



Introduction
The City of New York (New York USA) estimates that 91,000 responders were involved in the eight-month clean-up and recovery operation following the September 11, 2001 terrorist attacks (9/11).Reference Savitz, Oxman and Metzger1 These responders were exposed to a myriad of toxic materials including asbestos, lead, dioxins, and benzene.Reference Lippmann, Cohen and Chen2 Various health programs track the on-going health effects of 9/11 on responders. On January 2, 2011, the James Zadroga 9/11 Health and Compensation Act of 2010 (Zadroga Act) was signed into law and the World Trade Center (WTC) Health Program (WTCHP) was created to monitor and treat responders and survivors with 9/11-related adverse health conditions.Reference Santiago-Colon, Daniels and Reissman3 Eligibility details for inclusion in the program are available elsewhere.4–6
Health data from responders are collected by the WTCHP and summarized to inform a range of research outputs, including the program statistics reported by the Centers for Disease Control and Prevention (CDC; Atlanta, Georgia USA). The objective of this research was to review the WTCHP statistics reported by the CDC to analyze health trends among enrolled responders as the 20-year anniversary of the terrorist attacks approaches.
Methods
The CDC reports WTCHP statistics on responders enrolled and responders certified (approved) for treatment for 9/11-related health conditions. This information is updated quarterly and includes statistics on the overall enrollment of responders in the program, new enrollees within the last 12 months, and enrollment by responder type, age, gender, and state. Statistics are also reported on the number of responders with conditions certified by the Zadroga Act categories of conditions, including the top ten certified conditions (Figure 1) and top ten cancers (Figure 2).
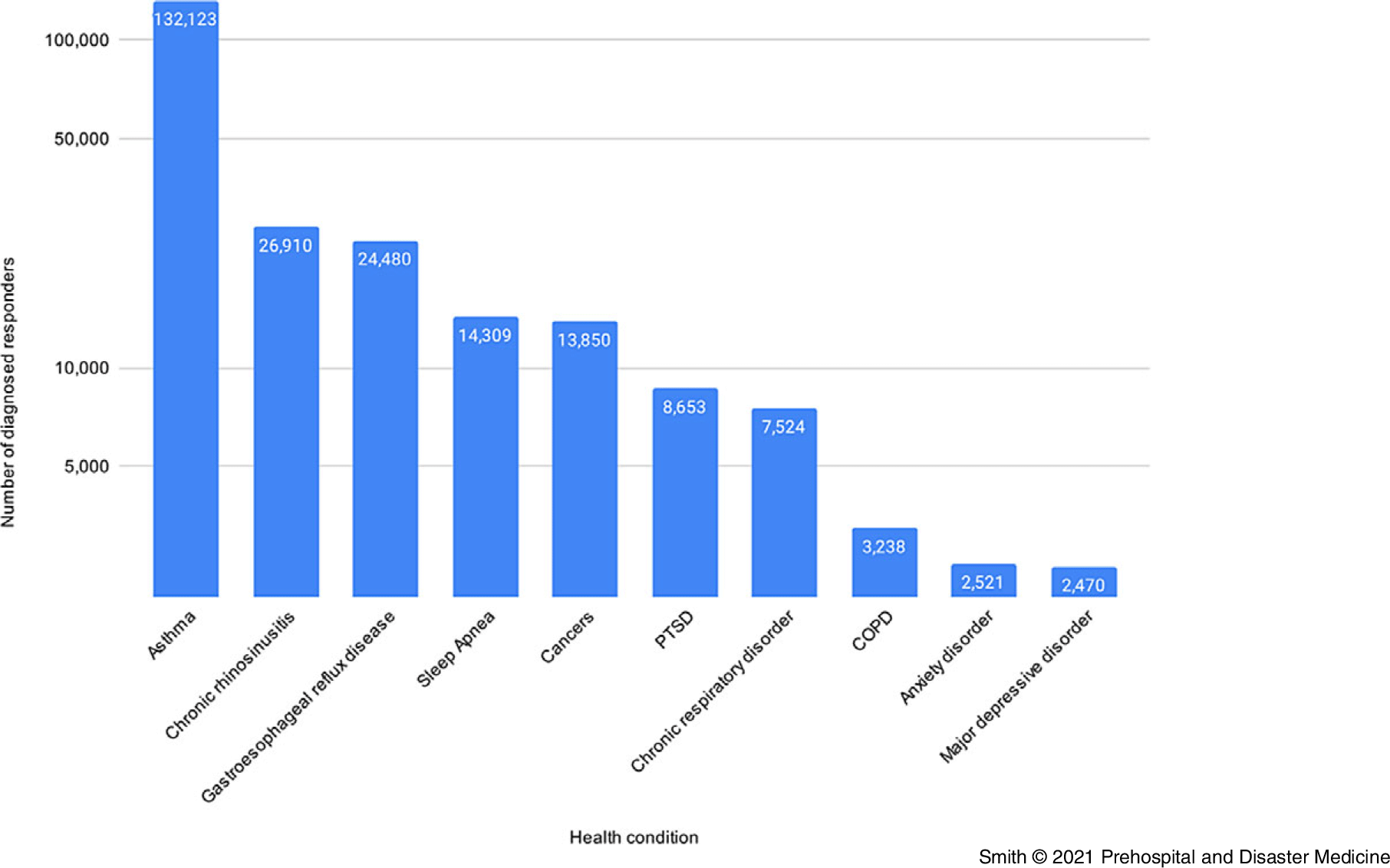
Figure 1. Top 10 Certified Conditions (Responders).
Note: Individual responders may have certifications in more than one category.
Abbreviations: COPD, chronic obstructive pulmonary disease; PTSD, posttraumatic stress disorder.

Figure 2. Top 10 Certified Cancers (Responders).
Note: Individual responders may have certifications in more than one category.
In June 2021, a comprehensive review of WTCHP statistics was undertaken by two members of the research team utilizing a combination of publicly available reports and datasets from the CDC utilizing a data extraction form designed for the study. Statistics from July 2011 through March 2021 were included. A third member of the research team checked raw data and combined results for accuracy. Statistics for non-responders were excluded.
The research was granted exemption from human ethics review by the Edith Cowan University Human Research Ethics Committee (Joondalup, Perth, Western Australia; Project Number 2021-02677).
Results
A total of 80,745 responders were enrolled in the WTCHP as of March 2021 (Figure 3). Of these, 62,773 were classified as “general” responders (including police, ambulance, rescue, recovery, clean-up, and related support workers and volunteers); 17,023 were New York City Fire Department (FDNY; New York USA) responders (including active and retired firefighters, emergency medical technicians, and paramedics); and 989 were Pentagon (Arlington, Virginia USA) and Shanksville (Pennsylvania USA) responders who participated for at least one day in rescue and recovery efforts at any of the former WTC sites.
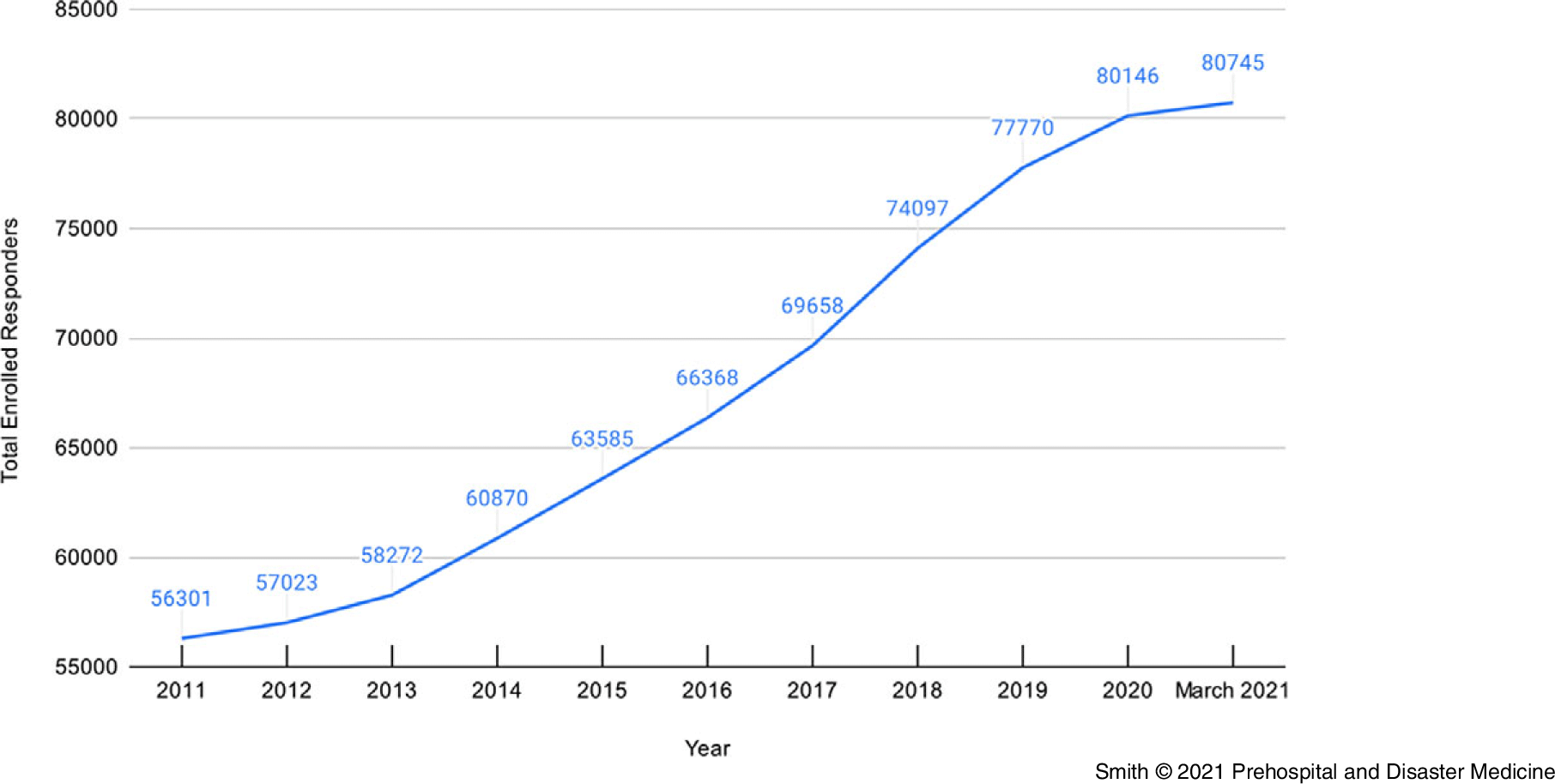
Figure 3. Total Enrollments in the World Trade Center Health Program (Responders).
Just under 40% of responders with health issues were aged 45-64 (Figure 4) and 83% were male. The general responders were more racially and ethnically diverse compared to FDNY responders who were mostly non-Hispanic, white, and male.Reference Santiago-Colon, Daniels and Reissman3 Of the total responders in the program, 3,439 are deceased; the primary causes of death were aerodigestive illness (34%), cancer (30%), and mental ill health (15%).

Figure 4. Number of Certifications by Age (Responders).
Health certifications are classified using the Zadroga Act Categories of Conditions and individual responders enrolled in the program may have certifications in more than one category. Forty-five percent of responders enrolled in the WTCHP had aerodigestive illness; 16% had cancer; 16% had mental health illness; and 0.7% had musculoskeletal and acute traumatic injuries.
Discussion
There has been an observed increase of 185% among this cohort for all certified cancers within the top ten over the past five years. While the certified cancer types listed in the top ten have remained constant during this time-period, there has been a shift in ranking, with leukemia now overtaking colon and bladder cancer. This equates to an increase of 175% in certified leukemia cases within this cohort of responders over a five-year period. This finding supports previous research identifying increased incidence of cancer among 9/11 responders.Reference Solan, Wallenstein and Shapiro7–Reference Shapiro, Wallenstein and Dasaro9 The increased incidence of leukemia within this cohort is not surprising; there is a proven link between benzene exposure and acute myeloid leukemia,Reference Shallis, Weiss, Deziel and Gore10 and benzene, which is found in jet fuel, was one of the toxic exposures at the WTC site.
Firefighter responders have been reported to have a modest, yet statistically significant, excess of cancer cases in the WTC-exposed cohort compared to the general population.Reference Zeig-Owens, Webber and Hall11 However, a subsequent study comparing the same cohort with firefighters from Chicago (Illinois USA), San Francisco (California USA), and Philadelphia (Pennsylvania USA) with similar, non-WTC-related occupational exposure found no excess cancer in the WTC firefighters. Thyroid cancer was significantly elevated from 2001 to 2009, however, this was not significant when surveillance bias was accounted for. Prostate cancer was elevated between 2005 to 2009 and warrants further follow-up.Reference Moir, Zeig-Owens and Daniels12
Surveillance bias has also been documented as a potential explanation for an excess risk of thyroid cancer reported in different WTC-dust exposed cohorts.Reference Van Gerwen, Cerutti and Rapp13–Reference Tuminello, van Gerwen and Genden15 Increased surveillance can potentially lead to an increased diagnosis of earlier-stage thyroid cancers. However, there remains uncertainty as to what extent surveillance bias has contributed to the reported increase in incidence of thyroid cancer among responders, highlighting the on-going need to explore a potential causal link between exposure to WTC dust and thyroid cancer. Future studies should explore the potential consequences of exposure to WTC dust on the thyroid gland.
This review identified an elevation in prostate cancer cases over the past five years, with an observed increase of 181% among this cohort of responders. Prostate cancer is most often diagnosed in older men, with the average age of men at diagnosis being 66.Reference Gupta, Supta and Saini16 Around six cases in ten are diagnosed in men who are 65-years or older, and it is usually rare in men under 40. However, analysis of prostate cancer cases among responders has found that some responders develop an aggressive, fast-growing form of prostate cancer.Reference Gong, Wang and Yu17 Inhaling the toxic dust at the WTC site potentially caused a cascading series of cellular events, increasing the number of inflammatory T-cells in some of these 9/11 responders. This increased inflammation may eventually lead to prostate cancer.Reference Stark, Livas and Kyprianou18 Prostate cancer tissue samples from responders have revealed a higher degree of expression of immunologic and inflammatory genes than tissue samples from prostate cancer tumors from non-responders. Animal models that were exposed to WTC dust had the same over-expression of inflammatory genes in the prostate, leading to the hypothesis that exposure by inhalation in WTC responders increased the local inflammatory response in the prostate, and this process facilitated prostate cancer development.Reference Gong, Wang and Yu17
There has been a combined increase of 607% in deaths attributed to the top four certified conditions (aerodigestive illness, cancer, mental ill health, and musculoskeletal and acute traumatic injuries) since the beginning of 2016. Between the end of 2016 and March 2021, deaths associated with aerodigestive illness increased by 289%; deaths associated with cancer increased by 707%; deaths associated with mental ill health increased by 159%; and deaths associated with musculoskeletal and acute traumatic injuries increased by 100%. While not specifically identified within the WTCHP data, federal agents from the Federal Bureau of Investigation (FBI) have also seen a recent increase in the number killed by 9/11-related illnesses, with at least 16 FBI agent deaths recorded as of May 2019.19,20
While cancer has arguably exacted the highest toll on 9/11 responders over the years, research suggests they also have notably higher rates of cardiovascular disease.Reference Cohen, Zeig-Owens and Joe21 Firefighters on the scene at the WTC were found to be 44% more likely to develop cardiovascular disease than those who arrived the next day. This finding suggests a significant association between greater exposure at the WTC site and a higher risk of long-term cardiovascular disease. Greater exposure, however, was not found to be associated with a responder’s risk of cancer, nor was the amount of dust to which they were exposed.Reference Shapiro, Wallenstein and Dasaro9
The large body of research conducted after the 9/11 attacks suggests that the burden of posttraumatic stress disorder (PTSD) among 9/11 responders is substantial, with as many as 15% to 20% of responders living with PTSD symptoms.Reference Smith, Holmes and Burkle22–Reference Clouston, Kotov and Pietrzak26 This is roughly four-times the rate of PTSD symptoms typically found in the general population.27 Most studies of 9/11 responders have documented an increase in PTSD over time, which contrasts with the general population where most longitudinal studies show declining rates of prevalence.Reference Lowell, Suarez-Jimenez and Helpman28 Posttraumatic stress disorder that is 9/11-related is associated with sociodemographic and background factors, event exposure characteristics, loss of life of significant others, and social support factors.Reference Neria, DiGrande and Adams29
Recent research has identified that PTSD and depression in 9/11 responders is related to cognitive issues, including difficulty recalling names and words, and a greater reliance on written reminders.Reference Singh, Zeig-Owens and Rabin30,Reference Singh, Zeig-Owens and Hall31 Researchers have also found that the thinning of the grey matter in the brain scans on 9/11 responders is indicative of early-stage dementia. These results build on previous work in this population noting that cognitive impairment occurs at approximately twice the rate of population controls for people 10 to 20 years older.Reference Clouston, Deri and Horton32
These findings echo those from studies of veterans and certain other survivors of trauma that have shown PTSD and depressive symptoms are risk factors for mental dysfunction.Reference Brown, Antonius, Kramer, Root and Hirst33–Reference Shalev, Gevonden and Ratanatharathorn35 Though forgetfulness can sometimes simply be a result of age, this recent research reported that the cognitive effects were similar for both younger and older members of the study group.Reference Singh, Zeig-Owens and Rabin30,Reference Singh, Zeig-Owens and Hall31 Even almost 20 years later, the prevalence of mental health disorders and need for mental health treatment remains elevated among this group of 9/11 responders, with almost one-half of all responders reporting an on-going need for mental health care.Reference Diab, DePierro and Cancelmo36
An emerging threat for this cohort of responders will be cancers associated with exposure to asbestos at the WTC site. As of 2016, at least 352 responders had been diagnosed with asbestosis and at least 444 had been diagnosed with pulmonary fibrosis. Exposure to asbestos and other fibers in the toxic 9/11 dust may have contributed to these cases.37 The development of mesothelioma will continue to be a concern among this cohort of responders, as it usually takes between 20 and 50 years to develop after asbestos exposure.
Compounding existing health issues for 9/11 responders, the coronavirus disease 2019 (COVID-19) pandemic has taken a great toll. Illnesses linked to 9/11 exposure, including cancer and respiratory ailments, have left this cohort uniquely vulnerable to a novel coronavirus that attacks the lungs and the immune system. More than 100 responders have died to date due to complications from the virus.38 According to the National Institute for Occupational Safety and Health (NIOSH; Washington, DC USA), at the end of August 2020, some 1,200 responders had confirmed cases of COVID-19.39 Even among 9/11 responders who have not been infected with COVID-19, the pandemic has exacerbated one of the key conditions caused by search and rescue and recovery efforts after terrorist attacks: PTSD.Reference Rodriguez and Muylaert40
Limitations
The findings reported in this publication are subject to several limitations. From a methodological perspective, the use of existing databases for research has many of the same challenges as those for chart-review-based research.Reference Stratton41–Reference Gilbert, Lowenstein, Kiziol-McClain, Barta and Steiner44 The use of pre-existing databases can be prone to systematic error that can lead to selection bias, marginal error, and interpretation bias. More difficult to address is missing data and invalid data entry within original databases. Validation of data entered in a database is essential if data analysis is to be considered accurate. Invalid data entry can occur from several sources, including error due to variation for data elements without absolute definition, data entry error, and miscoding error. The WTCHP is a well-designed database that requires a number of steps to be taken to minimize bias and error and ensure that data are accurate, complete, and reliable. In addition, the two independent researchers that reviewed this pre-existing database information are disciplined in use and interpretation of pre-recorded data that are derived for a study.
Due to these limitations, trends identified from this dataset need to be viewed with some caution. Direct links can’t be made between exposure to the WTC site or length of time at the WTC and risk of illness. Differences in age, sex, ethnicity, smoking status, and other factors between the exposed and unexposed groups should also be considered. Increased rates of thyroid cancer in WTC-exposed cohorts may be associated with heightened surveillance rather than an increase in disease. The number of people enrolled in the WTCHP does not reflect the full population of responders involved in initial search and rescue or subsequent recovery and clean-up operations. It is estimated that some 400,000 people were exposed to WTC-derived contaminants in the days, weeks, and months following the attacks.Reference Newman45 With the trends identified by this review highlighting that 9/11-exposure is still causing both physical and mental health impact to responders, it is likely that responders are still developing illnesses related to their exposures and many have yet to enroll in the WTCHP.
Conclusion
The long-term effects of responding to the 9/11 terrorist attacks are beginning to be fully understood. The number of responders enrolling in the WTCHP increases each year, and the number of illnesses and deaths associated with response to the toxic WTC site continues to grow. On-going monitoring of the health status of the responders who worked at the WTC site remains a priority, especially considering the looming threat of new asbestos-related cancers.
Conflicts of interest
none
Supplementary Materials
To view supplementary material for this article, please visit https://doi.org/10.1017/S1049023X21000881





