



The SARS CoV–2 outbreak in 2019, which led to the COVID–19 pandemic, has had an impact on the daily lives of people of all ages that is unprecedented in the modern era. COVID–19 remains a worldwide emergency that is challenging all sectors of society (World Health Organization [WHO] 2020), including increased numbers of deaths and hospitalizations (Adhikari et al., Reference Adhikari, Meng, Wu, Mao, Ye, Wang, Sun, Sylvia, Rozelle, Raat and Zhou2020), adverse effects on the mental health of healthcare workers (Greenberg et al., Reference Greenberg, Docherty, Gnanapragasam and Wessely2020), and a greater burden of grief and bereavement (Mayland et al., Reference Mayland, Harding, Preston and Payne2020). Perhaps unsurprisingly, these consequences have attracted their own research interest.
The fact that older adults are more likely to experience serious complications (including death) from COVID–19 have made this group the focus of public health decisions, political discussion, and media attention (Shahid et al., Reference Shahid, Kalayanamitra, McClafferty, Kepko, Ramgobin, Patel, Aggarwal, Vunnam, Sahu, Bhatt, Jones, Golamari and Jain2020). However, most studies have focused on the negative effects of the pandemic, including how severe disease affects older people (Mueller et al., Reference Mueller, McNamara and Sinclair2020), or the presence of ageism within society or when making medical decisions (Previtali et al., Reference Previtali, Allen and Varlamova2020). Less is known about the strengths and social or personal resources that older adults may use to cope.
Primarily, the present study aimed to fill the gap in our knowledge by exploring the strengths of older persons based on the concept of post-traumatic growth (PTG), as defined by Tedeschi and Calhoun (Reference Tedeschi and Calhoun1996). As a secondary aim, we sought to identify the variables that predict this PTG in terms of the form of experience of COVID–19, the specific sociodemographic variables, and the social resources of older persons.
Post-Traumatic Growth
During our lifetimes, we each face events that deeply impact our health, emotional balance, social relationships, and life goals. Luhmann et al. (Reference Luhmann, Fassbender, Alcock and Haehner2020) have defined that important events (which they label as “major life events”; MLEs) are “events that are clearly timed, disrupt one’s everyday routine, and are perceived as personally significant and memorable by those who experience them” (p. 2).
Although many MLEs are reported as negative or highly stressful for the person, they can also positively affect psychological and social factors, leading to personal growth. This paper focus on the theory and process of PTG, which is defined as a “positive psychological change experienced as a result of the struggle with highly challenging life circumstances” (Tedeschi & Calhoun, Reference Tedeschi and Calhoun2004, p. 1). This positive change could affect cognitive ideas or values, emotions, and behaviors (Tedeschi & Calhoun, Reference Tedeschi and Calhoun1996). PTG has been studied especially in unexpected MLEs such as natural disasters (Tang, Reference Tang2006), becoming a refugee (Chan et al., Reference Chan, Young and Sharif2016), or facing a potentially fatal illnesses such cancer (Pérez-San-Gregorio, Reference Pérez-San-Gregorio, Martín-Rodríguez, Borda-Mas, Avargues-Navarro, Pérez-Bernal, Conrad and Gómez-Bravo2017) or HIV/AIDS (Sawyer et al., Reference Sawyer, Ayers and Field2010). Research has shown that experiencing PTG predicts a good level of psychological and social adjustment after an MLE (Jayawickreme & Blackie, Reference Jayawickreme and Blackie2016).
According to Tedeschi and Calhoun’s (Reference Tedeschi and Calhoun2004) model of PTG, experiencing an MLE poses several challenges. These include managing distressing emotions and questioning important beliefs and goals, both of which leave marks on a person’s life narrative (Tedeschi & Calhoun, Reference Tedeschi and Calhoun2004). Processes of rumination, such as deliberated rumination or meaning-making thoughts, are core to eliciting PTG (Calhoun et al., Reference Calhoun, Cann, Tedeschi, Weiss and Berger2010). That is, it is not only the trauma itself that enables PTG but also the cognitive and emotional assessment and changes that people endorse about their life and future (Linley & Joseph, Reference Linley and Joseph2004). Tedeschi and Calhoun’s (Reference Tedeschi and Calhoun2004) model provided the framework for building the PTGI-SF used in this study. It considers five areas of change: (a) Relating to others, (b) new possibilities, (c) personal strength, (d) spiritual change, and (e) appreciation of life (Cann et al., Reference Cann, Calhoun, Tedeschi, Taku, Vishnevsky, Triplett and Danhauer2010). Variables have been studied that seem to influence the experience of PTG. Features of the event, such as time since it occurred and the type of event, as well as sociodemographic variables and social resources, have been stressed to be the most relevant (Wu et al., Reference Wu, Kaminga, Dai, Deng, Wang, Pan and Liu2019).
Facing COVID–19 and PTG
Dealing with COVID–19 may be described as an undesirable life event for individuals, thanks to the low level of person control, low anticipation of the event, and lack of familiarity (Luhmann et al., Reference Luhmann, Fassbender, Alcock and Haehner2020). These unique features mean that it cannot be compared accurately with previous literature on PTG or with other kinds of disruptive life events, such as wars (Chan et al., Reference Chan, Young and Sharif2016) or natural disasters (Nalipay & Mordeno, Reference Nalipay and Mordeno2018). Although the social restrictions imposed due to COVID–19 have a clear time frame, as in the case of other major life events it is not known how much time is needed afterwards for PTG to occur. Following Wu et al. (Reference Wu, Kaminga, Dai, Deng, Wang, Pan and Liu2019), who stated that the best descriptions of PTG are those made closest to the event, this study was conducted immediately after the 49 days of forced lockdown in Spain. This time point was a landmark for many people – a moment of respite after the first wave of the pandemic. Moreover, the individual could have been exposed to the consequences of COVID–19 in at least one of three overlapping scenarios.
First, one can be infected by the disease. Research on this topic has focused on how to control the infection and how it impacts the person, either during the infection or in terms of negative long-term consequences (Ferrarese et al., Reference Ferrarese, Silani, Priori, Galimberti, Agostoni, Monaco, Padovani and Tedeschi2020). Second, people may face the death of someone close because of COVID–19. The issues of bereavement and grief have been studied only by looking at the negative consequences of not being able to have a proper funeral or not being able to accompany the relative in the last moments of life (Burrell & Selman, Reference Burrell and Selman2020). Third, most people had to deal with a forced lockdown to limit the transmission of infection. Again, only the negative effects of lockdown on family dynamics, especially those families that have children (Fontanesi et al., Reference Fontanesi, Marchetti, Mazza, Di Giandomenico, Roma and Verrocchio2020), or on the increase in loneliness or psychological distress (Losada-Baltar et al., Reference Losada-Baltar, Jiménez-Gonzalo, Gallego-Alberto, Pedroso-Chaparro, Fernandes-Pires and Márquez-González2020) have been described.
The present research will explore differences in how PTG is experienced depending on exposure, taking into account participants that had direct experience of the virus (whether they were infected or they lost a close relative because of the virus) and those with indirect experience (i.e., only being involved in lockdown). This direct or indirect contact has been studied in other MLEs, such as the 9/11 attacks (Cann et al., Reference Cann, Calhoun, Tedeschi, Taku, Vishnevsky, Triplett and Danhauer2010) and the Katrina and Rita hurricanes of 2005 (Stanko et al., Reference Stanko, Cherry, Ryker, Mughal, Marks, Brown, Gendusa, Sullivan, Bruner, Welsh, Su and Jazwinski2015) in the US.
Sociodemographic Variables Associated with PTG
Few studies have explored the sociodemographic variables associated with PTG (Jayawickreme & Blackie, Reference Jayawickreme and Blackie2016). Although sex, marital status, and age have each been associated with PTG, the results have been inconsistent (Helgeson et al., Reference Helgeson, Reynolds and Tomich2006). Women have been reported to express more PTG than men (Wu et al., Reference Wu, Kaminga, Dai, Deng, Wang, Pan and Liu2019). This seems to be based on a tendency to use more positive appraisals as coping strategies to deal with traumatic or negative events. It may be that this cognitive strategy elicits PTG (Nowlan et al., Reference Nowlan, Wuthrich and Rapee2015).
Widowhood and the process of bereavement have also been the focus of some studies, considering how this change can influence PTG. However, not all the bereaved adults experience PTG after a partner’s death (Kim et at., Reference Kim, Kjervik, Belyea and Choi2011) and comparative studies has found no significant differences between widowed and non-widowed adults (López et al., Reference López, Camilli and Noriega2015).
As for age, comparative studies have revealed less PTG among older people (Sim et al., Reference Sim, Lee, Kim and Kim2015; Wu et al., Reference Wu, Kaminga, Dai, Deng, Wang, Pan and Liu2019), although sample characteristics indicate that people older than 70 years are rarely included (Wu et al., Reference Wu, Kaminga, Dai, Deng, Wang, Pan and Liu2019). Some studies suggest that the higher PTG scores among younger people could be explained by both the need to make life adjustments and the ease with which they can be made (Sawyer et al., Reference Sawyer, Ayers and Field2010). However, other reviews have shown inconsistent associations between age and PTG (Linley & Joseph, Reference Linley and Joseph2004; Stanton et al., Reference Stanton, Bower, Low, Calhoun and Tedeschi2006), with Davison et al. (Reference Davison, Kaiser, Spiro, Moye, King and King2016) even explaining that older adults could experience more PTG due to the normal process of reminiscence and valuing life. This is consistent with the work of psychologist Erik Erikson (Reference Erikson1963), who entitled this the final stage, integrity vs. despair, in his model of psychosocial development.
It is important that we study the experiences and challenges of older people during the COVID–19 pandemic given that this group has arguably suffered most from the disease and its consequences (Verity et al., Reference Verity, Okell, Dorigatti, Winskill, Whittaker, Imai, Cuomo-Dannenburg, Thompson, Walker, Fu, Dighe, Griffin, Baguelin, Bhatia, Boonyasiri, Cori, Cucunubá, FitzJohn, Gaythorpe and Ferguson2020). Older age has been considered a risk factor for presenting health complications (or death) due to the virus (World Health Organization [WHO], 2021). Moreover, despite experiencing the same lockdown as younger people, this group has had to face greater fear of infection (Ishikawa, Reference Ishikawa2020), greater feelings of loneliness and social isolation (Tyrrell & Williams, Reference Tyrrell and Williams2020), and ageism in terms of how authorities have dealt with the pandemic (Ehni & Wahl, Reference Ehni and Wahl2020). The greater vulnerability to COVID–19 and its negative impacts on physical, psychological, and social factors in older adults highlight the importance of studying PTG in this group. Given that such research may uncover protective factors for this population, this study focused on the positive impact of the COVID–19 pandemic on older adults.
Social Resources and PTG
The PTG model (Tedeschi & Calhoun, Reference Tedeschi and Calhoun2004) stresses the importance of social resources and how networks could enable the person to disclose and talk about their feelings and worries regarding the trauma, potentially helping to elicit PTG. It is likely that the forced lockdown affected precisely those social resources, and that it potentially affected social isolation or feelings of loneliness (Brooke & Jackson, Reference Brooke and Jackson2020). Older adults who perceived higher social support during the forced lockdown did not experience an increase in loneliness, not even those who lived alone (Groarke et al., Reference Groarke, Berry, Graham-Wisener, McKenna-Plumley, McGlinchey and Armour2020; Luchetti et al., Reference Luchetti, Lee, Aschwanden, Sesker, Strickhouser, Terracciano and Sutin2020). For example, many face-to-face befriending interventions adapted their programs to a phone-call format in order to reduce the risk of social isolation in older adults with limited technological skills (Kahlon et al., Reference Kahlon, Aksan, Aubrey, Clark, Cowley-Morillo, Jacobs, Mundhenk, Sebastian and Tomlinson2021). Given the importance of these social resources during lockdown, this study will explore their capacity for encouraging meaningful conversations with individuals’ networks and for mitigating feelings of loneliness, above all in relation to PTG.
The COVID–19 pandemic is a unique MLE for most of us that has had many negative implications, but that may also have been associated with PTG. However, this has not been studied to date, so in this study, the aim was to assess PTG in older people in Spain during the forced lockdown between March and April 2020. It was hoped that this would reveal what COVID–19 experiences (personal infection, bereavement, and lockdown), sociodemographic variables, and social resources are associated with PTG.
Method
Sample
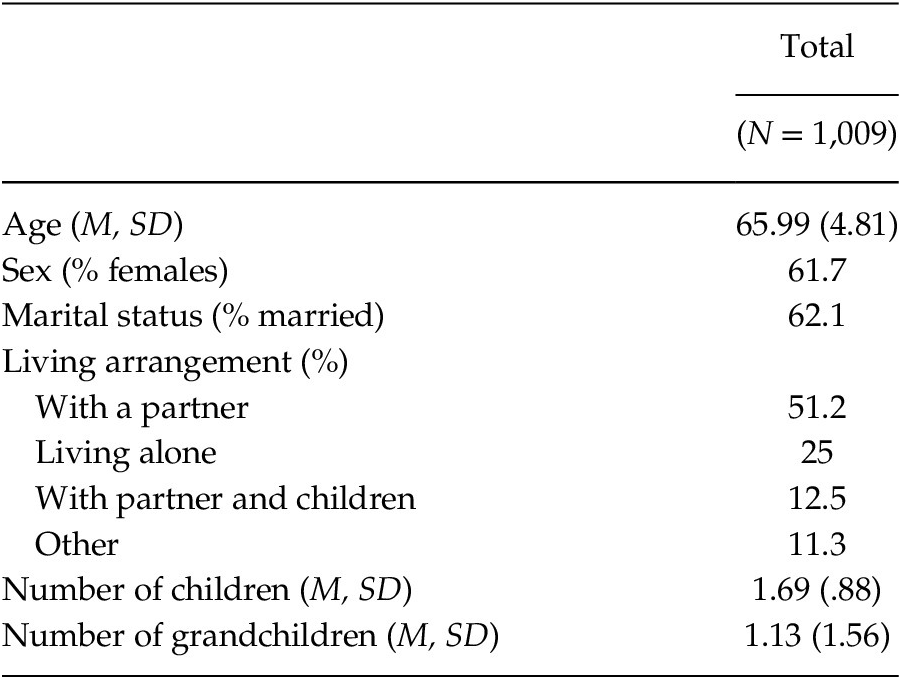
In total, 1,009 people aged 55 and older participated in the study (Table 1). All were senior students at the University of Experience of the University of Barcelona (Spain), their age range was 55–88 years, and all lived in Barcelona or its metropolitan area.
Table 1. Description of the Sample
Instrument
The questionnaire administered to participants included three sections. The first section covered sociodemographic information, such as sex, number of children and grandchildren, marital status, and living arrangements. The second and third sections were then specific to COVID–19 and their experiences.
The second section comprised the short form version of the Post-traumatic Growth Inventory (PTGI-SF). Participants received instruction to assess the degree of change that they had experienced due to the COVID–19 pandemic. Higher scores indicated that older adults perceive that they experienced more change due to the COVID–19. The PTGI-SF is a ten-item form that retains the original five subscales of the PTGI (relating to others, new possibilities, personal strength, spiritual change, and appreciation of life) (Cann et al., Reference Cann, Calhoun, Tedeschi, Taku, Vishnevsky, Triplett and Danhauer2010). Each item has six Likert-type answer categories, from 0 (“No change”) to 5 (“a high degree of change”). Although its structure into five subscales (2 items per subscale), previous studies usually only used the full-scale scores (Vishnevsky et al., Reference Vishnevsky, Cann, Calhoun, Tedeschi and Demakis2010). In this study, the Spanish translation by Cárdenas Castro et al. (Reference Cárdenas Castro, Barrientos Delgado, Ricci Alvarado and Páez Rovira2015) was used, for which the Cronbach’s alpha was reported to be .83 and the five-subscale structure of the Spanish translation was deemed valid. In this study, Cronbach’s alpha value reached .94.
The third section included a series of questions regarding the impact of COVID–19 and social resources. Two questions focused on Covid–19: If they had been infected by the virus (yes/no) and if someone close had died because of Covid–19 (yes/no). Regarding social resources during the lockdown, we asked about any changes in feelings of loneliness (increase, no change, or decrease) or the level of meaningful conversation (increase, no change, or decrease).
Procedure
The first author of this paper contacted the director of the University of the Third Age (University of Barcelona, Spain) and explained the objective of the study and the general procedure for data collection. After obtaining agreement to collaborate, a survey link was sent to all students. Qualtrics Surveys was used to create the questionnaire and monitor the survey distribution and responses. The online questionnaire included an introduction page in which information of the project and contact with the main researcher was given. Participants gave written informed consent in order to participate in the study and if only they gave their contest they were able to fill the questionnaire. The informed consent followed the same information the ethics committee formally approved.
There were 1,512 senior students studying one of fourteen degrees offered by the University in 2019–2020. The courses required twice weekly attendance at regular classes for senior students and at least one optional subject with undergraduate students. Due to the lockdown, however, all classes were suspended. The survey was conducted online for 17 days from 8th May to 24th May, immediately after the forced lockdown in Barcelona and its metropolitan area ended. During those 17 days, only walking and sports activities were allowed, and only at certain hours. No informal or formal meetings were allowed, and senior centers, shopping centers, bars, and restaurants were closed. Two reminder emails to complete the survey were sent to all students during the data collection period.
The final sample comprised 1,073 participants, giving a response rate of 70.97%. However, 64 participants did not answer the PTGI-SF completely and were dropped from the analysis. Participants from all courses responded in high numbers, but those from gastronomy (82.1%), psychology (76.1%), and philosophy (71.6%) courses responded in the highest proportions. This project received the ethical approval by The University of Barcelona’s Bioethics Commission (CBUB).
Data Analysis
To analyze PTG differences because of impact of COVID–19, sociodemographic variables, and social resources, a series of t test or correlations were performed, depending the nature of the variables studied. Thereafter, stepwise regression analysis was performed to explain the influence on overall PTG of the variables that had a significant impact in the correlation analyses. IBM SPSS Statistics version 25 was used to analyze the data.
Results
As shown in Table 2, PTGI-SF scores were diverse, with a mean of 17.54 (standard deviation: 12.54) and only 20.5% of the sample reaching 60% of the PTGI-SF score considered by Wu et al. (Reference Wu, Kaminga, Dai, Deng, Wang, Pan and Liu2019) to indicate a moderate-to-high PTG. The highest subscale score was for “Appreciation of life” and the lowest was for “Spiritual change.”
Table 2. Mean Scores of PTG

To analyze differences in PTG due to the impact of COVID-19 and according to sociodemographic variables and the availability of social resources, a series of t tests or correlations were performed. Post-traumatic growth was significant associated with the experience of COVID–19, but only those who had been infected by it scored significantly higher on the PTGI-SF, t(983) = 2.302, p = .022, with no significant differences for participants who had experienced the death of a close relative because of COVID–19. Concerning the sociodemographic variables, only women, t(995) = 2,017, p = .044, and younger participants (r = –.098, p < .001) had significantly higher scores. Marital status, living arrangements, number of children and grandchildren were not related to PTG. Finally, an increase in the number of meaningful conversations during lockdown, F (2, 1,000) = 49.219, p < .001, and perceptions of loneliness (either an increase or a decrease; F (2, 982) = 15.123, p <.001) were associated with higher PTGI-SF scores.
All variables significantly associated with PTGI-SF scores were entered in a three-step hierarchical multiple regression analyses to explore their combined effects on PTG (Table 3). No multicollinearity was found between the different variables in any of the regression models, as VIF values were between 1 and 1.14. Durbin-Watson’s value was 2.07, also within the recommended values for this statistic. In Step 1, direct exposure to COVID–19 was entered; in Step 2, sex and age were entered; and in Step 3, loneliness and level of meaningful conversations were entered. All three models were significant: Model 1, F (1, 928) = 4.99, p < .05, accounted for only 0.53% of the explained variance; Model 2, F (3, 926) = 5.99, p < .001, increased the variance explained slightly to 1.9%; and Model 3, F (7, 922) = 17.22, p < .001, did increase the variance explained to 11.56%. Overall, Model 3 offered the best goodness of fit, the following significant variables correlating with the PTGI-SF score: Younger age, increase in the number of meaningful conversations, those perceiving an increase in loneliness, and those perceiving a decrease in loneliness.
Table 3. Variables Associated with Post-Traumatic Growth: Hierarchical Multiple Regression
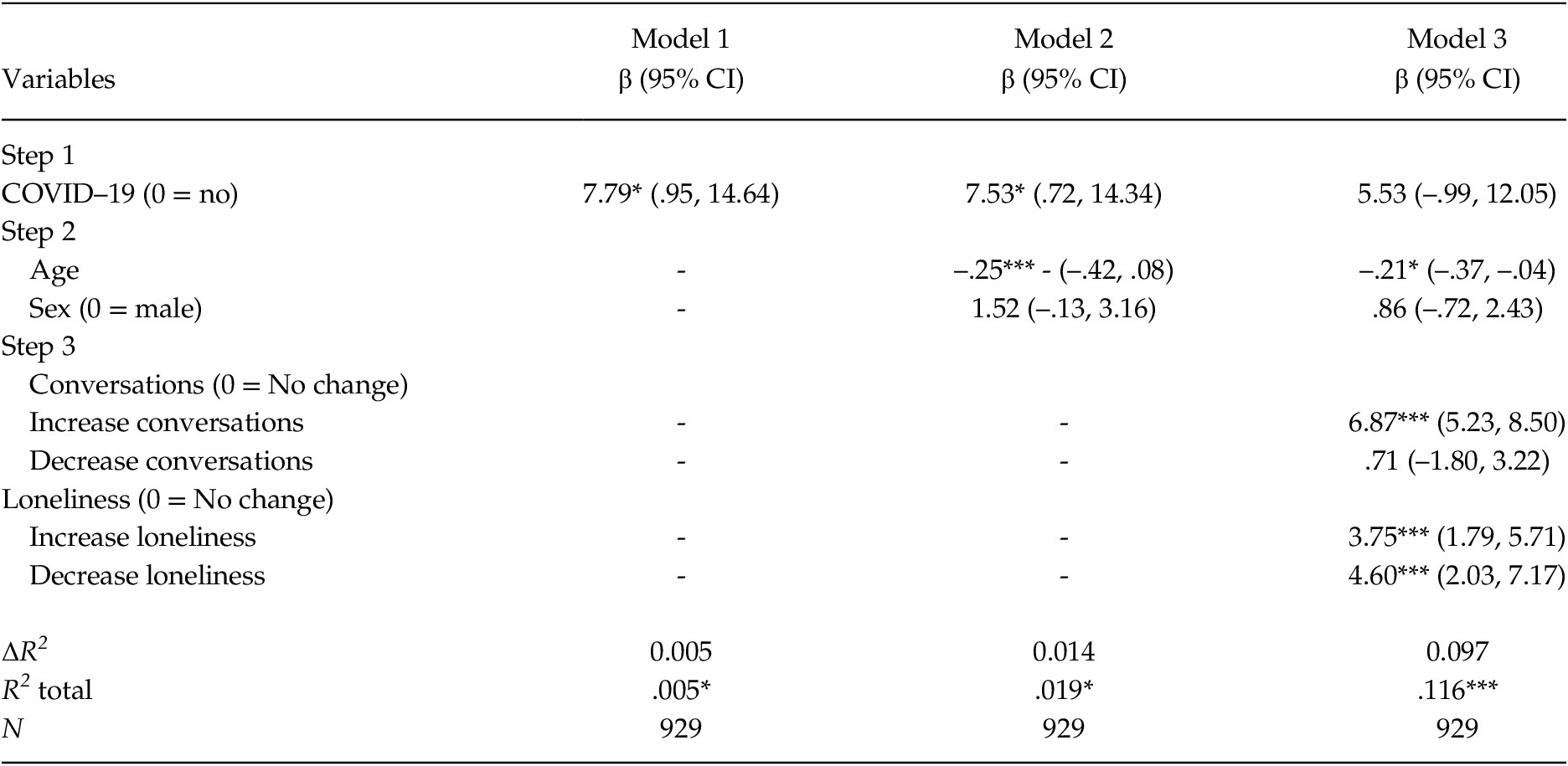
Note. *p < .05. **p < .01. ***p < .001.
Discussion
The primary aim of this study was to describe PTG in older people in Spain after the forced lockdown due to COVID–19 of March-April 2020. However, it also analyzed if direct experience with the disease, sociodemographic variables, and social resources, such as changes in significant conversations or loneliness, were related to PTG.
Our results show the diversity of PTG in the studied population, but that only a quarter experienced higher PTG values, suggesting that lockdown itself was not the main determinant. Moreover, PTG was not higher among those directly exposed to COVID–19 either because they were infected or they experienced a close death. The nature of the event, its unpredictability, and the lack of previous experience may have affected how the process of PTG occurred. In that sense, an important requisite for PTG seems to be the time needed after the experience to start the necessary cognitive and emotional processes. Given that this pandemic is unique in the modern era, it is unknown how long it would take to see the long-term consequences of the pandemic could in different aspects of life, such as PTG, which was the focus in this research. In fact, many countries continue to struggle with the disease, and although there has been no more forced lockdowns in Spain, people remain unable to carry out daily activities as they did before the pandemic appeared. Therefore, some people may need more time to process the consequences of the pandemic, whether these are positive or negative.
The characteristics of the forced lockdown experienced in Spain may also explain the different focus on specific dimensions of the PTG, such as “Appreciation of life.” As described as “Greater appreciation of life may develop as priorities shift dramatically and the “little things” in life are recognized for their value” (Riffle et al., Reference Riffle, Lewis, Tedeschi and Schulenberg2020, p. 156), this recognition of these “little things” in person’s lives may have been experienced precisely because of the lockdown and all the other major activities in their lives being removed.
Along with the direct experience of COVID–19 and its influence on PTG, we analyzed a set of sociodemographic and personal resources. This analysis showed that only age, the presence of significant conversations, and changes in loneliness were related to PTG. Young-older adults experienced more PTG consistent with previous research supporting this correlation (Sim et al., Reference Sim, Lee, Kim and Kim2015; Wu et al., Reference Wu, Kaminga, Dai, Deng, Wang, Pan and Liu2019). However, those studies compared only younger and older adults, while the present research found the same negative tendency when focusing on older adults alone. The ease and necessity of making life adjustments in the young-older adults and the ease with which young-older adults resumed their routines and social activities could explain the age differences in PTG, as other studies have also suggested (Sawyer et al., Reference Sawyer, Ayers and Field2010). For example, more than a year and half after the outbreak of the pandemic, many activities designed for older adults have still not reopened fully in Spain. Also, the older the person, the greater the exposure to the media message of vulnerability and the greater the fear of the disease. Therefore, even though social restrictions are being relaxed, these older adults still perceive the risk and do not regard the event as being over. These fears represent a major obstacle to the appearance of PTG. More studies are needed in the oldest old generation to understand more deeply the cognitive, affective, and social mechanisms that generate lower PTG in this population.
Other elements considered in this study could shed light on the diversity in PTG. One is the increase in amount of significant conversation. This variable was one of the core elements in Tedeschi and Calhoun’s (Reference Tedeschi and Calhoun2004) model of PTG. Having the opportunity to be involved in profound and significant conversations with important emotional or cognitive depth about the pandemic, fears of the disease, and how to face the future can trigger the necessary cognitive mechanisms to express PTG in a person.
Loneliness has been a direct consequence of the lockdown and the social changes to reduce the infection rates. Being prevented from social gatherings, visiting relatives or friends, or outdoor activities could directly affect the sense of loneliness and social isolation. This is especially relevant to Mediterranean countries such as Spain where those social activities are valuable to citizens (Fokkema et al., Reference Fokkema, De Jong Gierveld and Dykstra2012). However, it was not the presence or absence of loneliness during lockdown, but the changes in this feeling, that affected PTG. It was the presence of a change in social relationships, not whether that change was positive or negative, that was most important. The change in equilibrium is what appears to be key to making people view their life or value their relationships differently, ultimately triggering feelings of PTG. On the one hand, the experience of loneliness has usually been portrayed negatively, but some studies have looked at solitude, seeking to focus on the positive impact of being or feeling alone (Lay et al., Reference Lay, Pauly, Graf, Mahmood and Hoppmann2020; Ost Mor et al., Reference Ost Mor, Palgi and Segel-Karpas2020).
This solitude is described as the experience when someone needs to do an introspection task or take time to oneself to decide on goal or lifestyle changes (Lay et al., Reference Lay, Pauly, Graf, Mahmood and Hoppmann2020; Ost Mor et al., Reference Ost Mor, Palgi and Segel-Karpas2020). This sense of solitude is precisely what the person needs to for PTG and could explain why some people who experienced increased loneliness still experienced high levels of PTG. On the other hand, those who experienced reduced loneliness during lockdown may have benefited from closer social relationships and experiencing more opportunities for social support and listening. In turn, these factors may have helped both groups to appreciate their lives and social relationships more, thereby contributing to PTG.
Some limitations of this study must be taken into account to understand the implications of those results and its replicability. First, the study took place just immediately after the 49 days of forced lockdown in Spain, so more time may be needed for PTG to develop. Further studies are therefore needed to follow this immediate scenario and clarify how older adults have adapted to new restrictions and new forms of social relationships. Secondly, the results of the multiple linear regression analysis indicate that a high percentage of the variance remains unexplained. Although the study included relevant variables that have been associated with PTG in previous studies, the unique experience of COVID–19 makes it important to explore other personal and social resources that might provide a better explanation of this personal growth after the pandemic. The use of only a few items to evaluate social resources and the impact of Covid is another limitation of this study. Further analyses with validated scales of loneliness or perceived support, as well as Covid-specific instruments (e.g., The Fear of Covid scale; Ahorsu et al., Reference Ahorsu, Lin, Imani, Saffari, Griffiths and Pakpour2020) may help to explore in more detail how PTG appears after COVID–19. Finally, all participants were obtained by convenience sampling at the University of the Third Age, so our results cannot be extrapolated directly to all older adults. Students at this university tend to be better educated, in better health, and have a broader social network than older people in general (Villar, Reference Villar and Formosa2019). However, it is precisely this group that has probably seen the most drastic changes in their routines and lifestyles. This makes them an interesting population to follow the long-term consequences of social measures if they cannot continue as normal with life projects or other aspects of healthy aging (World Health Organization [WHO], 2015).
In conclusion, this study has shed light on our understanding of the psychological effects of the COVID pandemic on the older population. The results highlight the importance of social relationships and the experience of loneliness as facilitators of PTG in the medium- or long-term. These data have practical implications for the design of interventions aimed at reducing social isolation and loneliness during periods in which physical distancing measures are in place. These interventions can benefit from the inclusion of elements that promote growth and learning among older adults (Williams et al., Reference Williams, Townson, Kapur, Ferreira, Nunn, Galante, Phillips, Gentry and Usher-Smith2021). Indeed, many older adults attend the University of Experience in order to make friends, socialize and broaden their social network (Menéndez et al., Reference Menéndez, Pérez-Padilla and Maya2018). Therefore, our results may also have practical implications for the administration of educational programs of this kind. These programs could allow participants to meet face-to-face in smaller groups or use their current online classes to create group dynamics outside the educational contexts that allow students to share their concerns regarding the pandemic. The results also show the importance of viewing older adults as agents of positive change, resilience, and plasticity. It is essential that we have a more balanced and diverse vision of how older adults have faced the COVID–19 pandemic, often successfully overcoming the focus on negative effects in their age group.




 Open access
Open access