
173 results

Building Quantum Computers
- A Practical Introduction
- Coming soon
-
- Expected online publication date:
- September 2024
- Print publication:
- 11 July 2024
-
- Textbook
- Export citation
Characteristics of healthcare personnel with SARS-CoV-2 infection: 10 emerging infections program sites in the United States, April 2020–December 2021
-
- Journal:
- Infection Control & Hospital Epidemiology , First View
- Published online by Cambridge University Press:
- 21 May 2024, pp. 1-9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Potential underreporting of treated patients using a Clostridioides difficile testing algorithm that screens with a nucleic acid amplification test
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 5 / May 2024
- Published online by Cambridge University Press:
- 25 January 2024, pp. 590-598
- Print publication:
- May 2024
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Variations in implementation of antimicrobial stewardship via telehealth at select Veterans Affairs medical centers
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s38
-
- Article
-
- You have access
- Open access
- Export citation
Evaluating racial disparities in central-line–associated bloodstream infections for Tennessee hospitals, 2018–2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s48
-
- Article
-
- You have access
- Open access
- Export citation
Factors associated with high influenza vaccination among healthcare workers in Tennessee acute-care hospitals, 2014–2022
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s73
-
- Article
-
- You have access
- Open access
- Export citation
Susceptibility results discrepancy analysis between NHSN antimicrobial resistance (AR) Option and NEDSS Base System in Tennessee, July 2020–December 2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s104
-
- Article
-
- You have access
- Open access
- Export citation
Characterization of negative health outcomes for dialysis events by vascular access type—Tennessee, 2015–2019
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s64
-
- Article
-
- You have access
- Open access
- Export citation
-
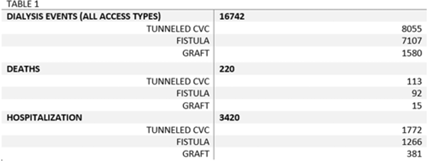
Background: The dialysis patient population is at a higher risk for nosocomial infections as well as related negative consequences including hospitalization and death. The CMS and the state of Tennessee mandate reporting of 3 types of dialysis events: positive blood culture, intravenous antimicrobial starts, and pus, redness, or increased swelling at the access site. We explored hospitalization and death outcomes by vascular access types for dialysis events reported to the NHSN for licensed outpatient hemodialysis clinics in Tennessee from 2015 to 2019. Methods: We looked at the frequency of hospitalization and death among those who experienced a dialysis event for 3 types of vascular access: arteriovenous fistula, arteriovenous graft, and tunneled central venous catheter (CVC). Other vascular-access types were excluded due to low usage rates. Odds ratios and confidence intervals were used to quantify the relationship between access type and hospitalization, and access type and death. Pooled analysis was used due to the stable rates of death and hospitalization among access types from 2015 to 2019. Results: From 2015 to 2019, 16,742 dialysis events were reported for the 3 access types: 8,055 dialysis events (48.1%) occurred among those with tunneled CVCs, 7,107 (42.5%) occurred among those with fistulas, and 1,580 (9.4%) occurred among those with grafts. Of the 16,742 dialysis events, 3,420 patients (20.4%) were hospitalized either due or related to their dialysis event; 220 (1.3%) deaths occurred either due to or related to the patient’s dialysis event. The odds of being hospitalized was 1.47 (95% CI, 1.29–1.67) times greater in those with grafts compared to those with fistulas. Patients with tunneled CVCs were 1.30 (95% CI, 1.20–1.41) times greater to be hospitalized compared to those with fistulas. The odds of death was 1.09 (95% CI, 0.9–2.5) times greater in those patient with tunneled CVCs compared to those with fistulas, whereas the odds of death among patients with grafts was 0.73 (95% CI, 0.82–1.43) times the odds of death compared to patients with fistulas. Conclusions: Overall, our findings conclude hemodialysis patients with tunneled CVCs have an increased risk for the negative health outcomes of hospitalization and death when compared to the other access types, supporting previous studies. Additionally, grafts had a higher risk of hospitalization compared to fistulas, but patients with grafts had lower odds of death than those with fistulas. Further investigation is needed to study how the COVID-19 pandemic may have affected the trends of negative health outcomes related to dialysis events.
Disclosures: None

Epidemiology of carbapenem-resistant and extended-spectrum beta-lactamase-producing Enterobacterales in US children, 2016–2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s16
-
- Article
-
- You have access
- Open access
- Export citation
Using telehealth to support antimicrobial stewardship at four rural VA medical centers: Interim analysis
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s110
-
- Article
-
- You have access
- Open access
- Export citation
-
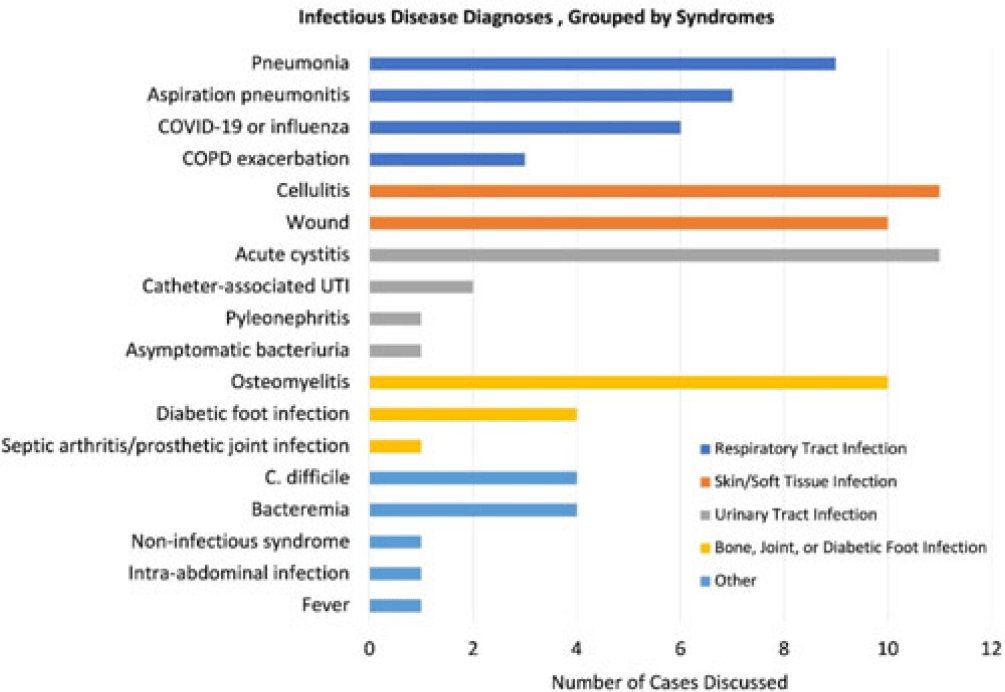
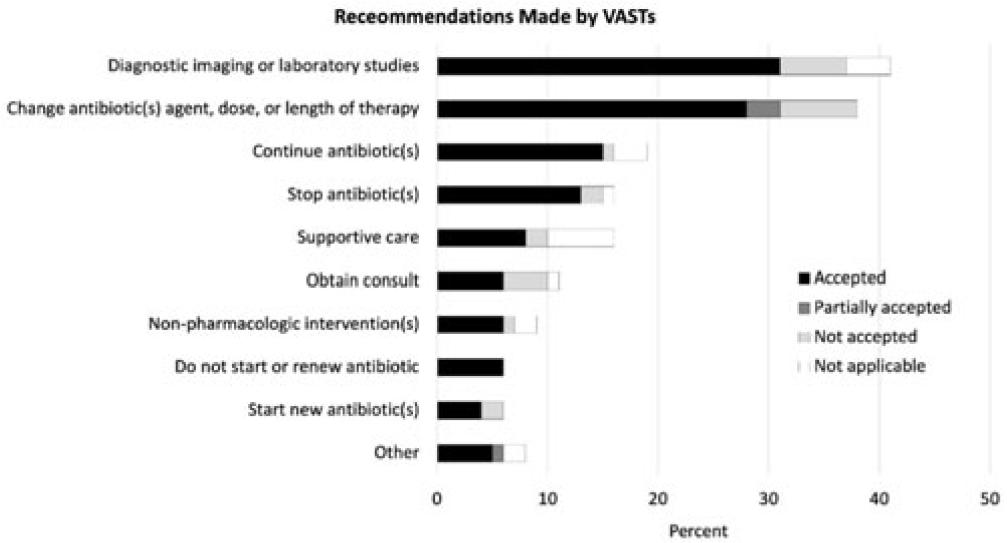
Background: Healthcare settings without access to infectious diseases experts may struggle to implement effective antibiotic stewardship programs. We previously described a successful pilot project using the Veterans Affairs (VA) telehealth system to form a Videoconference Antimicrobial Stewardship Team (VAST) that connected multidisciplinary teams from rural VA medical centers (VAMCs) with infectious diseases experts at geographically distant locations. VASTs discussed patients from the rural VAMC, with the overarching goal of supporting antibiotic stewardship. This project is currently ongoing. Here, we describe preliminary outcomes describing the cases discussed, recommendations made, and acceptance of those recommendations among 4 VASTs. Methods: Cases discussed at any of the 4 participating intervention sites were independently reviewed by study staff, noting the infectious disease diagnoses, recommendations made by infectious diseases experts and, when applicable, acceptance of those recommendations at the rural VAMC within 1 week. Discrepancies between independent reviewers were discussed and, when consensus could not be reached, discrepancies were discussed with an infectious diseases clinician. Results: The VASTs serving 4 different rural VAMCs discussed 96 cases involving 92 patients. Overall, infection of the respiratory tract was the most common syndrome discussed by VASTs (Fig. 1). The most common specific diagnoses among discussed cases were cellulitis (n = 11), acute cystitis (n = 11), wounds (n = 11), and osteomyelitis (n = 10). Of 172 recommendations, 41 (24%) related to diagnostic imaging or laboratory results and 38 (22%) were to change the antibiotic agent, dose, or duration (Fig. 2). Of the 151 recommendations that could be assessed via chart review, 122 (81%) were accepted within 1 week. Conclusions: These findings indicate successful implementation of telehealth to connect clinicians at rural VAMCs with an offsite infectious diseases expert. The cases represented an array of common infectious syndromes. The most frequent recommendations pertained to getting additional diagnostic information and to adjusting, but not stopping, antibiotic therapy. These results suggest that many of the cases discussed warrant antibiotics and that VASTs may use the results of diagnostic studies to tailor that therapy. The high rate of acceptance suggests that the VASTs are affecting patient care. Future work will describe VAST implementation at 4 additional VAMCs, and we will assess whether using telehealth to disseminate infectious diseases expertise to rural VAMCs supports changes in antibiotic use that align with principles of antimicrobial stewardship.
Disclosures: None


Determining trends of respiratory tract infections in a long-term care facility pilot surveillance project
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s24
-
- Article
-
- You have access
- Open access
- Export citation
Increasing Registration for a VA Multidrug-Resistant Organism Alert Tool
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s124-s125
-
- Article
-
- You have access
- Open access
- Export citation
-
Objectives: To address the importation of multi-drug-resistant organisms (MDROs) when a colonized or infected patient is transferred from another VA facility, the Veterans Health Administration (VHA) launched the Inpatient Pathogen Tracker (IPT) in 2020. IPT tracks MDRO-infected/colonized patients and alerts MDRO Program Coordinators (MPCs) and Infection Preventionists (IPs) when such patients are admitted to their facility to facilitate rapid identification and isolation of infected/colonized patients. IPT usage has been low during initial rollout (32.5%). The VHA and the CARRIAGE QUERI Program developed targeted implementation strategies to increase utilization of IPT’s second iteration, VA Bug Alert (VABA). Methods: Familiarity with IPT was assessed via pre-education survey (3/2022). All sites received standard VABA implementation including: 1) adaptation of VABA features based on end-user feedback (completed 4/2022), 2) development and delivery of an educational module regarding the revised tool (completed 4/2022), and 3) internal facilitation from the VHA MDRO Program Office (ongoing) (see Figure for all key timepoints). Intent to register for VABA was assessed via post-education survey (4-5/2022). Sites (125 eligible) not registered for VABA by 6/1/2022 were randomly assigned to receive one of two conditions from 6/2022–8/2022: continued standard implementation alone or enhanced implementation. Enhanced implementation added the following to standard implementation: 1) audit and feedback reports and 2) external facilitation, including interviews and education about VABA. We compared the number of sites with ≥1 MPC/IP registered for VABA to-date between implementation conditions. Results: Pre-education survey. 168 MPC/IPs across 117 sites responded (94% of eligible sites). Among respondents, 25% had used IPT, 35.1% were familiar with but had not used IPT, and 39.9% were unfamiliar with IPT. Post-education survey. 93 MPC/IPs across 80 sites responded (59% of eligible sites). Of these, 81.7% said they planned to register for VABA, 4.3% said they would not register, and 14.0% said they were unsure. Post-6/1/2022 Registrations. By 6/1/2022, 71% of sites had ≥1 registered VABA user. Of the 28 unregistered sites eligible for enhanced implementation, thirteen were assigned to receive enhanced implementation, and fifteen were assigned to receive continued standard implementation. Eight sites in the enhanced implementation condition (61.5%) registered for VABA. Seven standard-implementation-only sites (46.7%) registered. The number of registered sites did not significantly differ by implementation condition (Fisher’s exact p=0.476). Conclusions: Standard and enhanced implementation were equally effective at encouraging VABA registration, suggesting that allocating resources to enhanced implementation may not be necessary.
Disclosures: None.


Chapter 12 - How kings went about accumulating wealth and adding to it
-
- Book:
- The Chronicles of Fernão Lopes
- Published by:
- Boydell & Brewer
- Published online:
- 28 December 2023
- Print publication:
- 20 June 2023, pp 92-94
-
- Chapter
- Export citation
Chapter 15 - The pacts that the King of Castile and King Pedro of Portugal signed and how the King of Portugal promised to support him against Aragon
-
- Book:
- The Chronicles of Fernão Lopes
- Published by:
- Boydell & Brewer
- Published online:
- 28 December 2023
- Print publication:
- 20 June 2023, pp 97-99
-
- Chapter
- Export citation
Chapter 40 - How King Pedro arrived in Galicia, killed the Archbishop of Santiago and departed for England
-
- Book:
- The Chronicles of Fernão Lopes
- Published by:
- Boydell & Brewer
- Published online:
- 28 December 2023
- Print publication:
- 20 June 2023, pp 152-153
-
- Chapter
- Export citation
Chapter 22 - How the year-long truce between the kings came to be broken, and how King Pedro assembled a fleet to wage war on Aragon
-
- Book:
- The Chronicles of Fernão Lopes
- Published by:
- Boydell & Brewer
- Published online:
- 28 December 2023
- Print publication:
- 20 June 2023, pp 116-117
-
- Chapter
- Export citation
Chapter 2 - How the King of Castile sent for the body of Queen Maria, his mother, and concerning the letter he sent to the King of Portugal, his uncle
-
- Book:
- The Chronicles of Fernão Lopes
- Published by:
- Boydell & Brewer
- Published online:
- 28 December 2023
- Print publication:
- 20 June 2023, pp 73-74
-
- Chapter
- Export citation
Translators’ Note
-
- Book:
- The Chronicles of Fernão Lopes
- Published by:
- Boydell & Brewer
- Published online:
- 28 December 2023
- Print publication:
- 20 June 2023, pp xxv-xxviii
-
- Chapter
- Export citation
Bibliography of Works Cited
-
- Book:
- The Chronicles of Fernão Lopes
- Published by:
- Boydell & Brewer
- Published online:
- 28 December 2023
- Print publication:
- 20 June 2023, pp 162-166
-
- Chapter
- Export citation
Chapter 37 - How the King of Castile sent a daughter of his to Portugal, and how he left Seville out of fear of the people of the city
-
- Book:
- The Chronicles of Fernão Lopes
- Published by:
- Boydell & Brewer
- Published online:
- 28 December 2023
- Print publication:
- 20 June 2023, pp 147-148
-
- Chapter
- Export citation
