3 results
Perceptions of an automated benchmarking dashboard for antimicrobial stewardship programs among antimicrobial stewards within the veterans’ health administration: a multicenter qualitative study
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 10 July 2023, e118
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Qualitative Evaluation of an automated nationwide benchmarking antimicrobial utilization dashboard for the VHA
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s4
-
- Article
-
- You have access
- Open access
- Export citation
-
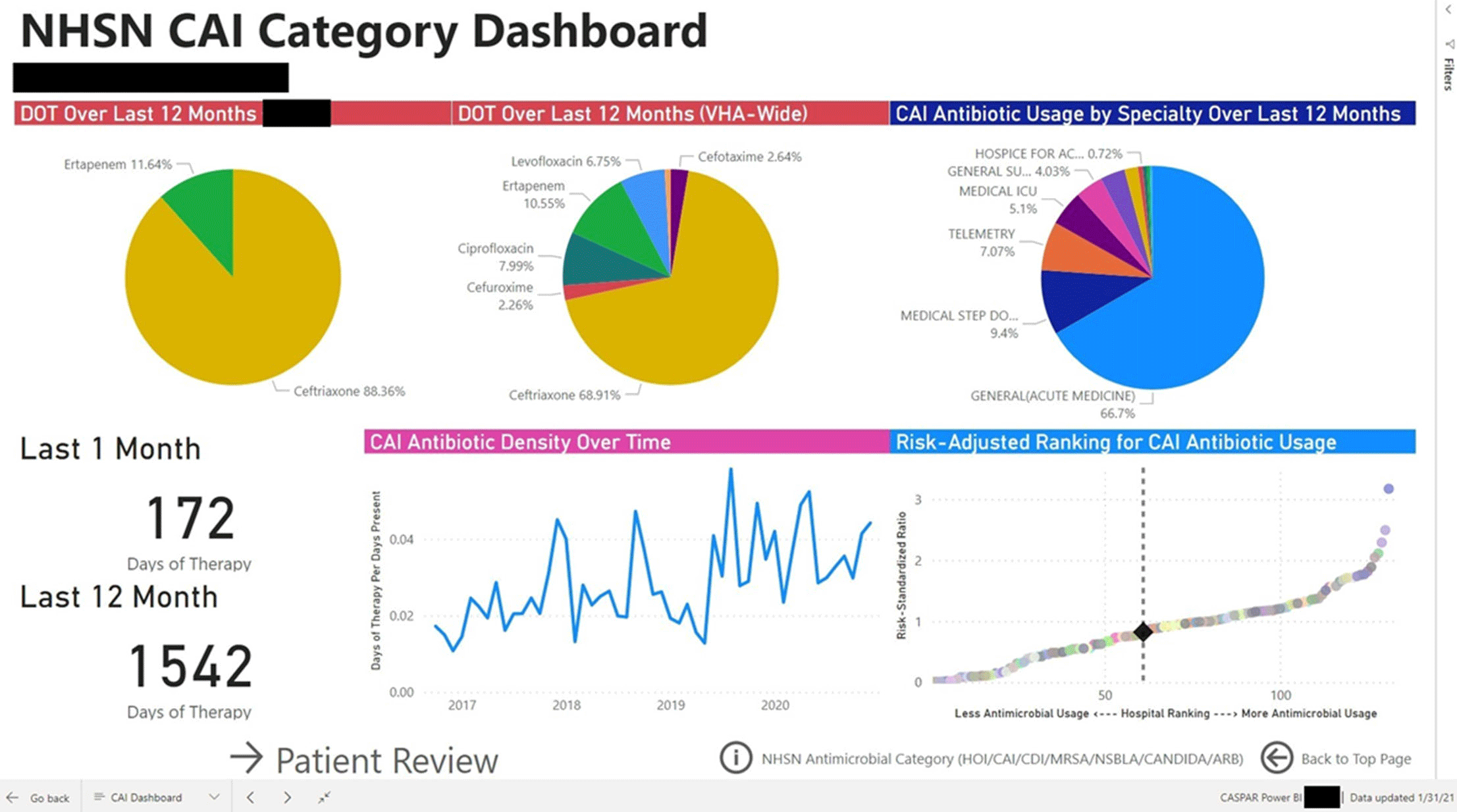
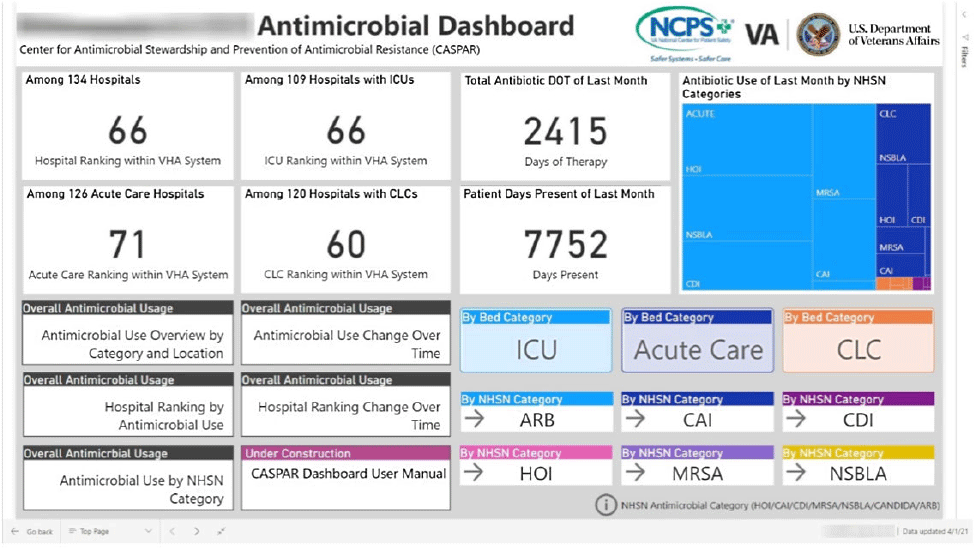
Background: Antimicrobial stewardship programs (ASPs) are advised to audit antimicrobial consumption as a metric to feedback to clinicians. However, many ASPs lack the tools necessary for appropriate risk adjustment and standardized data collection, which are critical for peer-program benchmarking. We evaluated the impact of the dashboard deployment that displays these metrics and its acceptance among ASP members and antimicrobial prescribers. Materials/methods: We conducted semistructured interviews of ASP stewards and antimicrobial prescribers before and after implementation of a web-based ASP information dashboard (Fig. 1) implemented in the VA Midwest Health Care Network (VISN23). The dashboard provides risk-adjusted benchmarking, longitudinal trends, and analysis of antimicrobial usage patterns at each facility. Risk-adjusted benchmarking was based on an observed-to-expected comparison of antimicrobial days of therapy at each facility, after adjusting for differences in patient case mix and facility-level variables. Respondents were asked to evaluate several aspects of the dashboard, including its ease of use, applicability to ongoing ASP activities, perceived validity and reliability, and advantages compared to other ASP monitoring systems. All interviews were digitally recorded and transcribed verbatim. The analysis was conducted using MaxQDA 2020.4 and the Consolidated Framework for Implementation Research (CFIR) constructs. Results: We completed 4 preimplementation interviews and 11 postimplementation interviews with ASP champions and antimicrobial prescribers from 6 medical centers. We derived 4 key themes from the data that map onto CFIR constructs. These themes were interconnected so that implementation of the dashboard (ie, adapting and adopting) was influenced by respondents’ perception of a facility’s size, patient population, and priority placed on stewardship (ie, structural and cultural context), the availability of dedicated stewardship staff and training needed to implement the dashboard (ie, resources needed), and how the dashboard compared to established stewardship activities (ie, relative advantage). ASP champions and antimicrobial prescribers indicated that dashboard metrics were useful for identifying antimicrobial usage and for comparing metrics among similar facilities. Respondents also specified barriers to acceptance of the risk-adjusted metric, such as disagreement regarding how antimicrobials were grouped by the current NHSN protocol, uncertainty of factors involved in risk adjustments, and difficulty developing a clear interpretation of hospital rankings. Conclusions: Given the limited resources for antimicrobial stewardship personnel, automated, risk-adjusted, antimicrobial-use dashboards provided by ASPs are an attractive method to both facilitate compliance and improve efficiency. To increase the uptake of surveillance systems in antimicrobial stewardship, our study highlights the need for clear descriptions of methods and metrics.
Funding: None
Disclosures: None

Automated Nationwide Benchmarking Dashboard for Antimicrobial Stewardship Programs within the Veterans’ Health Administration
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s23-s24
-
- Article
-
- You have access
- Open access
- Export citation
-
Group Name: VHA Center for Antimicrobial Stewardship and Prevention of Antimicrobial Resistance (CASPAR) Background: Antimicrobial stewardship programs (ASPs) are advised to measure antimicrobial consumption as a metric for audit and feedback. However, most ASPs lack the tools necessary for appropriate risk adjustment and standardized data collection, which are critical for peer-program benchmarking. We created a system that automatically extracts antimicrobial use data and patient-level factors for risk-adjustment and a dashboard to present risk-adjusted benchmarking metrics for ASP within the Veterans’ Health Administration (VHA). Methods: We built a system to extract patient-level data for antimicrobial use, procedures, demographics, and comorbidities for acute inpatient and long-term care units at all VHA hospitals utilizing the VHA’s Corporate Data Warehouse (CDW). We built baseline negative binomial regression models to perform risk-adjustments based on patient- and unit-level factors using records dated between October 2016 and September 2018. These models were then leveraged both retrospectively and prospectively to calculate observed-to-expected ratios of antimicrobial use for each hospital and for specific units within each hospital. Data transformation and applications of risk-adjustment models were automatically performed within the CDW database server, followed by monthly scheduled data transfer from the CDW to the Microsoft Power BI server for interactive data visualization. Frontline antimicrobial stewards at 10 VHA hospitals participated in the project as pilot users. Results: Separate baseline risk-adjustment models to predict days of therapy (DOT) for all antibacterial agents were created for acute-care and long-term care units based on 15,941,972 patient days and 3,011,788 DOT between October 2016 and September 2018 at 134 VHA hospitals. Risk adjustment models include month, unit types (eg, intensive care unit [ICU] vs non-ICU for acute care), specialty, age, gender, comorbidities (50 and 30 factors for acute care and long-term care, respectively), and preceding procedures (45 and 24 procedures for acute care and long-term care, respectively). We created additional models for each antimicrobial category based on National Healthcare Safety Network definitions. For each hospital, risk-adjusted benchmarking metrics and a monthly ranking within the VHA system were visualized and presented to end users through the dashboard (an example screenshot in Figure 1). Conclusions: Developing an automated surveillance system for antimicrobial consumption and risk-adjustment benchmarking using an electronic medical record data warehouse is feasible and can potentially provide valuable tools for ASPs, especially at hospitals with no or limited local informatics expertise. Future efforts will evaluate the effectiveness of dashboards in these settings.
Funding: No
Disclosures: None
Figure 1.
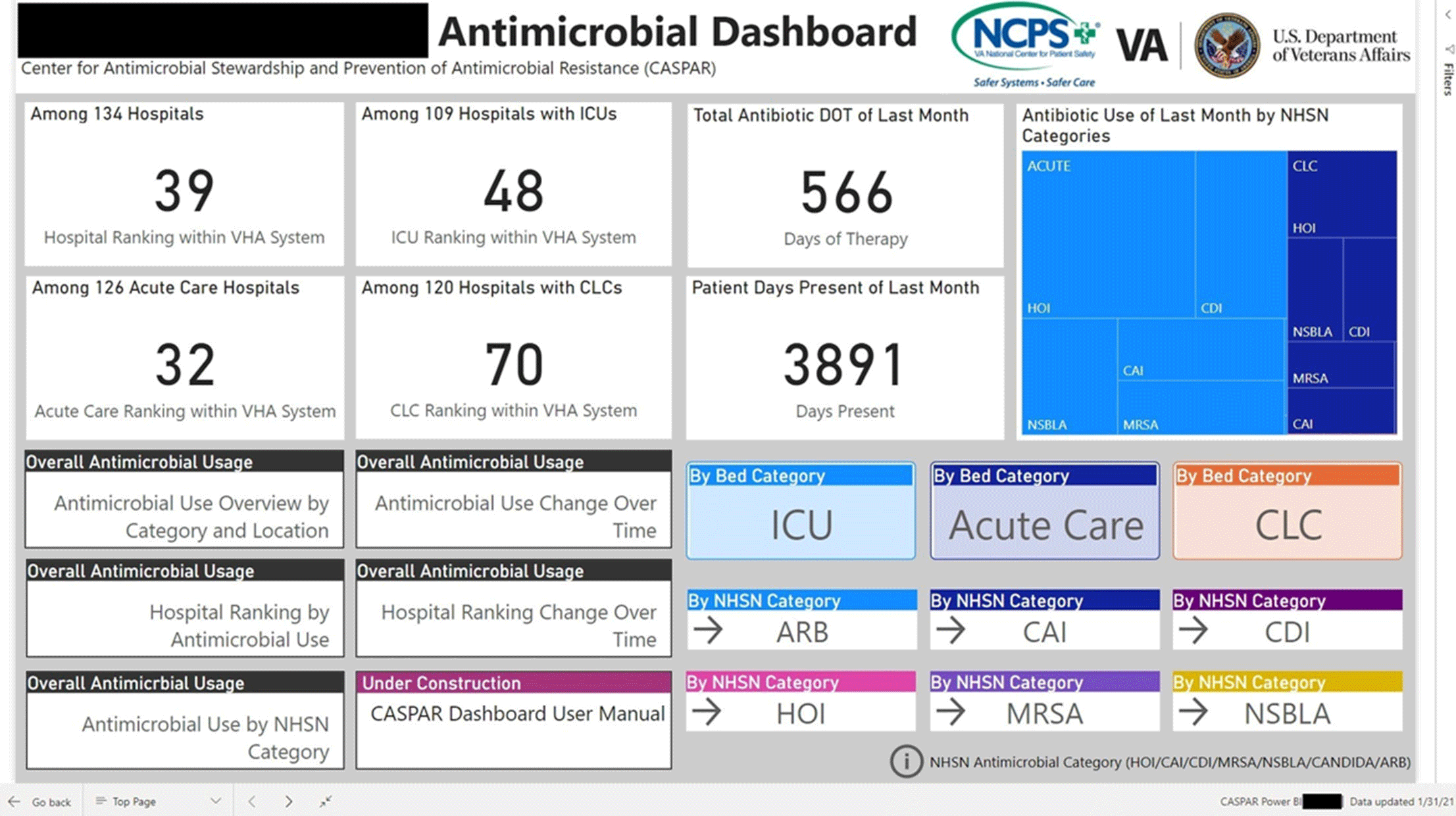
Figure 2.
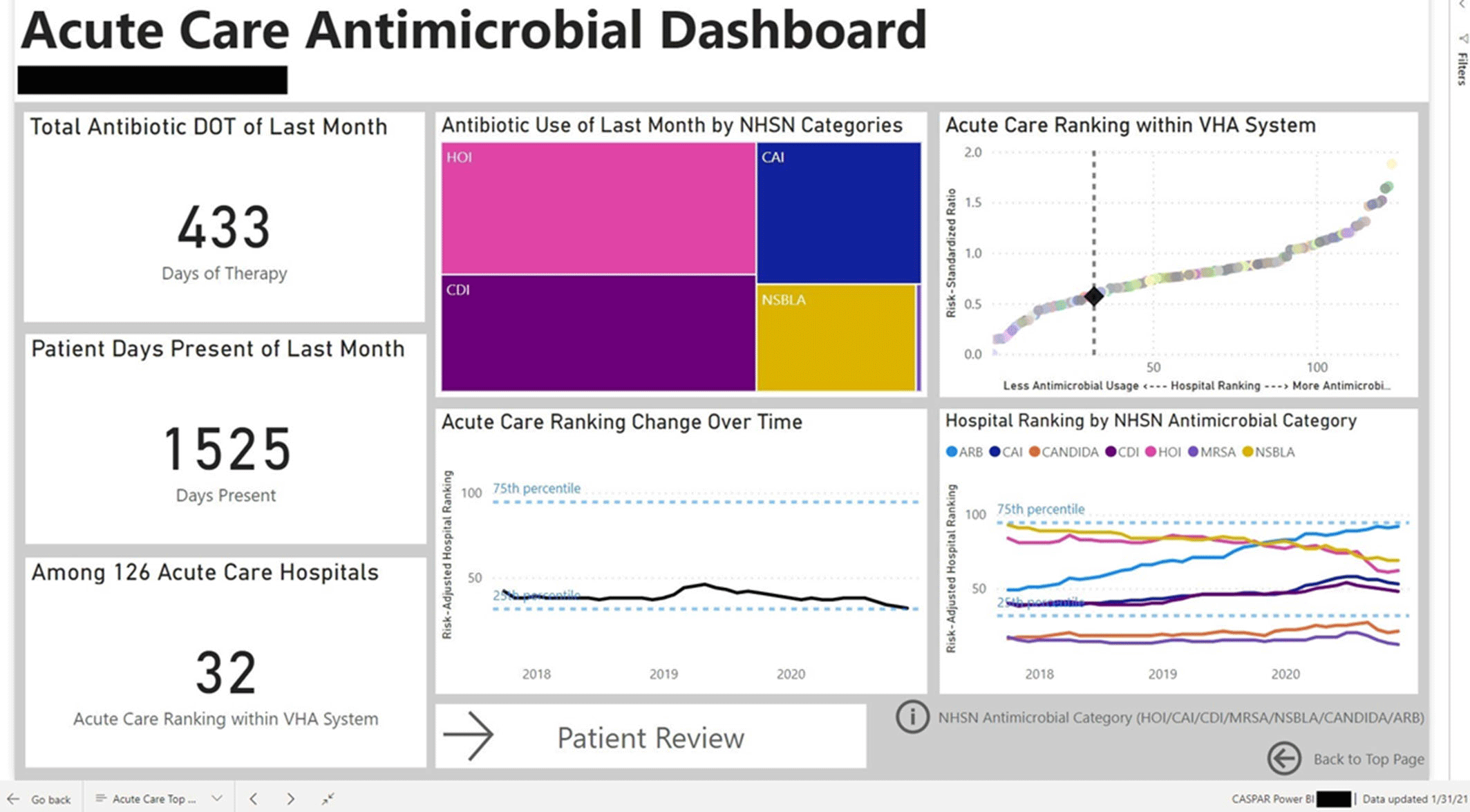
Figure 3.