2 results
Outbreak of Pseudomonas aeruginosa Bacteremia Infections among Stem-Cell Transplant Patients Related to Change in Prophylaxis
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s25-s26
-
- Article
-
- You have access
- Open access
- Export citation
-
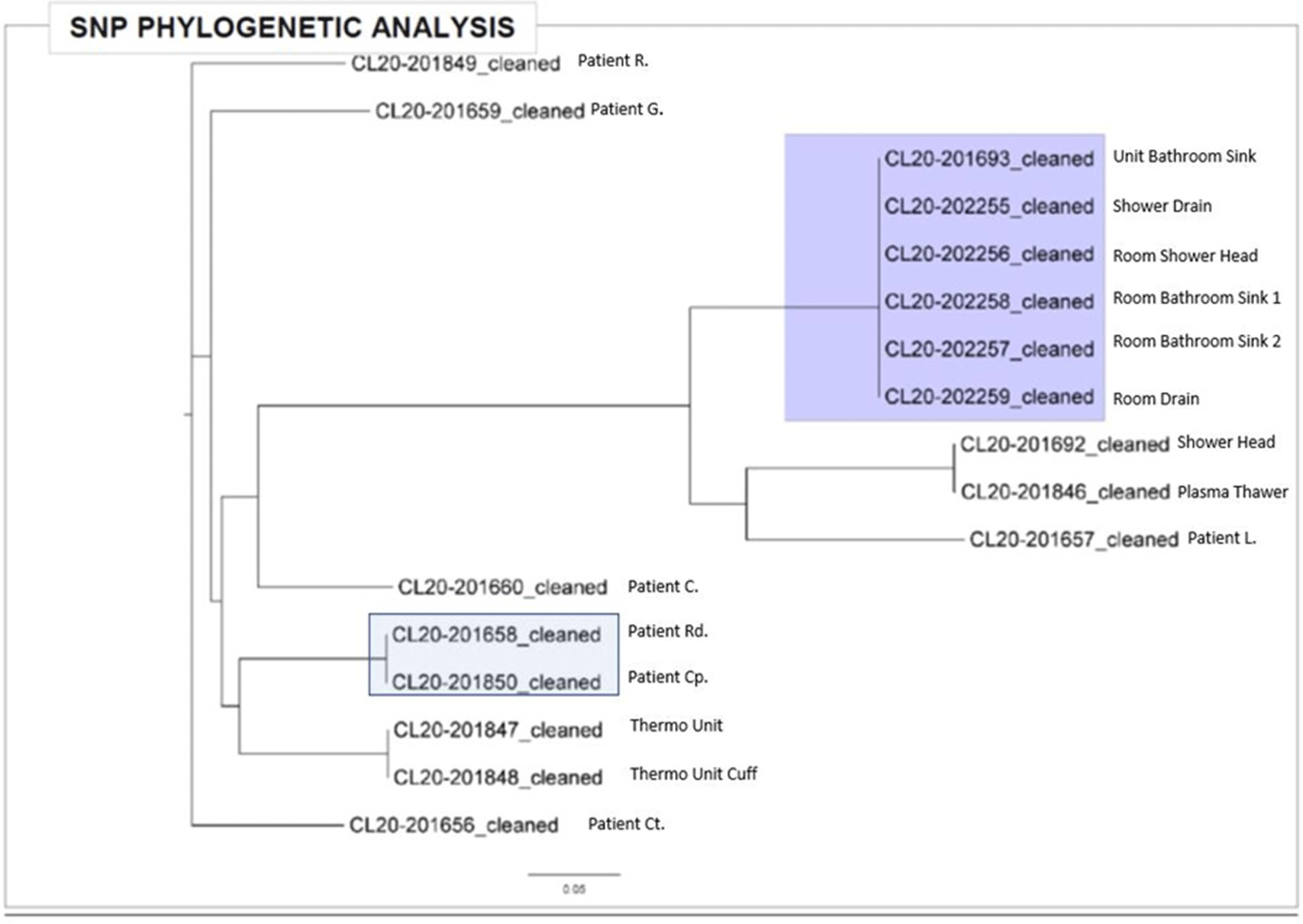
Background:Pseudomonas aeruginosa outbreaks can originate from various sources and can cause severe complications in posttransplant patients. Antibiotic prophylaxis can decrease posttransplant infections; however, consideration must be given to P. aeruginosa coverage as we outline an outbreak among the stem-cell transplant (SCT) population. Methods: A multidisciplinary outbreak investigation was conducted to evaluate sources of contamination and changes in clinical processes. Positive blood cultures from SCT patients and environmental isolates were analyzed using whole-genome sequencing (WGS). Incidence density rates for P. aeruginosa blood cultures from January 2019 through October 2020 were calculated per 10,000 patient days and stratified by unit, specimen, and transplant type. Statistical analysis was calculated with significance at p < 0.05. Results: A cluster of 8 SCT patients was identified between May and September 2020. Moreover, 10 environmental samples were positive for P. aeruginosa including drains, water sources prior to the point-of-use (POU) filter and blood-bank thaw machines. Phylogenetic analysis revealed 1 cluster of 2 patients who shared the same room, 5 patients with unique P. aeruginosa isolates, and 2 separate clusters of environmental isolates with relatedness only to each other. Review of clinical processes showed a change from fluoroquinolone prophylaxis to cephalosporin in the spring of 2020. Also, 5 P. aeruginosa bacteremia infections occurred prior to June (11.78 cases per 10,000 patient days). During the period of cephalosporin use, 8 infections were identified (58.27 cases per 10,000 patient days) (P = .006). Following the restart of fluoroquinolone, zero infections have occurred to date, as of January 28, 2021. Conclusions: Discontinuation of fluoroquinolone prophylaxis was associated with P. aeruginosa bacteremia infections in SCT patients. Use of fluoroquinolone prophylaxis in SCT patients is protective from P. aeruginosa bacteremia infections. There have been no further infections in the following 3 months after the change back to the use of fluoroquinolone. Additionally, WGS showed that most patient isolates did not have a common source, suggesting that P. aeruginosa gastrointestinal colonization may play a role in seeding these bacteremia infections.
Funding: No
Disclosures: None
Figure 1.
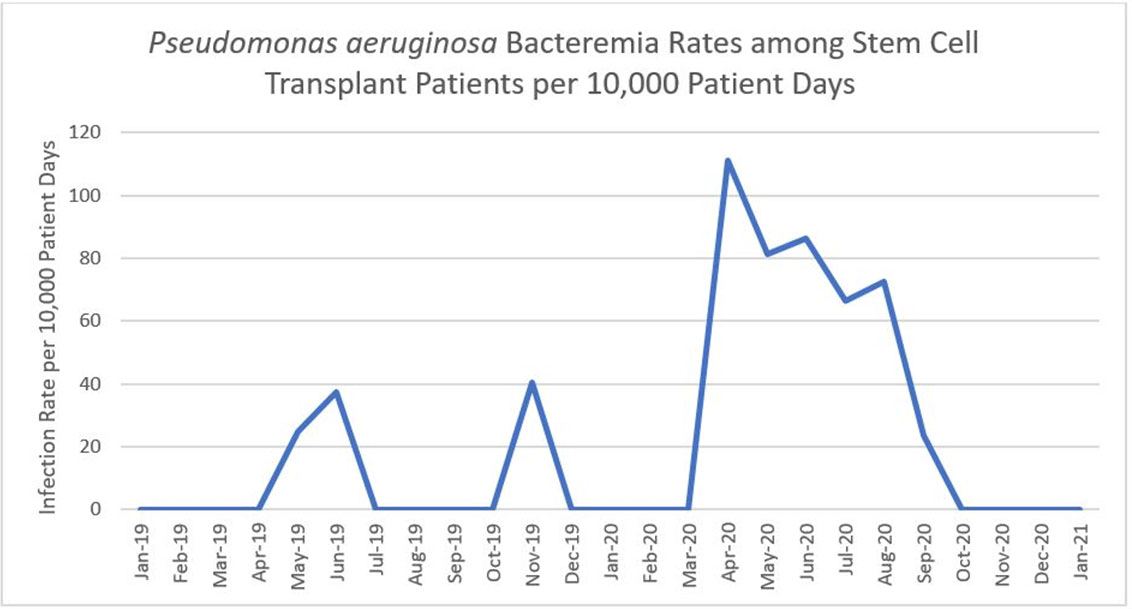
Figure 2.


A Cluster of Aspergillosis Associated with SARS-CoV-2
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s10
-
- Article
-
- You have access
- Open access
- Export citation
-
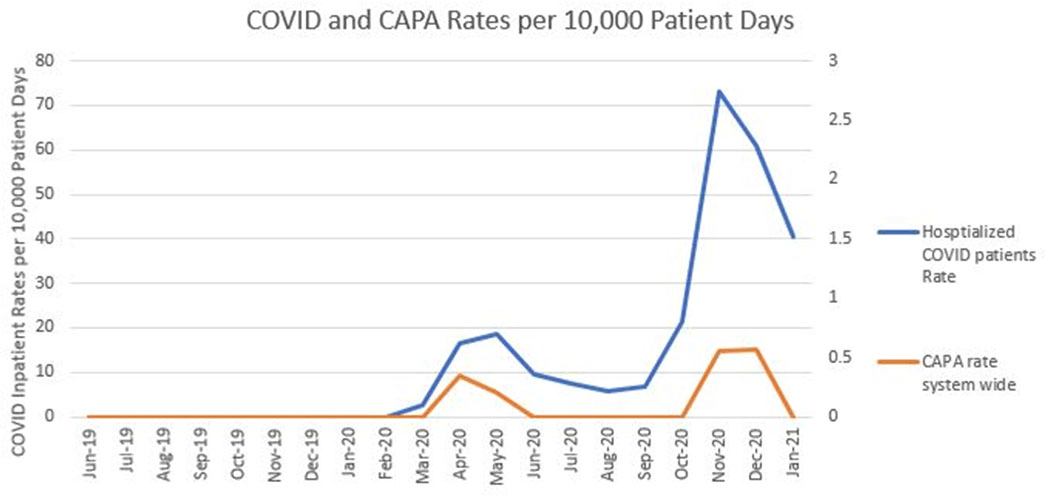
Background: Coronavirus disease 2019 (COVID-19) has demonstrated a variety of presentations and clinical complications, among them coinfection of pneumonia with the mold Aspergillus spp. Patients at risk for invasive disease include transplant recipients and those with prolonged neutropenia, immune disorders, cystic fibrosis, and steroid use. There have been recent descriptions of coronavirus disease–associated pulmonary aspergillosis (CAPA). An outbreak investigation into a cluster of Aspergillus fumigatus infections in a health system intensive care unit uncovered a community-onset (CO) increase in CAPA. Methods: A multidisciplinary outbreak investigation was conducted evaluating sources of contamination, completion of construction projects, and changes in clinical processes. Retrospective chart review was done for the prior 18 months and incidence density rates for Aspergillus infections from June 2019 through December 2020 were calculated per 10,000 patient days, stratified by unit, specimen source, and coinfection with COVID-19. Data were linked with all positive and negative COVID-19 tests performed by the health system’s regional laboratory from March to December 2020. Healthcare-onset (HO) classification was based on infections identified ≥7 days after admission. Statistical analysis was calculated with significance at p < 0.05. Results: Over the last 18 months, 82 patients were identified positive with Aspergillus cultures; of which 10 (12%) met CAPA definitions. Aspergillus fumigatus was the most common species and accounted for 62% of samples, followed by Aspergillus niger (17%). Median rates of HO Aspergillosis were 0.45 cases per 10,000 patient days, whereas the median total rates of infection were 1.97 cases per 10,000 patient days. Rates of CAPA coincided with COVID-19 hospitalization rates. In the spring and fall, surges of COVID-19, the rate ratio of CAPA to COVID hospitalized infections per 10,000 patient days, ranged from 0.006 to 0.015. Once CAPA infections were adjusted for, rates of CO Aspergillus remained high, whereas HO cases suggested baseline acquisition. Conclusion: This study outlines rates of CO aspergillosis as well as CAPA rates coinciding with the healthcare system’s spring and fall surges of COVID-19 hospitalizations. Despite the determination that this was not a hospital-acquired cluster, the investigation revealed some areas for opportunity in construction processes along with maintaining coverage of all patient supplies to reduce the risk of contamination.
Funding: No
Disclosures: None
Figure 1.