2 results
Using telehealth to support antimicrobial stewardship at four rural VA medical centers: Interim analysis
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s110
-
- Article
-
- You have access
- Open access
- Export citation
-
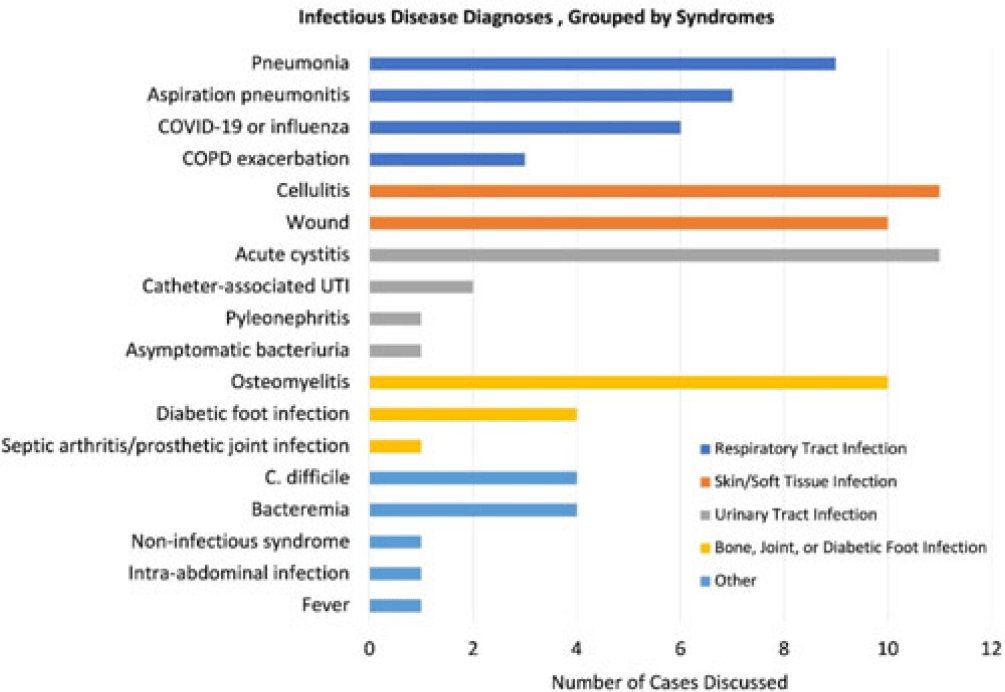
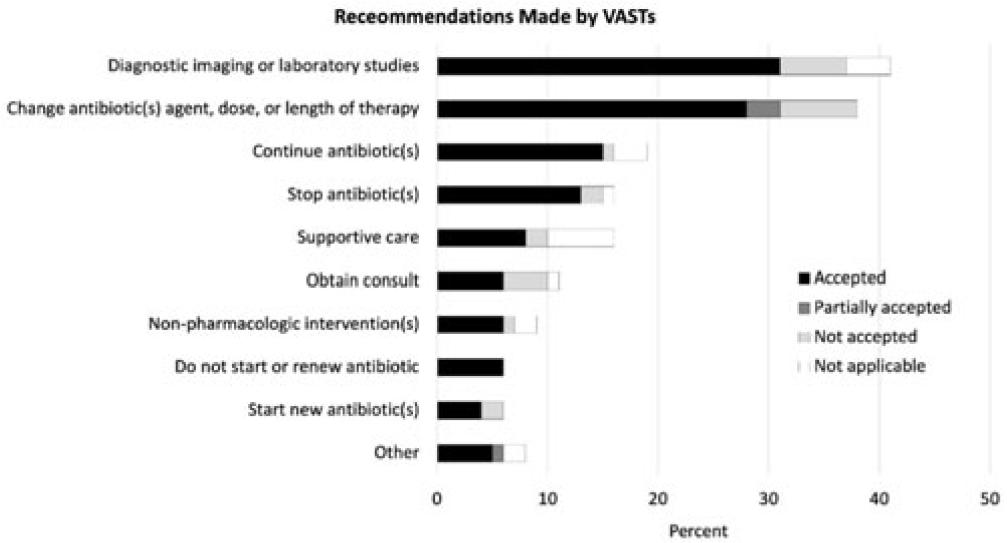
Background: Healthcare settings without access to infectious diseases experts may struggle to implement effective antibiotic stewardship programs. We previously described a successful pilot project using the Veterans Affairs (VA) telehealth system to form a Videoconference Antimicrobial Stewardship Team (VAST) that connected multidisciplinary teams from rural VA medical centers (VAMCs) with infectious diseases experts at geographically distant locations. VASTs discussed patients from the rural VAMC, with the overarching goal of supporting antibiotic stewardship. This project is currently ongoing. Here, we describe preliminary outcomes describing the cases discussed, recommendations made, and acceptance of those recommendations among 4 VASTs. Methods: Cases discussed at any of the 4 participating intervention sites were independently reviewed by study staff, noting the infectious disease diagnoses, recommendations made by infectious diseases experts and, when applicable, acceptance of those recommendations at the rural VAMC within 1 week. Discrepancies between independent reviewers were discussed and, when consensus could not be reached, discrepancies were discussed with an infectious diseases clinician. Results: The VASTs serving 4 different rural VAMCs discussed 96 cases involving 92 patients. Overall, infection of the respiratory tract was the most common syndrome discussed by VASTs (Fig. 1). The most common specific diagnoses among discussed cases were cellulitis (n = 11), acute cystitis (n = 11), wounds (n = 11), and osteomyelitis (n = 10). Of 172 recommendations, 41 (24%) related to diagnostic imaging or laboratory results and 38 (22%) were to change the antibiotic agent, dose, or duration (Fig. 2). Of the 151 recommendations that could be assessed via chart review, 122 (81%) were accepted within 1 week. Conclusions: These findings indicate successful implementation of telehealth to connect clinicians at rural VAMCs with an offsite infectious diseases expert. The cases represented an array of common infectious syndromes. The most frequent recommendations pertained to getting additional diagnostic information and to adjusting, but not stopping, antibiotic therapy. These results suggest that many of the cases discussed warrant antibiotics and that VASTs may use the results of diagnostic studies to tailor that therapy. The high rate of acceptance suggests that the VASTs are affecting patient care. Future work will describe VAST implementation at 4 additional VAMCs, and we will assess whether using telehealth to disseminate infectious diseases expertise to rural VAMCs supports changes in antibiotic use that align with principles of antimicrobial stewardship.
Disclosures: None


Absence of racial and ethnic disparities in COVID-19 survival among residents of US Veterans’ Affairs community living centers
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s35
-
- Article
-
- You have access
- Open access
- Export citation
-
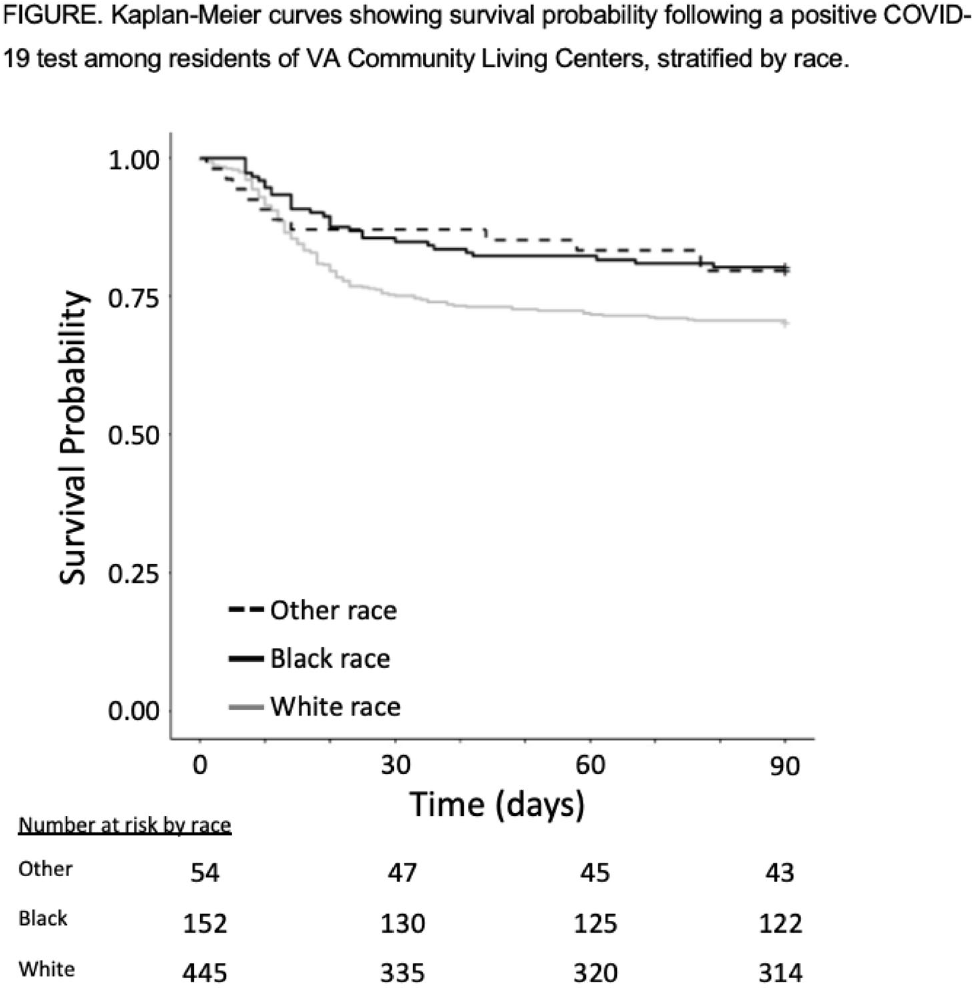
Background: COVID-19 has had a disproportionate effect on nursing homes residents as well as people from racial and ethnic minorities. Whether differences in mortality due to COVID-19 exists for nursing-home residents from racial and ethnic minorities is less clear, with some previous studies reporting systems-level disparities. The Department of Veterans’ Affairs (VA) has nursing homes, termed community living centers (CLCs), across the United States. We hypothesized that differences in COVID-19–related mortality among racial and ethnic minorities would be less pronounced among residents of CLCs. Methods: Using data from the VA Corporate Data Warehouse, we conducted a retrospective cohort study from April 14, 2020 (implementation of population-based testing) to December 10, 2020 (availability of a COVID-19 vaccine). Inclusion criteria were residents with a positive SARS-CoV-2 test while residing in or <48 hours before admission to a CLC. Positive tests <180 days after a prior positive test were excluded. We assessed the cohort for demographics, including self-reported race or ethnicity, clinical characteristics, and survival probability including all-cause 30-day mortality. A multivariable logistic regression model was used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for all-cause 30-day mortality that included race, ethnicity, age, and Charlson comorbidity index (CCI). Results: Among 14,759 CLC residents, 651 (4.4%) had a positive SARS-COV-2 test. Their mean age was 75.7 ± 11.3 years, and self-reported race or ethnicity was 68% White (445 of 651), 23% Black (152 of 651), and 4% Hispanic/Latinx (27 of 651). The mean CCI was lower among White residents than Black residents (4.15 ± 2.6 vs 4.61 ± 3.1, respectively). All-cause 30-day mortality for CLC residents following positive SARS-COV-2 test was 25% for White patients, 14% for Black patients, and 15% for Hispanic/Latinx patients (Fig. 1). Age (in years), but neither race or ethnicity nor CCI, was independently associated with all-cause 30-day mortality (OR, 1.07; 95% CI, 1.05–1.09) in CLC residents with COVID-19. Conclusions: Among VA CLC residents with a positive COVID-19 test, minority CLC residents did not have worse outcomes than white residents, suggesting that users of the VA healthcare system may enjoy abrogation of some aspects of health disparities.
Funding: None
Disclosures: None