



Mass casualty and disaster incidents are both complex and dynamic, providing a challenging environment for first responders to navigate and to respond to.Reference Abrahamsen 1 , Reference Lichtman and Nair 2 Decisions by an incident commander (IC) are often made in a high intensity, uncertain environment with ambiguous information and minimal or sub-optimal situational awareness.Reference Abrahamsen 1 It has been suggested that unmanned aerial vehicle (UAV) technology has the potential to fundamentally change the practice of civilian emergency medical services (EMS), improving the situational awareness of ICs and safety of first responders.Reference Leduc 3 UAVs can provide ICs with enhanced capabilities such as mass gathering monitoring, delivery of medical supplies, search and rescue, telemetry in remote areas, and early warning of danger during operations.Reference Leduc 3 - Reference Wen, Zhang and Wong 7 In comparison to a rotor-wing or fixed-wing manned aircraft, UAVs are faster to deploy, flexible, efficient, and customizable based on the requirements of the employing agency’s needs. The humanitarian community has been using UAV’s for several years in areas of disaster mapping, information gathering, community capacity building, logistics and transportation of goods.Reference Boccardo, Chiabrando, Dutto, Tonolo and Lingua 8 - Reference Fornace, Drakeley, William, Espino and Cox 10 UAV computer model networks have been shown to greatly reduce life saving equipment travel times for victims of cardiac arrest.Reference Pulver, Wei and Mann 11 Scene size up is an important step by paramedics prior to entering a potential hazardous environment to triage and treat casualties. One potential use of UAV technology is in the identification of scene hazards that may alter the response to a mass casualty or disaster incident.Reference Abrahamsen 1 , Reference Kurvinen, Smolander, Pöllänen, Kuukankorpi, Kettunen and Lyytinen 12 Despite a proliferation of UAV technology we were unable to find any studies that compared UAV technology to standard practice (SP) in this context.Reference Wesson and Humphreys 13
The aim of this study was to compare UAV technology to SP, by paramedic students, in hazard identification during a simulated multi-vehicle motor collision (MVC) in terms of time to identification, accuracy, and the order of hazard identification.
Methods
Study Design
This was a prospective observational cohort study using UAV technology on simulated hazards based on actual motor vehicle collisions on Prince Edward Island, Canada from 2014 to 2016. The scene set up was based on a real MVC. The ethics committee for human research at Holland College, Charlottetown, Prince Edward Island, Canada approved this study.
Study Setting and Population
In total, 21 students in their first year of the primary care paramedic program at Holland College were invited to participate in the study consisting of one group of 11 UAV students and one group of 10 SP students. All 21 were present for the scene lecture, UAV lecture, hands on session as well as the study scenario. Inclusion criteria included male and female students who were 18 years or older and in good academic standing within the primary care paramedic program. Potential participants were excluded if they opted not to voluntarily participate in the study or were unable to complete the study. All students were provided with a standardized 30 minute lecture on hazard identification in mass casualty and disaster incidents. Following this lecture all students received a 1-hour visual introduction to UAV technology by a UAV pilot operator. The study database contained no participant personal identifiers.
A 10 vehicle motor collision was simulated on a portion of an unused runway at a local airport. Traffic cones were set up on the perimeter simulating the borders of a standard Canadian 2 lane highway. The total area of the scene was ~160×25 ft. All vehicles were inspected and made safe by a designated firefighter/scene safety officer. Vehicle placement was based on a multiple motor vehicle collision that occurred on I-84 near Baker City, Oregon on January 17, 2015 7 hazards were placed throughout the scene in a realistic fashion. The location of these hazards was determined by the scene safety officer. The hazards included: a power line, a fuel spill (gasoline), fire, an active shooter, an unstable structure (vehicle perched on side), WHIMIS (workplace hazardous material information system) placard on the side of a vehicle, and an explosion potential (propane cylinders) (Figure 1).

Figure 1 Layout of simulated multi-vehicle accident scene with fuel, fire, power line, active shooter, explosion potential, WHIMIS placard and unstable vehicle.
UAV Technology
A Tornado H920 UAV (Yuneec International, Jinxi, Kunshan, China) was the UAV platform of choice operated by a professional UAV pilot. The total airtime per battery for this UAV was 24 minute with a range of 700 m and a takeoff weight of 4990 g allowing a maximum height of 4000m The ground station was based on Android operated system consisting of flight control, camera control, and a large digital display. A special flight operations certificate was granted by Transport Canada for this study providing the necessary flight framework to undertake this project.
Study Flow
The study was carried out over a 2-day period. Following an explanation of the study, participants were randomized into 2 groups; either UAV or SP. Study participants were initially blinded to the set-up of the MVC scene and were seconded to a room ~1 km from the area. They were then individually transported to the scene in the back of an ambulance. Upon arrival, the participants were taken directly to a canvas tent where they were unable to obtain any visual information of the MVC. A brief scenario was read to them by an adjudicator informing them that were required to identify 7 simulated hazards within the scene. Participants were given an opportunity to clarify any issue with regard to their role, requirements, or mechanics of the study. Next, participants left the tent and proceeded to the scene directly (SP group) or to the UAV ground station (UAV group). The adjudicator began timing the participants immediately after leaving the tent. The SP group walked the scene verbalizing the hazards to the adjudicator as they identified them. The UAV group while looking at a monitor directed the pilot in maneuvering the UAV, verbalizing the identification of hazards to the adjudicator. Timing stopped once all hazards were identified by the participant. The order of identification was also recorded.
Measurements
The primary outcome measures were the difference in time to identification of hazards, the difference in the order hazard identification and accuracy.
Data Analysis
Statistical analysis consisted of a 2 sample t-test to compare the time to hazard identification. Difference in rank order between the 2 groups were assessed statistically by a non-parametric permutation test based on the sum of squared deviations between average rank order across hazards [Stata software (Statistical software); StatCorp LP, College Station, TX, 2013]. Generally, statistical tests had a two-tailed alternative and were interpreted at a significance level of P<0.05.
Results
The mean time (SD, range) to identify the hazards were 3 minutes 41 seconds (1 minute 37 seconds, 1 minute 48 seconds-6 minutes 51 seconds) and 2 minutes 43 seconds (55 seconds, 1 minute 43 seconds-4 minutes 38 seconds) in the UAV and SP groups respectfully, corresponding to a difference of 58 seconds (95% CI: −14 seconds, 2 minutes 11 seconds). The difference was not statistically significant (P=0.11). Statistical analysis by a non-parametric permutation test based on 9999 simulations showed a significant (P=0.04) difference in the order of hazard identification in the 2 groups (see Figure 2). The statistical difference is essentially driven by 2 hazards, fuel and workplace hazardous material information system placard with the UAV group identifying fuel hazard faster than the SP group. The SP group identified the WHIMIS hazard faster than the UAV group. Both groups demonstrated 100% accuracy in identification of the hazards.
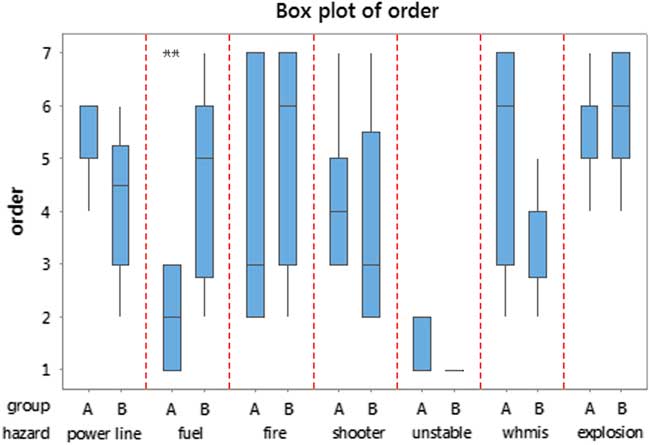
Figure 2 Box plot of the hazard ordering in the two groups UAV (A) and Standard Practice (B). This figure also shows the distribution of order scores for each hazard within each of the two groups. The statistical difference is essentially driven by fuel and WHIMIS.
Discussion
Although there are multiple sources that promote UAVs within the disaster medicine context there are limited studies conducted on topic comparing UAV technology and SP.Reference Abrahamsen 1 , Reference Wesson and Humphreys 13 , 14 We wanted to examine the effect of this technology on the first part of managing a mass casualty motor vehicle collision scene, namely safe hazard identification. 5 , Reference Kurvinen, Smolander, Pöllänen, Kuukankorpi, Kettunen and Lyytinen 12 , Reference Rodriguez, Geckle and Barton 15 During this type of event first responders could be exposed to a number of different hazards that would cause harm to both themselves and victims. Having the ability to identify these hazards prior to entering the scene could potentially prevent EMS injury as well as providing increased situational awareness for the incident commander. However, if this technology caused delay in the delivery of triage and treatment then this risk of delay could potentially outweigh the technology benefits. This study did not demonstrate a statistically significant difference in the time to hazard identification between the UAV and SP group. The average time to hazard identification was 58 seconds longer by the UAV method. We do not believe that 58 seconds is a clinically significant time difference based on this type of incident. More importantly, we demonstrated that this technology allowed the primary care paramedic student to correctly identify all hazards from a safe distance without exposure that could cause harm. With this in mind, an IC could mitigate these hazards and utilize appropriate resources with minimal impact on time during the scene size up phase of an incident.
According to our results there was a difference in the order of hazard identification. This was essentially driven by both the fuel and WHIMIS hazards. The UAV group identified the fuel faster than the SP group. The SP group identified the WHIMIS placard faster than the UAV group. This could be explained by the angle of the field of view for each of the hazards depending on the method used for identification. Walking the scene did not allow the paramedic student to see the fuel hazard until close to the fluid on the ground. Whereas the UAV was able to clearly delineate the fuel on the ground from the air. The WHIMIS placard was on the side of an upright vehicle that was relatively easy to identify from ground level when approaching the scene. From the air it was more difficult to observe the placard due to the field of view angle from the camera of the UAV. The overall importance of the differences in order identification in this study is likely negligible. However, in a real life scenario early identification of hazards that must be avoided [unstable structures, chemical biological radiological nuclear (CBRN) exposures] could be life saving.
Previous studies have examined the use of UAV technology in major incidents including mass casualty traffic incidents. These being more descriptive in nature, case studies, opinion pieces, simulation, or feasibility studies.Reference Abrahamsen 1 , Reference Leduc 3 , 6 , 14 , Reference Cook, Zhao, Lee and Yim 16 , Reference Claesson, Fredman and Svensson 17 This study is one of the first to conduct a prospective observational cohort method using UAV technology on simulated hazards with primary care paramedic students. This study not only demonstrated the feasibility of the technology but its significant benefit in identification of scene hazards within the disaster medicine context.
Limitations
There are both technical and design limitations when considering the results of this study. The UAV platform itself, like any airframe, is subject to the weather, performance limitations based on battery life and payload capability that could potentially impact its flight envelope. There was also a delay communication between the direction from the paramedic student to the UAV operator. This delay could be addressed in a future study where the subjects are qualified both as a paramedic and an UAV pilot thus providing a better understanding of UAV technology. In Canada, UAV’s are subject to regulatory bodies and we were granted a special flight operations flying certificate to conduct this study. Agencies requiring the use of UAV technology would need to obtain a special flight operations certificate on short notice and this may not be feasible for a MCI. Although 58 seconds may not be considered significant for a difference in hazard identification a larger study with a great number of hazards may demonstrate a difference in time that would be considered significant. Overall, the number of study participants was low. We employed a convenience sample of primary care paramedic students and did not apply a power calculation to determine a minimum sample size. A repeat of this study with more participants may have revealed differences that went undetected in this study. Finally, this was a simulation environment that is different from the actual clinical setting, which may have distractors and other factors that are not represented by simulation formats.
Conclusion
Prior to entering the scene of a MCI paramedics must ensure that the scene is safe. This study demonstrated the accurate, safe, and feasible use of UAV technology in the identification of hazards at a MCI scenario by primary care paramedic students. No statistical significant difference was noted in time to scene hazard identification using UAV technology versus SP. Although there was a difference found in the order of hazard identification both SP and UAV arms were 100% accurate. This study was limited by a sample of convenience and the research question merits further evaluation by employing a larger sample size to verify the results.

