


Introduction
The United States is comprised of diverse populations whose members speak over 350 languages (Dietrich and Hernandez Reference Dietrich and Hernandez2022). Approximately 22% of the U.S. population 5 years or older speak a language other than English at home; 19% of this population report they speak English “not well” or “not at all,” or have limited English proficiency (LEP) (Dietrich and Hernandez Reference Dietrich and Hernandez2022). It is well documented that individuals with LEP experience significant health-care disparities compared to their English-speaking counterparts in both pediatric and adult populations, and across the health-care continuum (Flores et al. Reference Flores, Abreu and Tomany-Korman2005; Jacobs et al. Reference Jacobs, Karavolos and Rathouz2005; Karliner et al. Reference Karliner, Kim and Meltzer2010; Schenker et al. Reference Schenker, Karter and Schillinger2010; VanderWielen et al. Reference VanderWielen, Enurah and Rho2014). Additionally, people with LEP are more likely to be part of racial, ethnic, or cultural minorities, putting them at even higher risk to experience health-care disparities (Sentell and Braun Reference Sentell and Braun2012). Patients with LEP have been shown to have a higher risk of harm from medical errors, fewer physician visits, and lower vaccination rates (Divi et al. Reference Divi, Koss and Schmaltz2007; Fiscella et al. Reference Fiscella, Franks and Doescher2002). These disparities extend to palliative care with lower rates of advance care planning, poorer pain assessment and management, and lower hospice utilization among this population (Abedini et al. Reference Abedini, Downey and Engelberg2022; Payson et al. Reference Payson, Pulido and San Martin2022; Rahemi and Jarrín Reference Rahemi and Jarrín2023; Silva et al. Reference Silva, Genoff and Zaballa2016).
Addressing health disparities is essential to creating an equitable health-care system, and the use of highly skilled professional interpreters is an important part in achieving that goal (VanderWielen et al. Reference VanderWielen, Enurah and Rho2014). Despite patients’ legal right to interpretation services, there is little regulation surrounding the quality of these services. Often bilingual family members or untrained hospital staff members are often utilized as ad hoc interpreters inappropriately (Chen et al. Reference Chen, Youdelman and Brooks2007; Silva et al. Reference Silva, Genoff and Zaballa2016). The use of ad hoc interpreters often contributes to culturally insensitive care and errors in medical interpretation that cause harm (Diamond et al. Reference Diamond, Wilson-Stronks and Jacobs2010; Flores et al. Reference Flores, Abreu and Barone2012). Professional interpreters, on the other hand, have specialized training, certifications, and adhere to a code of ethics that guide their practice (Certification Commission for Healthcare Interpreters 2016; National Board of Certification for Medical Interpreters 2023; The National Council on Interpreting in Health Care 2004). Their training and skills allow them to contribute to quality care for patients with LEP not only through interpretation but also by helping clinicians provide culturally sensitive care and advocating for patients (Hsieh and Kramer Reference Hsieh and Kramer2012; Latif et al. Reference Latif, Makuvire and Feder2022b; Wu and Rawal Reference Wu and Rawal2017).
Unfortunately, the role skilled medical interpreters play in palliative care is poorly defined, even though the benefits have been well documented (Sleptsova et al. Reference Sleptsova, Hofer and Morina2014). Given the communication benefits of utilizing skilled medical interpreters when caring for patients with LEP, interpreters are imperative to providing palliative care in assuring quality, meaningful communication, and culturally sensitive care. When professional interpreters are not utilized to care for palliative care patients with LEP, patients experience poor symptom management and poor understanding of their disease and prognosis (Silva et al. Reference Silva, Genoff and Zaballa2016). Medical interpreters not only interpret nuanced language but also interpret tone, navigate complicated cultural dynamics, and act as the emotional conduit during difficult conversations for these patients (Norris et al. Reference Norris, Wenrich and Nielsen2005; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Genoff and Zaballa2016). Given these complex responsibilities of medical interpreters in palliative care, their roles and experiences are unique and have not been explored in previous reviews. This narrative review examines the extant literature regarding the unique role and experiences of medical interpreters in palliative care.
Methods
A narrative review approach was chosen to analyze the extant literature and provide insight into the role and experiences of medical interpreters in palliative care. The searches were conducted from March to April 2023 in the following databases: Medline, Embase, Web of Science, and CINHAL. Title and abstract screening were completed, followed by a full-text review against the inclusion and exclusion criteria, and articles were identified for inclusion in the review. Finally, a citation search of each included article was conducted. Each citation of the included articles was screened, and relevant articles were included in the review. This broad search strategy ensured that relevant literature from a variety of disciplines was captured, and the full breadth of literature was explored.
The search terms that were included combined limited English proficiency, medical interpreter, OR translation AND palliative OR end-of-life care. The searches were translated and edited to utilize the appropriate subject headings in each database. The search details are available in Table 1. To ensure the extant literature was included, no date restrictions were added. Articles solely focused on the impact of medical interpreters in palliative care on patient experience or outcomes were excluded given that previous reviews have examined their impacts (Silva et al. Reference Silva, Genoff and Zaballa2016). Full inclusion and exclusion criteria are outlined in Table 2.
Search terms

Inclusion and exclusion criteria

Results
The search yielded 358 results from 4 databases. Duplicates were removed (n = 129) and title and abstract screening was completed for the remaining articles (n = 229). Irrelevant articles were removed, and a full-text review was completed (n = 52). Nine articles were identified for inclusion in the review based on the inclusion and exclusion criteria. The other articles (n = 43) were excluded mainly because they did not discuss the population of interest or lack of full text (e.g. poster abstracts). Citation mining was completed for the 9 included articles. All references for each article and any article that referenced an included article were added to the search (n = 419). Again, duplicates were removed (n = 179) and the title and abstract screening was completed (n = 240). Five articles were identified for further full-text review. One additional article was included in the review with the other remaining articles (n = 4) excluded as they did not target the population of interest. See Figure 1 for flowchart of the review process.
Review Flow Diagram.

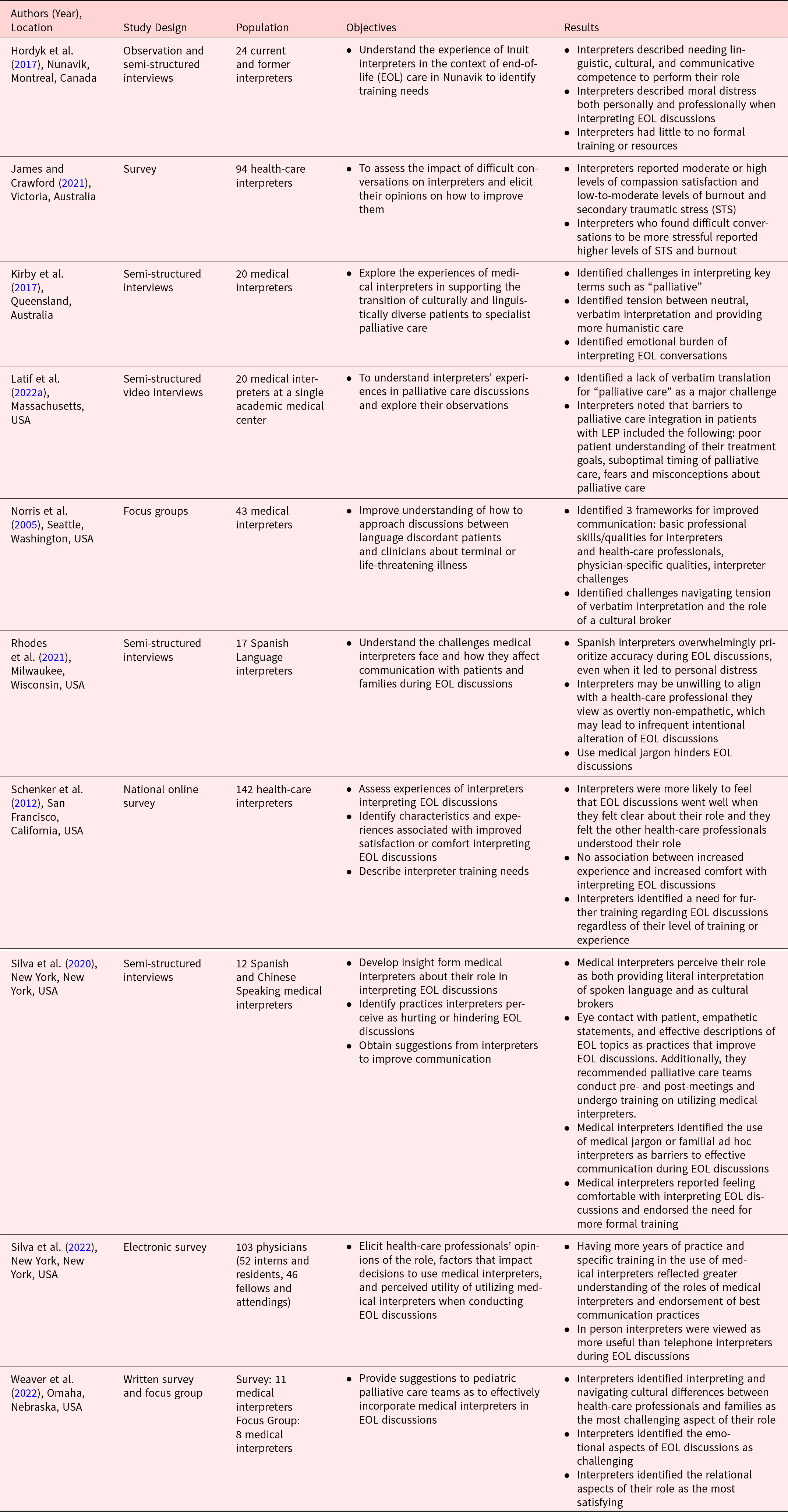
The 10 studies included in this review are all studies published in peer-reviewed journals. They utilized 1 or more of the following data collection techniques: semi-structured interviews (n = 5) (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; Kirby et al. Reference Kirby, Broom and Good2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Silva et al. Reference Silva, Tsai and Sobota2020), surveys (n = 4) (James and Crawford Reference James and Crawford2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Adelman and Singh2022; Weaver et al. Reference Weaver, Roeth and Navaneethan2022), focus groups (n = 2) (Norris et al. Reference Norris, Wenrich and Nielsen2005; Weaver et al. Reference Weaver, Roeth and Navaneethan2022), and observation (n = 1) (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017). Most of the studies included examined the perspectives of the medical interpreters themselves (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; James and Crawford Reference James and Crawford2021; Kirby et al. Reference Kirby, Broom and Good2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Norris et al. Reference Norris, Wenrich and Nielsen2005; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022), while 1 study analyzed the perspectives of both training and attending level physicians (Silva et al. Reference Silva, Adelman and Singh2022). In the 9 studies that focused on medical interpreters’ perspectives, the interpreters worked with patients who spoke a wide range of languages, with the most common being Spanish (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; James and Crawford Reference James and Crawford2021; Kirby et al. Reference Kirby, Broom and Good2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Norris et al. Reference Norris, Wenrich and Nielsen2005; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Additionally, interpreters who provide in-person, phone, and video interpretation were examined in the studies included in this review; however, the majority of interpreters provided in-person interpretation (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; James and Crawford Reference James and Crawford2021; Kirby et al. Reference Kirby, Broom and Good2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Norris et al. Reference Norris, Wenrich and Nielsen2005; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). See Table 3 for a brief description of the included studies.
Brief description of included articles

In analyzing the included articles, 3 overarching themes were generated: the roles of medical interpreters in the care of palliative care patients with LEP, the experiences of medical interpreters in caring for palliative care patients, and recommendations from interpreters to improve communication with palliative care patients with LEP. Within these 3 overarching themes, additional subthemes were identified and are discussed in the subsequent sections.
The roles of the medical interpreter in palliative care
It is clear from the literature included in this review that medical interpreters are not simply word-for-word conduits of communication. Instead, they play many vital roles in the care of patients with LEP. In analyzing the extant literature, 3 roles emerged: interpreting language and meaning, acting as a cultural broker, and advocating for patients and families.
Interpreting language and meaning
Acting as a conduit for language and interpreting health-care professionals’ messages accurately was the most commonly identified role of medical interpreters by health professionals and interpreters alike (Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Silva et al. Reference Silva, Adelman and Singh2022, Reference Silva, Tsai and Sobota2020). In semi-structured interviews, interpreters reported that literal interpretation of spoken language and delivering the messages of health-care professionals accurately was their highest priority even in the face of personal discomfort (Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021). Content alterations were reported to be rare and intended to improve communication and understanding (Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021). In situations where interpreters intentionally alter content, as Rhodes et al. examined, it was not reported to be motivated by an individual interpreter’s values or beliefs. These additions and clarifications were described as transparent communications with both the professionals and patients, which is consistent with how interpreters approached similar situations in the other studies (Norris et al. Reference Norris, Wenrich and Nielsen2005; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Weaver et al. Reference Weaver, Roeth and Navaneethan2022).
However, a unique challenge that interpreters face in their role as a language conduit in discussions regarding palliative care topics is the lack of verbatim translation for terms such as “palliative care” and “hospice” (Kirby et al. Reference Kirby, Broom and Good2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020). For example, 1 Spanish interpreter discussed how hospice translated to “hospicio,” which in Spanish means orphanage or poorhouse (Schenker et al. Reference Schenker, Fernandez and Kerr2012). There was wide variability in how this lack of verbatim translation was handled by the interpreters depending on their level of experience, knowledge of palliative care, and comfort level interpreting end-of-life discussions (Kirby et al. Reference Kirby, Broom and Good2017; Silva et al. Reference Silva, Tsai and Sobota2020).
Acting as a cultural broker
All of the studies identified in this review addressed the role of the interpreter as a cultural broker in discussions about palliative care topics (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; James and Crawford Reference James and Crawford2021; Kirby et al. Reference Kirby, Broom and Good2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Norris et al. Reference Norris, Wenrich and Nielsen2005; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Adelman and Singh2022, Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Acting as a cultural broker entailed providing cultural context and navigating perceived cultural differences between the palliative care team and patients or caregivers (Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Through this work, interpreters reported providing increased understanding of diverse cultures and values as well as increased accuracy of all types of communications (Norris et al. Reference Norris, Wenrich and Nielsen2005; Silva et al. Reference Silva, Tsai and Sobota2020).
Interpreters who participated in the included studies acknowledged that values and beliefs surrounding death and dying are deeply rooted in the culture of a patient and their family (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; Kirby et al. Reference Kirby, Broom and Good2017; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). For example, in a study of Spanish- and Chinese-speaking interpreters, they discussed that conversations surrounding death and dying are often viewed as disrespectful (Silva et al. Reference Silva, Tsai and Sobota2020). In another study of Inuit interpreters, they discussed that delivering news of a terminal illness or death is a task typically assigned to a community leader or elder, and being asked to deliver that news as an interpreter was contradictory to local customs (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017). In 1 study, interpreters identified navigating these culturally differences as the most challenging part of their role (Weaver et al. Reference Weaver, Roeth and Navaneethan2022).
Advocating for patients and caregivers
Given their understanding of both the patient and health-care professional perspectives, interpreters in the included studies identified their unique opportunity to act as advocates for patients and their caregivers (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; Kirby et al. Reference Kirby, Broom and Good2017; Norris et al. Reference Norris, Wenrich and Nielsen2005; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Interpreters in 1 study even reported that sharing a culture or language fosters a sense of partnership between the interpreter and patient (Silva et al. Reference Silva, Tsai and Sobota2020). Examples of interpreter advocacy were discussed in several of the studies included in this review. They alerted professionals and patients of miscommunication and ensured patients and caregivers had clarity (Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Additionally, interpreters reported they addressed patients’ and families’ fears and misconceptions surrounding palliative care and managed the interpretation of terms with poor verbatim translation by eliciting expanded explanations from professionals (Kirby et al. Reference Kirby, Broom and Good2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Silva et al. Reference Silva, Tsai and Sobota2020).
The lived experience of medical interpreters in palliative care
While each palliative care encounter is unique, medical interpreters reported some similar experiences across several studies included in this review. The 2 main subthemes that were identified regarding the experiences of medical interpreters participating in palliative care discussions were the difficulties associated with navigating their complex roles and the emotional impact of participating in the encounters.
Navigating complex roles
Across several included studies, interpreters reported feeling that the roles of language conduit, cultural broker, and patient advocate can be at odds and sometimes even present moral or ethical dilemmas for the interpreter to navigate (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; Kirby et al. Reference Kirby, Broom and Good2017; Norris et al. Reference Norris, Wenrich and Nielsen2005; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Interpreters reported better experiences interpreting discussions about palliative care topics when they felt both they and health-care professionals had an understanding of the roles of the medical interpreter in an encounter (Schenker et al. Reference Schenker, Fernandez and Kerr2012). In the study of health-care professionals, it was found that palliative care training, greater number of years in practice, and training in the use of medical interpreters lead to an increased awareness of the roles of medical interpreters (Silva et al. Reference Silva, Adelman and Singh2022). Additionally, navigating these complex roles can lead to a sense of professional and emotional distress (Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021). A lack of understanding of these complex challenges faced by medical interpreters was demonstrated to contribute to frustration from all participants and poor communication (Norris et al. Reference Norris, Wenrich and Nielsen2005).
Emotional impact of interpreting palliative care discussions
Despite the complicated dynamic that interpreters face in palliative care discussions, interpreters reported feeling comfortable interpreting palliative care–related discussions (Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). For example, all of the interpreters interviewed in Silva et al. reported feeling comfortable interpreting for palliative care discussions, and 85% of respondents in Schenker et al. reported the same. In Weaver et al. (Reference Weaver, Roeth and Navaneethan2022), interpreters in a pediatric hospital reported their comfort level with interpreting goals of care, symptom management, and psychosocial content at 7.2 of 10 and 8 of 10 for pediatric patients and their families, respectively. Additionally, 9 of 11 interpreters reported that they would willingly be assigned to interpret serious news (Weaver et al. Reference Weaver, Roeth and Navaneethan2022).
Even though interpreters reported feeling comfortable performing the task of interpreting in palliative care discussions, interpreters in 6 studies included in this review acknowledged the emotional impact of interpreting palliative care discussions (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; Kirby et al. Reference Kirby, Broom and Good2017; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Interpreters reported performing the role of an interpreter in conversations regarding palliative care issues is more stressful and requires compartmentalization or suppression of their of emotions (Kirby et al. Reference Kirby, Broom and Good2017; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020). The emotional burden of the conversations was reported to have been a result of both the content of the conversations and the emotional intensity of the participants (Weaver et al. Reference Weaver, Roeth and Navaneethan2022). They also reported that they felt they needed support, but did not have an outlet to process their emotions and often thought about the conversations for some time after they were over (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; Kirby et al. Reference Kirby, Broom and Good2017; Schenker et al. Reference Schenker, Fernandez and Kerr2012).
Recommendations of medical interpreters
All of the studies focused on the perspectives of medical interpreters included in this review elicited insights and recommendations from the participants to enhance communication with palliative care patients with LEP when utilizing medical interpreters (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; James and Crawford Reference James and Crawford2021; Kirby et al. Reference Kirby, Broom and Good2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Norris et al. Reference Norris, Wenrich and Nielsen2005; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Many of the recommendations focused on the language choice of the health-care professionals. Interpreters recommended avoiding the use of medical jargon such as “palliative” and “hospice” (Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020). Instead, interpreters recommend having an effective description of these terms utilizing lay language (Kirby et al. Reference Kirby, Broom and Good2017; Norris et al. Reference Norris, Wenrich and Nielsen2005; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Interpreters also recommended avoiding the use of metaphors or analogies, which can be common when describing death and dying, as they often do not translate well into other languages (Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Weaver et al. Reference Weaver, Roeth and Navaneethan2022).
Outside their recommendations surrounding language, the most common recommendation for health-care professionals was conducting a pre-meeting and debrief with the interpreter and the medical team (James and Crawford Reference James and Crawford2021; Norris et al. Reference Norris, Wenrich and Nielsen2005; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Pre-meetings offer an opportunity to help prepare interpreters for difficult topics, to clarify language and topics, and for the palliative care team to gain the interpreter’s insight into important information about the patient, family, or culture (James and Crawford Reference James and Crawford2021; Norris et al. Reference Norris, Wenrich and Nielsen2005; Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Tsai and Sobota2020; Weaver et al. Reference Weaver, Roeth and Navaneethan2022). Debriefs following the encounter provide a venue for interpreters and other health-care professionals to process difficult conversations as a team and offer each other support (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017). They also allow interpreters to provide the team with feedback or insights regarding patient comprehension or cultural considerations for subsequent visits (Rhodes et al. Reference Rhodes, Fletcher and Blumenfeld-Kouchner2021).
Many interpreters identified the need for further education and training both for the medical interpreters themselves and for health-care professionals (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; Kirby et al. Reference Kirby, Broom and Good2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Schenker et al. Reference Schenker, Fernandez and Kerr2012; Silva et al. Reference Silva, Adelman and Singh2022). The medical interpreters identified their need for education in palliative care and navigating difficult conversations and ethical dilemmas (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; Latif et al. Reference Latif, Makuvire and Feder2022a; Schenker et al. Reference Schenker, Fernandez and Kerr2012). For other health-care professionals, medical interpreters discussed the need for education regarding communication skills when working with medical interpreters (Hordyk et al. Reference Hordyk, Macdonald and Brassard2017; Kirby et al. Reference Kirby, Broom and Good2017; Silva et al. Reference Silva, Adelman and Singh2022). Finally, interpreters suggested introducing and treating the medical interpreter as an integral member of the health-care team (Norris et al. Reference Norris, Wenrich and Nielsen2005; Silva et al. Reference Silva, Adelman and Singh2022; Weaver et al. Reference Weaver, Roeth and Navaneethan2022).
Discussion
The literature in this review demonstrates that medical interpreters play many roles when interpreting palliative care discussions, including interpreting language and meaning, acting as a cultural broker, and advocating for patients and families. These roles are both distinct and overlapping, and the navigation of these roles is nuanced. Given the complicated nature of interpreting palliative care conversations, it is imperative that certified interpreters are utilized and that these interpreters are both educated about the elements of palliative care and empowered by the team in their roles. Norris et al. (Reference Norris, Wenrich and Nielsen2005) argued that interpreters should not be considered solely a linguistic conduit, but should be “semiautonomous.”. This autonomy recognizes the expertise interpreters offer in the care of patients with LEP and allows them to utilize their skills to provide high-quality patient care.
Part of empowering and supporting medical interpreters is integrating them more fully as members of the medical team during palliative care discussions. Palliative care professionals are well aware of the benefits of an interprofessional approach to caring for individuals, and for patients with LEP the medical interpreter should be considered a vital part of that interprofessional team (Crawford and Price Reference Crawford and Price2003). This can be done through including interpreters in pre-meetings and eliciting their insight and expertise, empowering them to address concerns during the encounter, as well as offering opportunities to debrief with the team following encounter. Additionally, fully integrating medical interpreters into the interprofessional team includes attending to the emotional and moral distress that interpreters may feel during palliative care encounters. Both this review and other recent reviews demonstrate the wide range of emotional reactions and experiences interpreters can experience when participating in palliative care discussions (Hancox et al. Reference Hancox, McKiernan and Martin2023).
Limitations
This narrative review is limited due to the relatively small and heterogenous nature of the literature examining the role and experiences of medical interpreters in palliative care. While palliative care presents unique challenges for medical interpreters, by only including articles focused on the role of the interpreter in palliative care, foundational articles discussing the role and experiences of medical interpreters may have been eliminated. Additionally, the articles in this review primarily examined the role of medical interpreters in palliative care from the perspective of medical interpreters themselves. Only a single study examined the role of interpreters from the perspective of palliative care professionals, and the only professionals included in that study were physicians who were not representative of the larger interprofessional team necessary for holistic palliative care. To mitigate the potential bias that may be introduced by a single researcher, content experts, interprofessional palliative care researchers, and research librarians were consulted in the development, conducting, and synthesis of this review.
Future research
While literature regarding the utilization, experiences, and roles of medical interpreters in palliative care is growing, there are many opportunities to expand and build upon the extant literature. Given the diversity of interpreters participating in most studies, it is unclear how the findings may differ between specific languages and cultures. Increased research into how language and culture may impact interpreters’ roles and experiences is warranted. Additionally, there is little information regarding patient or family factors that may impact the experience of medical interpreters in palliative care. Factors such as patient age and presence of surrogate decision makers are underexplored. Finally, increased work is needed to accurately measure the impact of interpreting palliative care discussions on interpreters as very limited quantitative research utilizing validated measurement tools has been done in this area.
To integrate interpreter recommendations within palliative care, there has been development of formal communication models and education for interpreters (Barwise et al. Reference Barwise, Yeow and Partain2021; Goldhirsch et al. Reference Goldhirsch, Halpenny and Scott2021). However, this work is in its infancy and most of the recommendations are consensus based rather than tested. This includes how implementation of recommendations impact interpreters’ experience and patient outcomes. More research is needed to test how adopting and integrating interpreter recommendations impacts the interprofessional team, including interpreters, and patient outcomes for palliative care patients with LEP.
Conclusion
Medical interpreters in palliative care are essential for patients with LEP. They play several roles including interpreting language and meaning, acting as a cultural broker, and advocating for patients and families. These roles often overlap and interact making them difficult to navigate and ultimately impacting the experience of medical interpreters participating in palliative care discussions. This review highlights the need to integrate medical interpreters into the broader interprofessional palliative care team to support them in performing their many roles and attend to the array of emotional reactions and distress they may experience. Further research into how to best achieve this and how it impacts both interpreters and patients is vital. This review may act as a basis for future research.
Acknowledgments
The author would like to thank the many people who provided assistance and encouragement in the development and execution of this review. The author thanks Andy Hickner (Weill Cornell Medicine), Dr. Isabell May (University of Maryland, Baltimore), Dr. Lynn McPherson (University of Maryland, Baltimore), Constance Dahlin (University of Maryland, Baltimore), Patricia Wright (University of Scranton), and Stephen Douglas for their insight and expertise.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The author declared no potential conflicts of interest with respect to research, authorship, and/or publication of this article.



 Open access
Open access