of ongoing infection prevention efforts. Increased adherence to infection prevention recommendations, increased antibiotic use, improved hand hygiene, and correct donning and doffing of personal protective equipment may have influenced healthcare-associated infections (HAIs) in the United States during the pandemic. In this study, we investigated testing for Clostridioides difficile infection (CDI) and incidence during the initial surge of the pandemic. We hypothesized that strict adherence to contact precautions may have resulted in a decreased incidence of CDI in hospitalized patients during the first peak of the COVID-19 pandemic and that CDI testing may have increased even in the absence of directed diagnostic stewardship efforts. Methods: We conducted a single-center, retrospective, observational study at the Veterans’ Affairs (VA) Hospital in Ann Arbor, Michigan, between January 2019 and June 2020. We compared data on CDI tests from January 2019 through February 2020 to data from March 2020 (the admission of the first patient with COVID-19 at our institution) through June 2020. Pre-peak and peak periods were defined by confirmed cases in Washtenaw County. No novel diagnostic or CDI-focused stewardship interventions were introduced by the antimicrobial stewardship program during the study period. An interrupted time series analysis was performed using STATA version 16.1 software (StataCorp LLC, College Station, TX). Results: There were 6,525 admissions and 34,533 bed days between January 1, 2019, and June 30, 2020. Also, 900 enzyme immunoassay (EIA) tests were obtained and 104 positive cases of CDI were detected between January 2019 and June 2020. A statistically significant decrease in EIA tests occurred after March 1, 2020 (the COVID-19 peak in our region) compared to January 1, 2019–March 1, 2020 (Figure 1). After March 1, 2020, the number of EIA tests obtained decreased by 10.2 each month (95% CI, −18.7 to −1.7; P = .02). No statistically significant change in the incidence of CDI occurred. The use of antibiotics that were defined as high risk for CDI increased in the months of April–June 2020 (Figure 2). Conclusions: In this single-center study, we observed a stable incidence of CDI but decreased testing during the first peak of the COVID-19 pandemic. Understanding local HAI reporting is critical because changes in HAI reporting structures and exemptions during this period may have affected national reporting. Further research should be undertaken to investigate the effect of COVID-19 on other HAI reporting within the US healthcare system.
Funding: No
Disclosures: None
Figure 1.
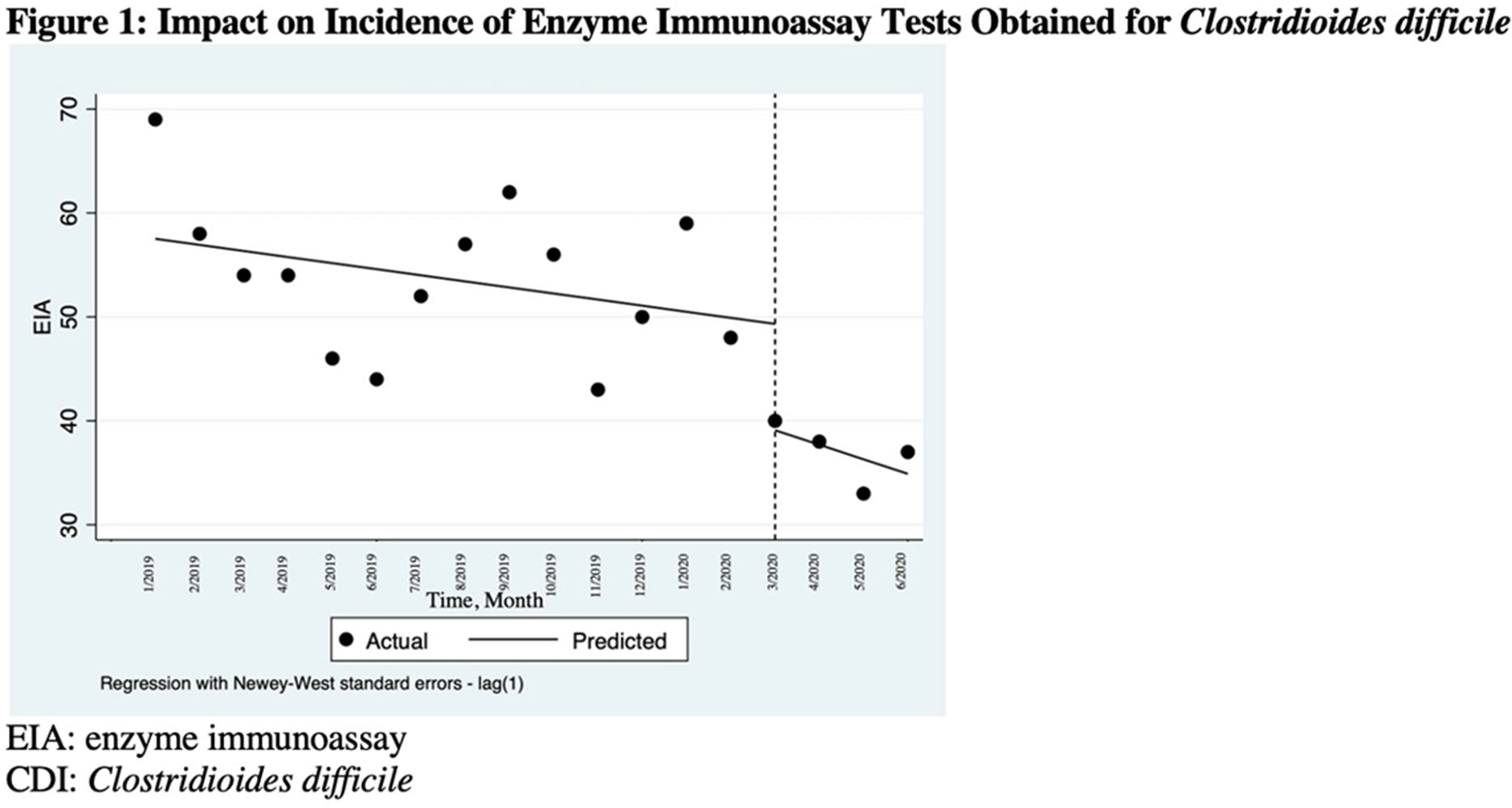
Figure 2.


CLABSI
Inequities in CLABSI Rates in a Children’s Hospital by Race, Ethnicity, and Language Preference
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s43-s44
-
- Article
-
- You have access
- Open access
- Export citation
-
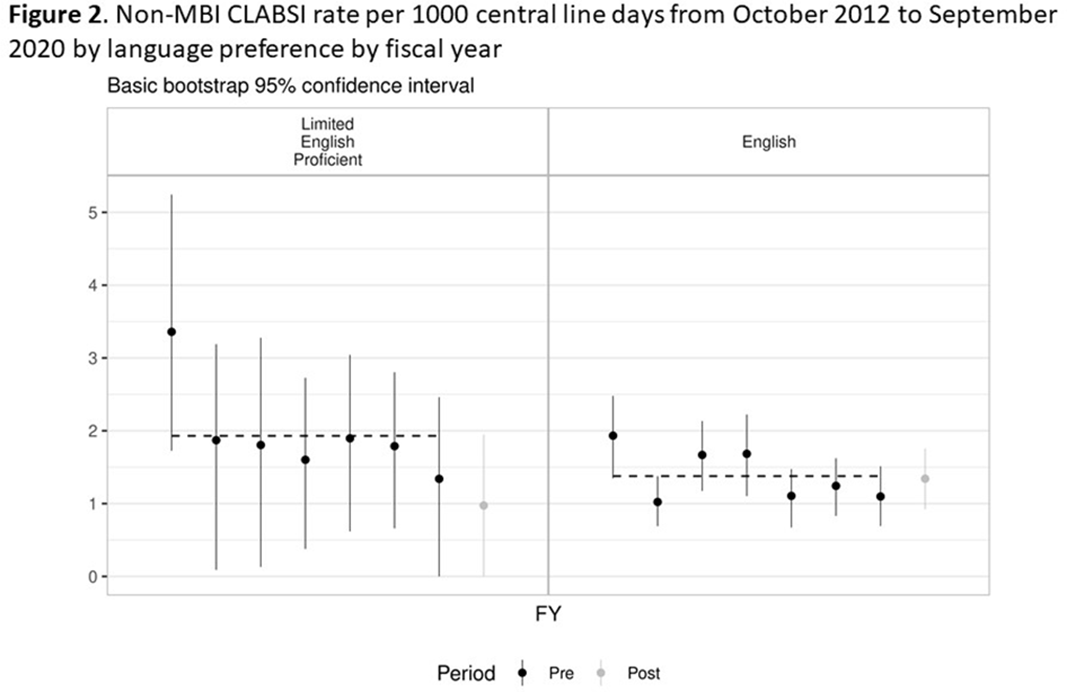
Background: Systemic racism results in health inequities based on patient race, ethnicity, and language preference. Whether these inequities exist in pediatric central-line–associated bloodstream infections (CLABSIs) is unknown. Methods: This retrospective cohort study included patients with central lines hospitalized from October 2012 to June 2019 at our tertiary-care children’s hospital. Self-reported race, ethnicity, language preference, demographic, and clinical factors were extracted from the electronic health record. The primary outcome was non–mucosal barrier injury (non-MBI) CLABSI episodes as defined by the NHSN. CLABSI rates between groups were compared using χ2 tests and Cox proportional hazard regression. We adjusted for care unit, age, immunosuppressed status, diapered status, central-line type, line insertion within 7 days, daily CLABSI maintenance bundle compliance, number of blood draws and IV medication doses, and need for total parental nutrition, extracorporeal membrane oxygenation, and renal replacement therapy. In mid-2019, we engaged stakeholders in each care unit to describe preliminary findings and to identify and address potential drivers of observed inequities. Results: We included 337 non-MBI CLABSI events over 230,699 central-line days (CLDs). The overall non-MBI CLABSI rate during the study period was 1.46 per 1,000 CLDs. Unadjusted CLABSI rates for black or African American (henceforth, “black”), Hispanic, non-Hispanic white, and Asian (the 4 largest race or ethnicity groups by CLDs) patients were 2.74, 1.53, 1.42, 1.24 per 1,000 CLDs, respectively (P < .001) (Table 1). Unadjusted CLABSI rates for patients with limited-English proficiency (LEP) and English-language preference were 1.98 and 1.38 per 1,000 CLDs, respectively (P = .014). After adjusting for covariates, the hazard ratio (HR) point estimate for CLABSI rate remained higher for black patients (HR, 1.50; 95% CI, 0.99–2.28) and patients with LEP (HR, 1.33; 95% CI, 0.87–2.05), compared to the reference group based on largest CLD. The differences in CLABSI rate by race or ethnicity and language were more pronounced in 2 of our 6 care units. Stakeholder engagement and analysis of hospital data revealed opportunities on those units for improved (1) interpreter utilization and (2) line maintenance observation practices by race/ethnicity and language preference (data not shown). These findings and CLABSI rates over time by race/ethnicity and language preference (Figures 1 and 2) were shared with frontline staff. Conclusions: In our children’s hospital, CLABSI rates differed based on patients’ self-reported race, ethnicity, and language preference, despite controlling for factors commonly associated with CLABSI. Identifying inequities in CLABSI rates and mitigating their determinants are both essential to the goal of achieving equitable care.
Funding: No
Disclosures: None
Table 1. 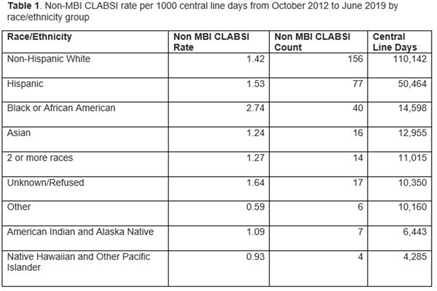
Figure 1.
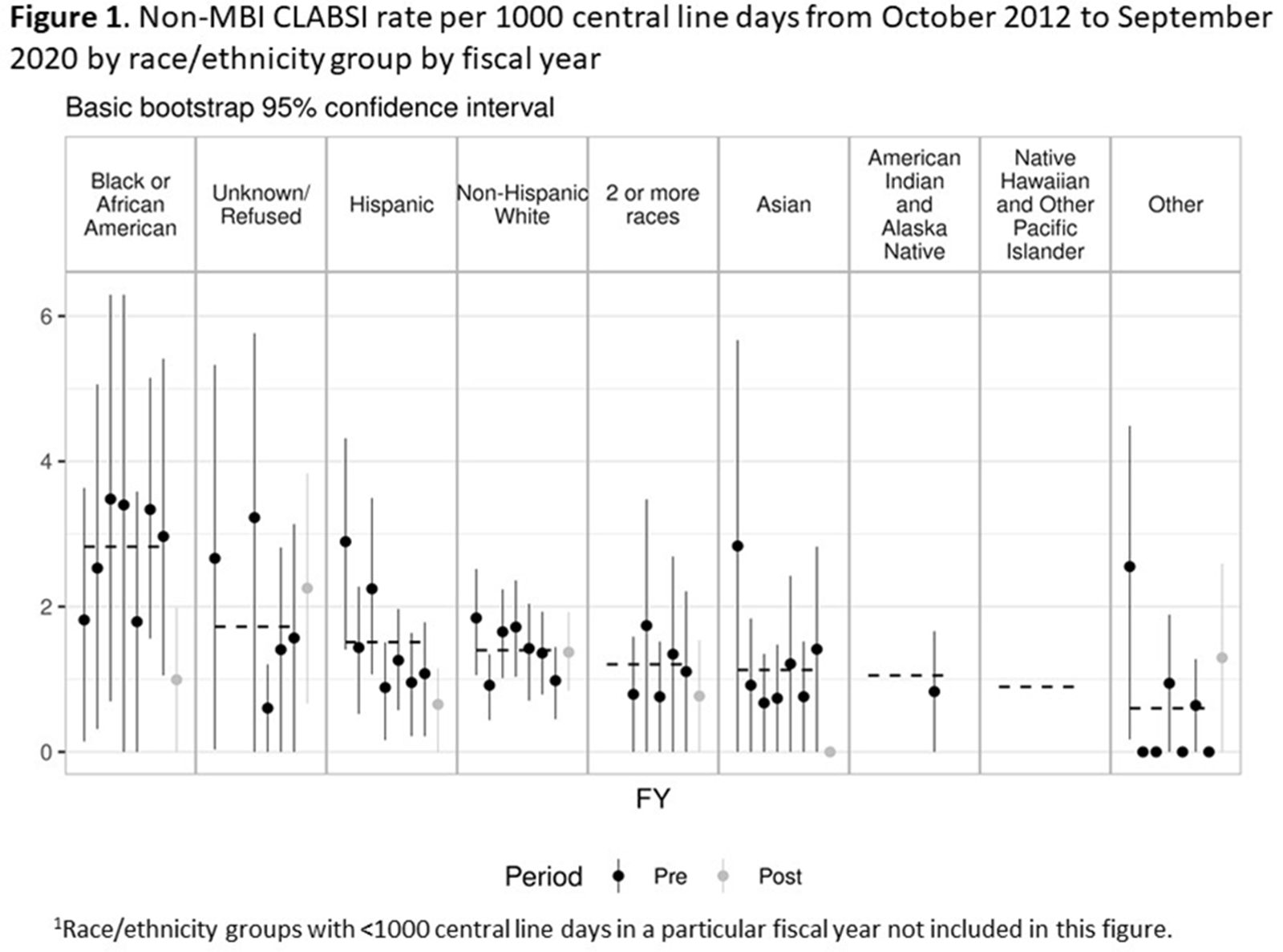
Figure 2.



COVID-19
Use of COVID-19 Serologic Testing in Healthcare Workers with Acute Respiratory Tract Infection
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s44
-
- Article
-
- You have access
- Open access
- Export citation
-
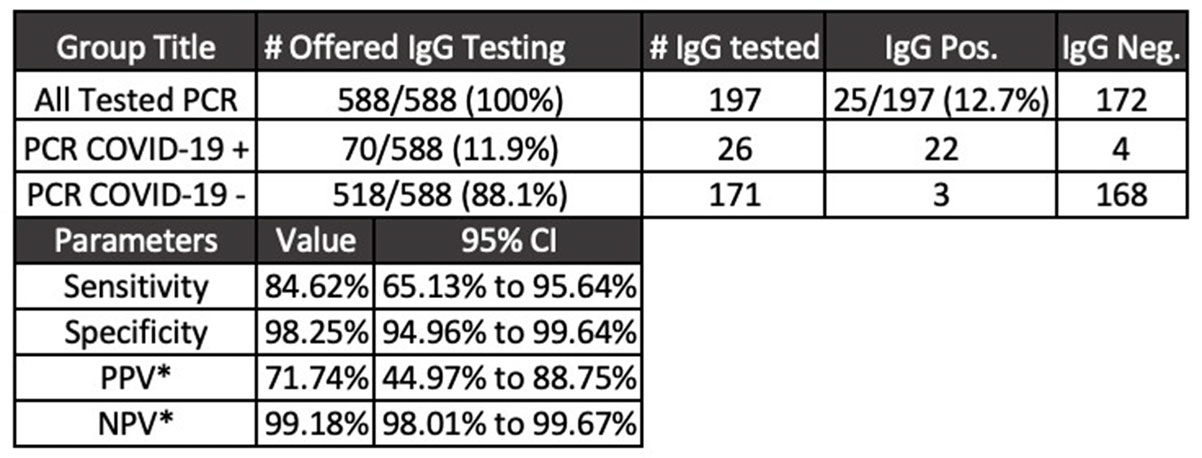
Background: Diagnostic tests for COVID-19 are in high demand. Serologic assays are of interest as diagnostic adjuncts to SARS-CoV-2 quantitative polymerase chain reaction (PCR); however, many of the commercially available assays have limited validation data and clinical utility is unknown. We describe the utilization of SARS-CoV-2 IgG enzyme-linked immunosorbent assay (ELISA) for healthcare workers with acute respiratory tract infection (ARTI) who underwent SARS-CoV-2 PCR testing. Methods: The MetroHealth System is the largest public hospital system in Ohio, employing ~8,000 staff. COVID-19 detection began in early March 2020. EDI novel coronavirus COVID-19 IgG ELISA (KT-1032) targeting antibody response to viral nucleocapsid was obtained for diagnostic and seroprevalence analyses. Manufacturer reports of sensitivity and specificity of the assay are 100% and 99%, respectively. A 2-part test strategy for employees with symptoms of ARTI was implemented. Qualifying symptoms for SARS-CoV-2 PCR testing included fever and either cough or shortness of breath. Additional symptoms were included to reflect expanding knowledge of COVID-19. Employees who underwent SARS-CoV-2 PCR testing (Luminex ARIES) were offered serologic testing on day 14 following PCR result. Education accompanied the offer for serologic testing as well as the receipt of test result to aide interpretation. Results: From April 16, 2020, through July 6, 2020, 588 employees underwent PCR testing. Overall, 70 cases of COVID-19 were detected. Of the 197 employees who opted for serologic testing, IgG positivity was 12.6%. The mean time to IgG collection following PCR result was 30 days (range, 10–79). Using PCR results obtained in the clinical setting of ARTI as the diagnostic gold standard, IgG was 84.6% sensitive and 98.2% specific (Figure 1). Conclusions: In a population of symptomatic healthcare workers, SARS-CoV2 IgG testing was specific for COVID-19 diagnosis. Sensitivity was inadequate compared to the positive predictive agreement of 90% or greater required for US Food and Drug Administration emergency use authorization. In a low-prevalence environment for COVID-19 (<5%), a positive SARS-CoV-2 IgG has a low positive predictive value, which may falsely imply immunity and may negatively affect infection prevention practices.
Funding: No
Disclosures: None
Figure 1.

COVID-19 and Ventilator-Associated Event Discordance
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s45
-
- Article
-
- You have access
- Open access
- Export citation
Stewardship of Remdesivir Use in a Rural Community Hospital During the COVID-19 Pandemic
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s45
-
- Article
-
- You have access
- Open access
- Export citation
-
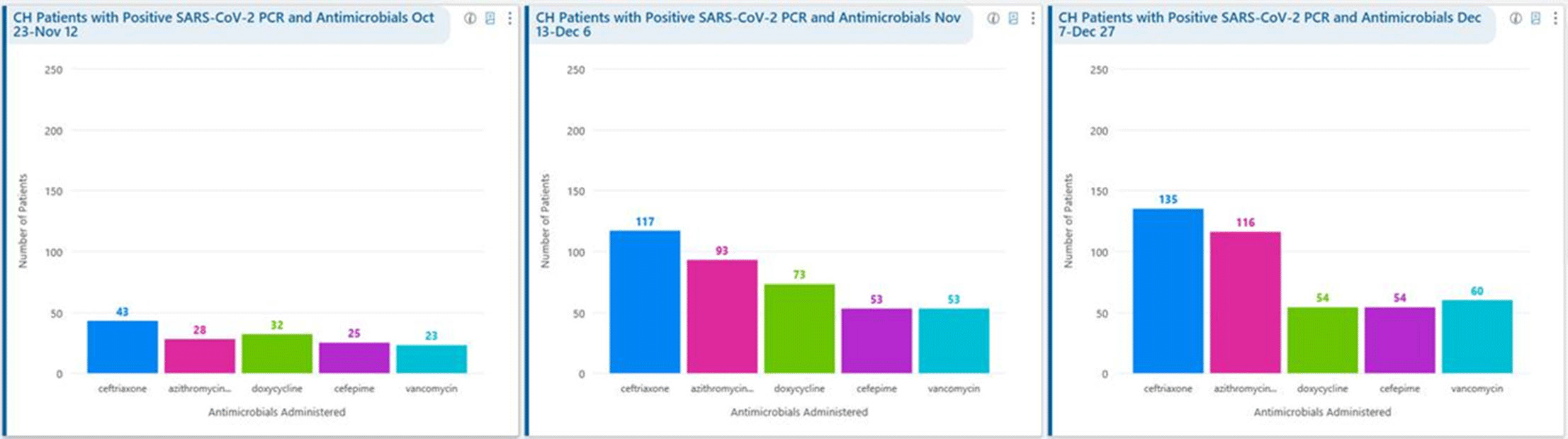
Background: Remdesivir was granted EUA followed by full FDA approval for treatment of hospitalized COVID-19 patients on October 22, 2020, based on the results from the ACTT1 trial. Remdesivir use was initially restricted to infectious disease (ID) physicians in our hospital with prescription needing formal ID consultation until complete approval. Due to increasing case counts in our hospital, a decision was made to allow intensivists and hospitalists the authorization to prescribe remdesivir in a phased manner. In this retrospective study, we assessed the impact of phased-in prescribing on remdesivir utilization and days of therapy of antimicrobials. Methods: Remdesivir prescribing was streamlined by real-time institutional guidelines developed by a COVID-19 treatment committee constituting ID and other clinicians. Eligibility for remdesivir included positive SARS-CoV-2 PCR test, severe disease defined as persistent hypoxia (<94% oxygen saturation on room air), requiring supplemental oxygen and/or on mechanical ventilation (MV) for <72 hours, and symptom onset of <10 days. We retrospectively reviewed cohorts of 3 periods during which remdesivir was prescribed. In the first cohort A, between October 23, 2020, and November 12, 2020, remdesivir was restricted to ID physicians with formal ID consultation. Cohort B comprised inpatients between November 13, 2020, and December 6, 2020, when hospitalists and intensivists were allowed to prescribe remdesivir through an EMR order set after prior authorization by an ID physician via curbside or telephonic consultation. Cohort C, from December 7, 2020, to December 26, 2020, comprised inpatients with unrestricted prescribing of remdesivir by hospitalists and intensivists. We also evaluated antibiotic use. Results: In cohort A, SARS CoV-2 positivity was 20.3%; 64 inpatients tested positive and 35 patients (54.7%) who met the criteria were prescribed remdesivir after a formal consultation with an ID physician. In cohort B, requiring prior authorization by an ID physician, SARS-CoV-2 positivity rapidly increased to 34%; 193 patients tested positive and 97 patients (50.3%) received remdesivir. In cohort C, during unrestricted access, positivity further increased to 38%; 235 inpatients tested positive and 123 (52.5%) received remdesivir. Remdesivir use remained steady during the 3 phases of gradual de-escalation of restricted prescribing and safe handoff in the context of clear guidelines, as well as ongoing curbside education provided by ID physicians during the second phase. Cohort B demonstrated the best prescribing rates. Antimicrobial prescribing data were also collected during the 3 cohort phases (Figures 1–3). Conclusions: Remdesivir is an expensive antiviral with limited utility and maximum benefit in COVID-19 inpatients who are hypoxic but do not require mechanical ventilation. Stewardship of remdesivir with safe, gradual handoff to inpatient can be achieved without overuse.
Funding: No
Disclosures: None
Figure 1.
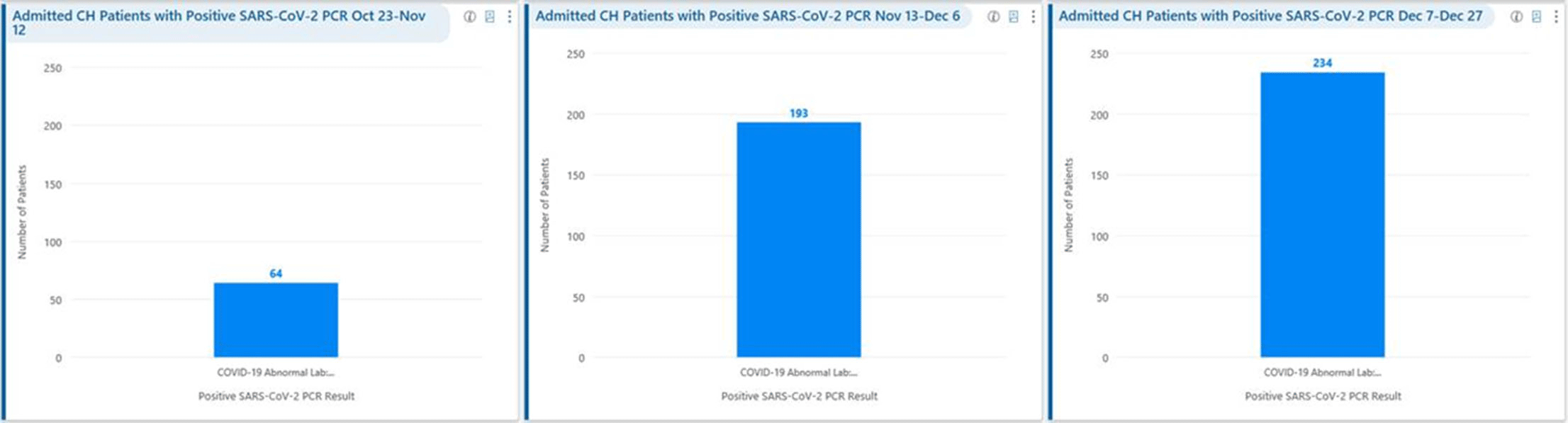
Figure 2.
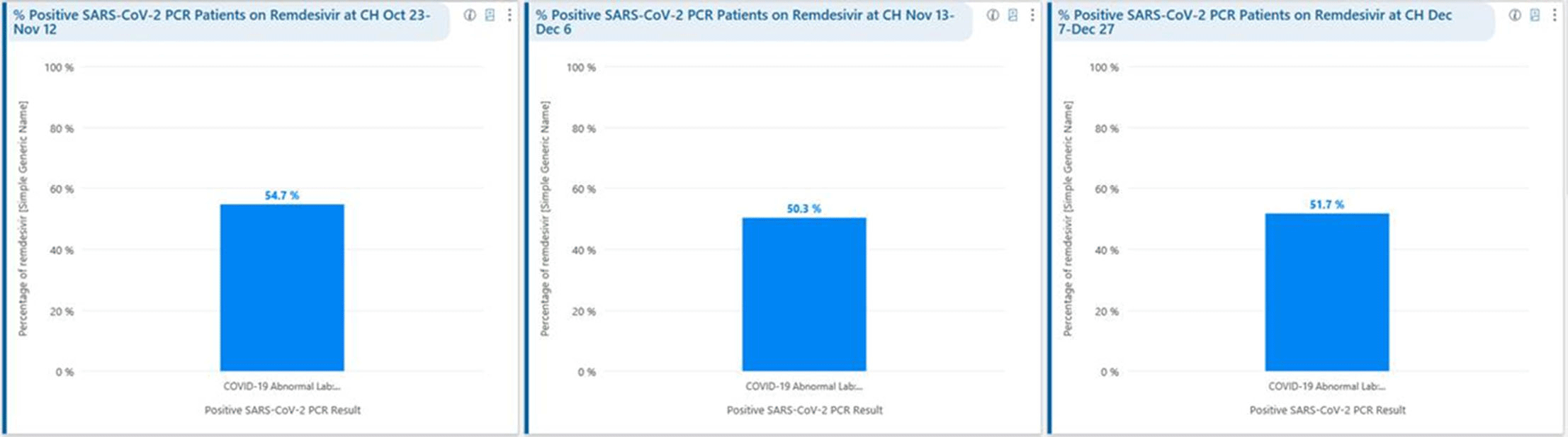
Figure 3.



Comparing Hospital Healthcare-Associated Infection Incidence During Pre-COVID-19 Pandemic and Pandemic Eras
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s45-s46
-
- Article
-
- You have access
- Open access
- Export citation
-
Background: Diversion of resources from infection prevention activities, personal protective equipment supply shortages, conservation (extended use and reuse) or overuse with multiple gown and glove layers, and antimicrobial prescribing changes during the COVID-19 pandemic might increase healthcare-associated infection (HAI) incidence and antimicrobial resistance. We compared the incidences of Clostridioides difficile infection (CDI), methicillin-resistant Staphyloccocus aureus bloodstream infection (MRSA BSI), and vancomycin-resistant enterococci bloodstream infection (VRE BSI) reported by California hospitals during the COVID-19 pandemic with incidence data collected prior to the pandemic. Methods: Using data reported by hospitals to the California Department of Health via the NHSN, we compared incidences in the second and third quarters of 2020 (pandemic) to the second and third quarters of 2019 (before the pandemic). For CDI and MRSA BSI, we compared the standardized infection ratios (SIRs, based on the 2015 national baseline), and we calculated the P values. No adjustment model is available for VRE BSI; thus, we measured incidence via crude incidence rates (infections per 100,000 patient days). We calculated incidence rate ratio (IRR) with 95% CI for VRE BSI. To examine the possible effect of missing data during the pandemic, we performed a sensitivity analysis by excluding all facilities that had incomplete data reporting at any time during either analysis period. Results: Incidence measures and numbers of facilities contributing data in prepandemic and pandemic periods are shown in Table 1. There were no statistically significant changes in SIRs at P = .05 for either MRSA BSI or CDI between the prepandemic and pandemic periods (MRSA BSI P = .17; CDI P = .08). Crude VRE BSI incidence increased during the pandemic compared to the prepandemic period (IRR, 1.40; 95% CI, 1.16–1.70). Excluding facilities with incomplete data had minimal effect. Conclusions: We found insufficient evidence that MRSA BSI or CDI incidence changed in California hospitals during the pandemic relative to the prepandemic period; however, there was a significant increase in the crude incidence of VRE BSI. Next, we will include interrupted time series analyses to assess departure from long-term trends, including a risk-adjusted model for VRE BSI. Additionally, we will evaluate for changes in central-line–associated bloodstream infection incidence and antimicrobial resistance among HAI pathogens.
Funding: No
Disclosures: None
Table 1. 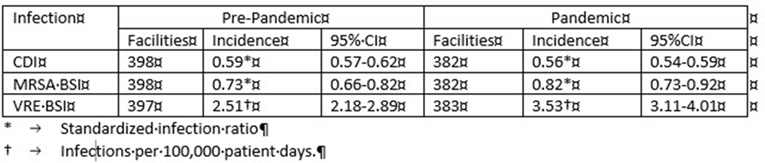

Secondary Bacterial Pneumonias and Bloodstream Infections in Patients Hospitalized with COVID-19
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s46
-
- Article
-
- You have access
- Open access
- Export citation
COVID-19 Contact Tracing in a Pediatric Hospital: Maximizing Effectiveness Through Specialized Team and Automated Tools
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s46-s47
-
- Article
-
- You have access
- Open access
- Export citation
Transmission of COVID-19 on an Inpatient Hospital Prison Unit
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s47
-
- Article
-
- You have access
- Open access
- Export citation
Building a PPE Monitor Team as Part of a Comprehensive COVID-19 Prevention Strategy
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s47
-
- Article
-
- You have access
- Open access
- Export citation
The COVID-19 Pandemic and Antibiotic Use on the United States–Mexico Border
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s47-s48
-
- Article
-
- You have access
- Open access
- Export citation
Risk Factors for In-Hospital Mortality from COVID-19 Among Nursing Home Patients—An Urban Center Experience
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s48
-
- Article
-
- You have access
- Open access
- Export citation
Linking Staff Cases in a Hospital COVID-19 Outbreak Using Electronic Tracking Data
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s48
-
- Article
-
- You have access
- Open access
- Export citation
Using a Quality-Driven Approach to Maintain an N-95 Respirator Supply During a Pandemic-Driven Global Shortage
-
- Published online by Cambridge University Press:
- 29 July 2021, pp. s48-s49
-
- Article
-
- You have access
- Open access
- Export citation
Prevalence of SARS-CoV-2 Antibody in Healthcare Workers in Central Pennsylvania
-
- Published online by Cambridge University Press:
- 29 July 2021, p. s49
-
- Article
-
- You have access
- Open access
- Export citation