
3 results
Alarming prevalence of Candida auris among critically ill patients in intensive care units in Dhaka City, Bangladesh
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s11
-
- Article
-
- You have access
- Open access
- Export citation
-
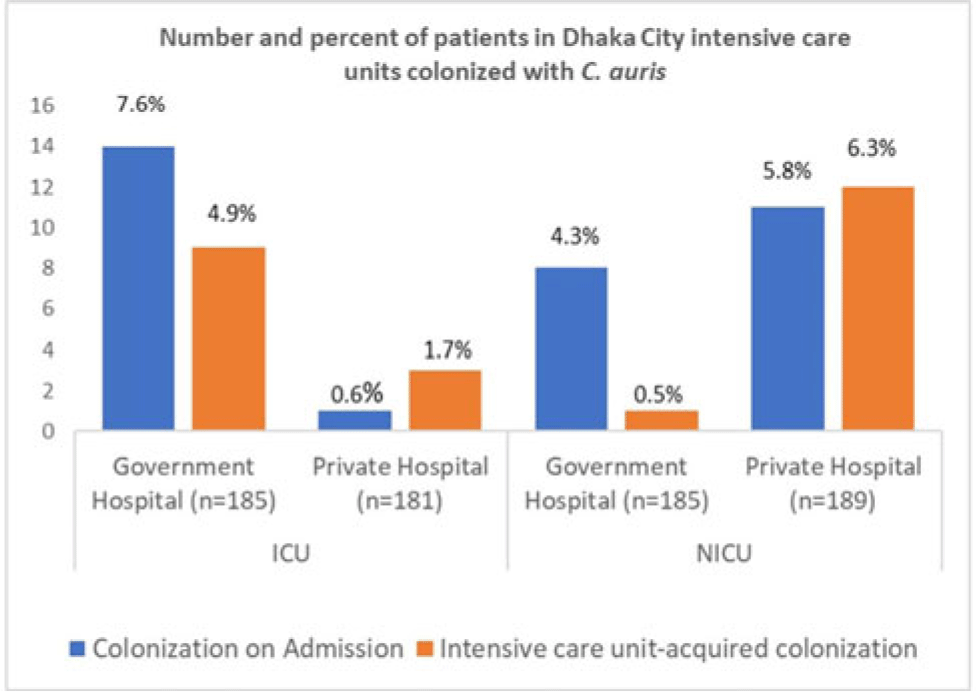
Background: Candida auris is a multidrug-resistant yeast capable of invasive infection with high mortality and healthcare-associated outbreaks globally. Due to limited labratory capacity, the burden of C. auris is unknown in Bangladesh. We estimated the extent of C. auris colonization and infection among patients in Dhaka city intensive care units. Methods: During August 2021–September 2022 at adult intensive care units (ICUs) and neonatal intensive care units (NICUs) of 1 government and 1 private tertiary-care hospital, we collected skin swabs from all patients and blood samples from sepsis patients on admission, mid-way through, and at the end of ICU or NICU stays. Skin swab and blood with growth in blood-culture bottle were inoculated in CHROMagar, and identification of isolates was confirmed by VITEK-2. Patient characteristics and healthcare history were collected. We performed descriptive analyses, stratifying by specimen and ICU type. Results: Of 740 patients enrolled, 59 (8%) were colonized with C. auris, of whom 2 (0.3%) later developed a bloodstream infection (BSI). Among patients colonized with C. auris, 27 (46%) were identified in the ICU and 32 (54%) were identified from the NICU. The median age was 55 years for C. auris–positive ICU patients and 4 days for those in the NICU. Also, 60% of all C. auris patients were male. Among 366 ICU patients, 15 (4%) were positive on admission and 12 (3%) became colonized during their ICU stay. Among 374 NICU patients, 19 (5%) were colonized on admission and 13 (4%) became colonized during their NICU stay. All units identified C. auris patients on admission and those who acquired it during their ICU or NICU stay, but some differences were observed among hospitals and ICUs (Figure). Among patients colonized on admission to the ICU, 11 (73%) were admitted from another ward, 3 (20%) were admitted from another hospital, and 1 (7%) were admitted from home. Of patients colonized on admission to the NICU, 4 (21%) were admitted from the obstetric ward, 9 (47%) were admitted from another hospital, and 6 (32%) were admitted from home. In addition, 18 patients with C. auris died (12 in the ICU and 6 in the NICU); both patients with C. auris BSIs died. Conclusions: In these Bangladesh hospitals, 8% of ICU or NICU patients were positive for C. auris, including on admission and acquired during their ICU or NICU stay. This high C. auris prevalence emphasizes the need to enhance case detection and strengthen infection prevention and control. Factors contributing to C. auris colonization should be investigated to inform and strengthen prevention and control strategies.
Disclosure: None

Antibiotic use among SARI patients according to the AWaRe classification before and during the COVID-19 pandemic in Bangladesh
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s28
-
- Article
-
- You have access
- Open access
- Export citation
-
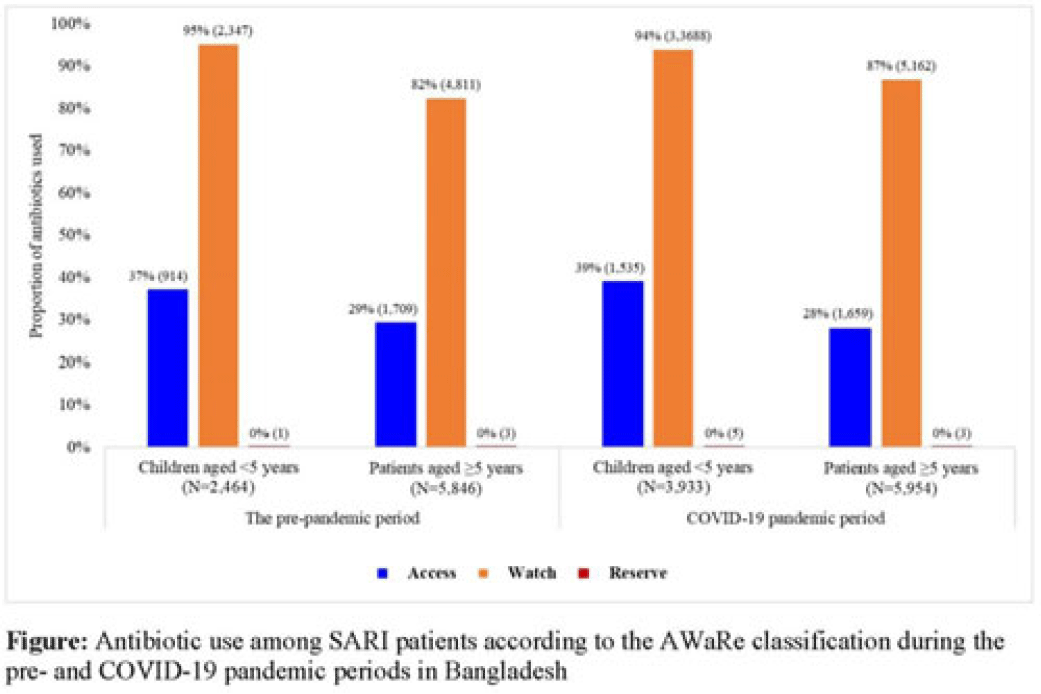
Background: Irrational antibiotic use among hospitalized patients can lead to antibiotic resistance. For rational use, the WHO introduced the Access, Watch, and Reserve (AWaRe) classification of antibiotics. We explored antibiotic use according to the AWaRe classification among patients hospitalized with severe acute respiratory infection (SARI) between the prepandemic and COVID-19 pandemic periods in Bangladesh. Methods: From June 2017 to November 2022, we analyzed SARI inpatient data from the hospital-based influenza surveillance platform at 9 tertiary-level hospitals in Bangladesh. We defined June 2017–February 2020 as the prepandemic period and March 2020–November 2022 as the pandemic period. Physicians identified inpatients meeting the WHO SARI case definition and recorded patient demographics, clinical characteristics, and antibiotics received during hospitalization. We used descriptive statistics to summarize the data. Results: We enrolled 20,640 SARI patients (median age, 20 years; IQR, 1.6–50; 63% male); and among them, 18,197 (88%) received antibiotics (26% of those received >1 different course of antibiotics). Compared to the prepandemic period, the proportion of antibiotic use among SARI patients was higher during the pandemic: 93% (9,887 of 10,655) versus 83% (8,310 of 9,985) (P < .001). According to AWaRe classification, Access, Watch, and Reserve groups accounted for 32% (n = 2,623), 86% (n = 7,158), and 0.05% (n = 4), respectively, before the pandemic and 32% (n = 3,194), 90% (n = 8,850), and 0.08% (n = 8), respectively, during the pandemic (Fig.). The most common antibiotic prescribed for children aged <5 years during the prepandemic was ceftriaxone (n = 1,940, 74%), followed by amikacin (n = 325, 13%) and flucloxacillin (n = 300, 12%); similarly, during the pandemic, most common antibiotic prescribed was ceftriaxone (n = 3,097, 79%), followed by amikacin (n = 723, 18%) and flucloxacillin (n = 348, 9%). The most common antibiotic prescribed for patients aged ≥5 years during the prepandemic period was ceftriaxone (n = 3,174, 54%), followed by amoxicillin-clavulanic acid (n = 1,304, 22%) and azithromycin (n = 1,038, 18%). During the pandemic, the most common antibiotic prescribed for patients aged ≥5 years was ceftriaxone (n = 3,793, 64%), followed by amoxicillin-clavulanic acid (n = 1,327, 22%) and clarithromycin (n = 797, 13%). Among children aged <5 years, use of the Watch group of antibiotics during the prepandemic and pandemic periods was similar: 94% (n = 3,688) versus 95% (n = 2,347) (P = .099). However, among patients aged ≥5 years, the use of Watch antibiotics was higher during the pandemic compared to the prepandemic period: 87% (n = 5,163) versus 82% (n = 4,811) (P < .001). Conclusions: Use of antibiotics in the Watch group was predominant among SARI patients both before and during the COVID-19 pandemic, and it increased among SARI patients aged ≥5 years during the pandemic period in Bangladesh. Promoting antibiotic stewardship programs for physicians, including in-service training on antibiotic use, could reduce irrational antibiotic use, which might contribute to mitigating antibiotic resistance in the country.
Financial support: This study was funded by the CDC.
Disclosures: None

Working with Respiratory Illness: Presenteeism Among Healthcare Personnel at Tertiary-Care Hospitals in Bangladesh, 2008–2016
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s76
-
- Article
-
- You have access
- Open access
- Export citation
