
20 results
Length of antibiotic therapy among adults hospitalized with uncomplicated community-acquired pneumonia, 2013–2020
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 45 / Issue 6 / June 2024
- Published online by Cambridge University Press:
- 14 February 2024, pp. 726-732
- Print publication:
- June 2024
-
- Article
- Export citation
Uncovering gut microbiota-mediated indirect effects of antibiotic use on Clostridioides difficile transmission
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s104-s105
-
- Article
-
- You have access
- Open access
- Export citation
-
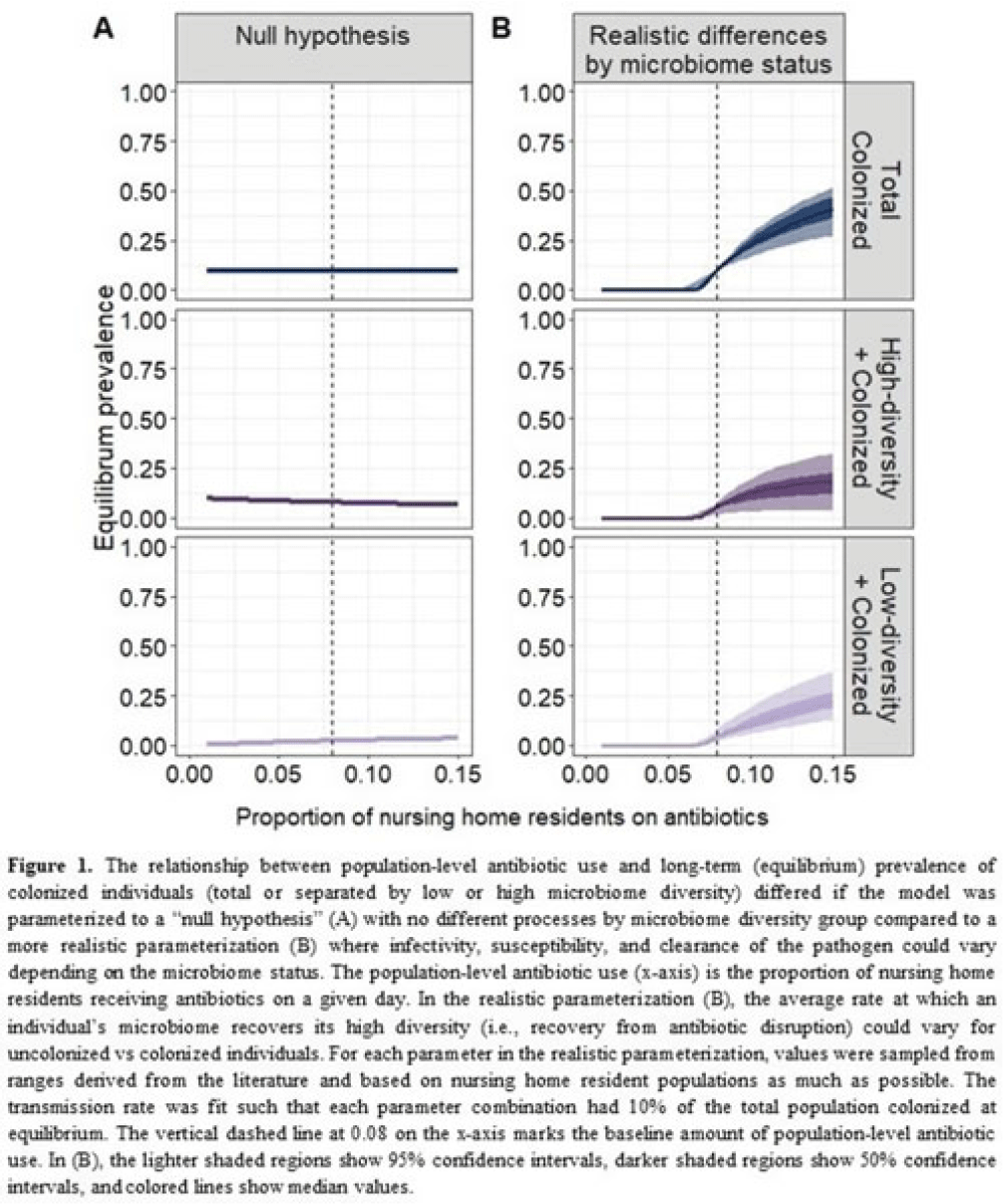
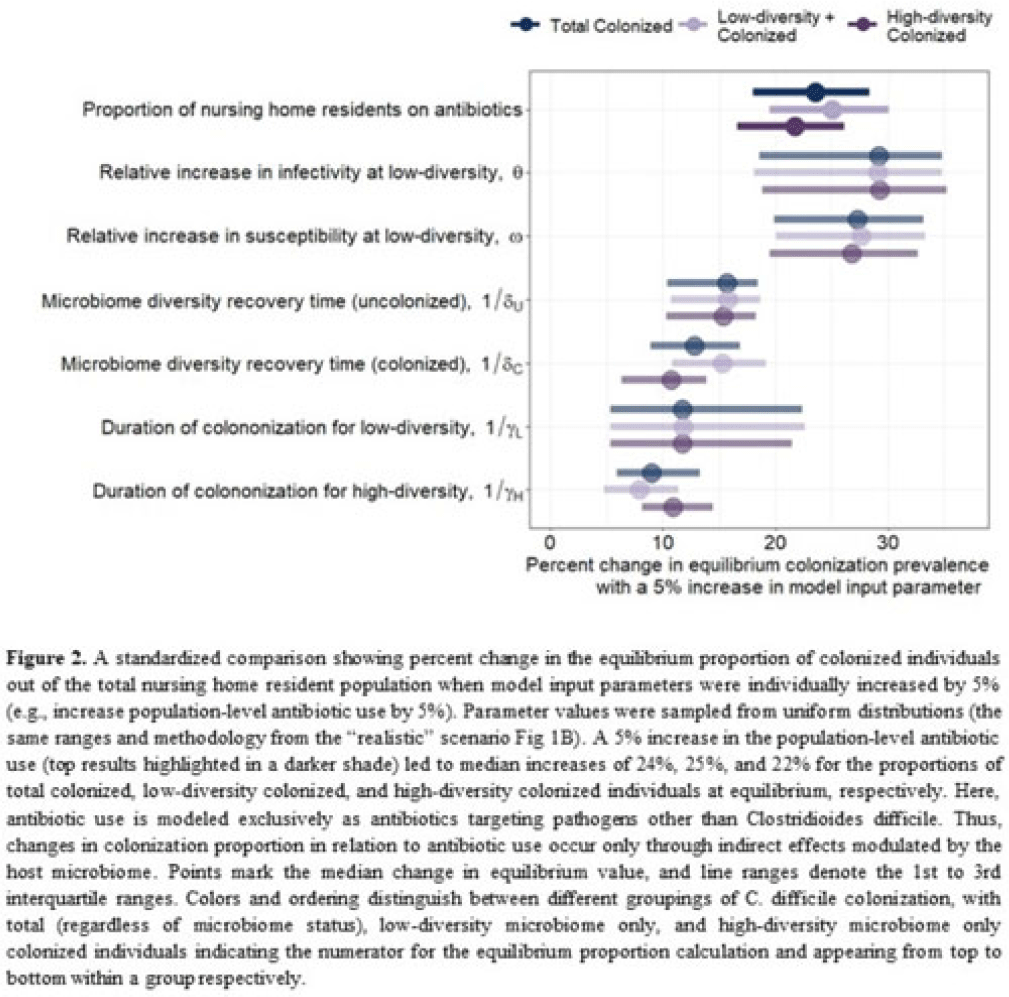
Background: Clostridioides difficile and multidrug-resistant organisms (MDROs) pose challenges due to treatment complexities and substantial morbidity and mortality. Susceptibility to colonization with these organisms and potential onward transmission if colonized (ie, infectivity) is influenced by the human microbiome and its dynamics. Disruptive effects of antibiotics on the microbiome imply potential indirect effects of antibiotics on C. difficile colonization. Mathematical models can help explore the relative impact of key pathways linking antibiotic use to C. difficile colonization, including the relationship between population-level antibiotic use and colonization prevalence. Methods: We built a compartmental model of long-term C. difficile colonization prevalence of nursing home residents (though malleable for any MDRO), allowing interactions between the microbiome and the colonization process. Based on proportional abundance of microbial taxa, we classified individuals into high and low α diversity groups, each further stratified into uncolonized or colonized with C. difficile. The rate of transition from the high to low microbiome diversity group was proportional to the population-level rate of antibiotic use. Transmission dynamics followed a susceptible–infectious–susceptible framework with the possibility for increased susceptibility and infectivity for the low-diversity microbiome group. First, as a comparator, we used a “null model” in which microbiome diversity did not influence host susceptibility or infectivity. Next, we sampled from realistic (literature informed) parameter ranges to analyze how the microbiome mediates the effect of antibiotics on colonization in this population. Results: Our analysis suggests that antibiotic use can catalyze colonization with C. difficile through interactions with the host microbiome, resulting in a sharp increase in colonization with a modest increase in antibiotic use (Fig 1). Increasing the population-level antibiotic use by 5% led to a median 24% increase in long-term colonization prevalence in the model (Fig 2). In contrast, increasing susceptibility or infectivity rates by 5% resulted in slightly higher increases in total colonization (27% and 29%, respectively). However, there was considerable uncertainty around these estimates, with interquartile ranges of up to 20% for some parameters (Fig 2). Conclusions: Higher population-level antibiotic use likely increases colonization by C. difficile through indirect effects of the microbiome. The increased colonization burden attributable to increasing antibiotic use may be substantial. With high uncertainty around some estimates, conducting observational studies to better understand key colonization and microbiome parameters (eg, the relative increase in susceptibility or infectivity with lower microbiome diversity) is critical for future efforts to estimate the impact of antibiotic use on colonization with C. difficile and MDROs.
Disclosures: None


Fluconazole resistance in non-albicans Candida species in the United States, 2012-2021
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s29-s30
-
- Article
-
- You have access
- Open access
- Export citation
-
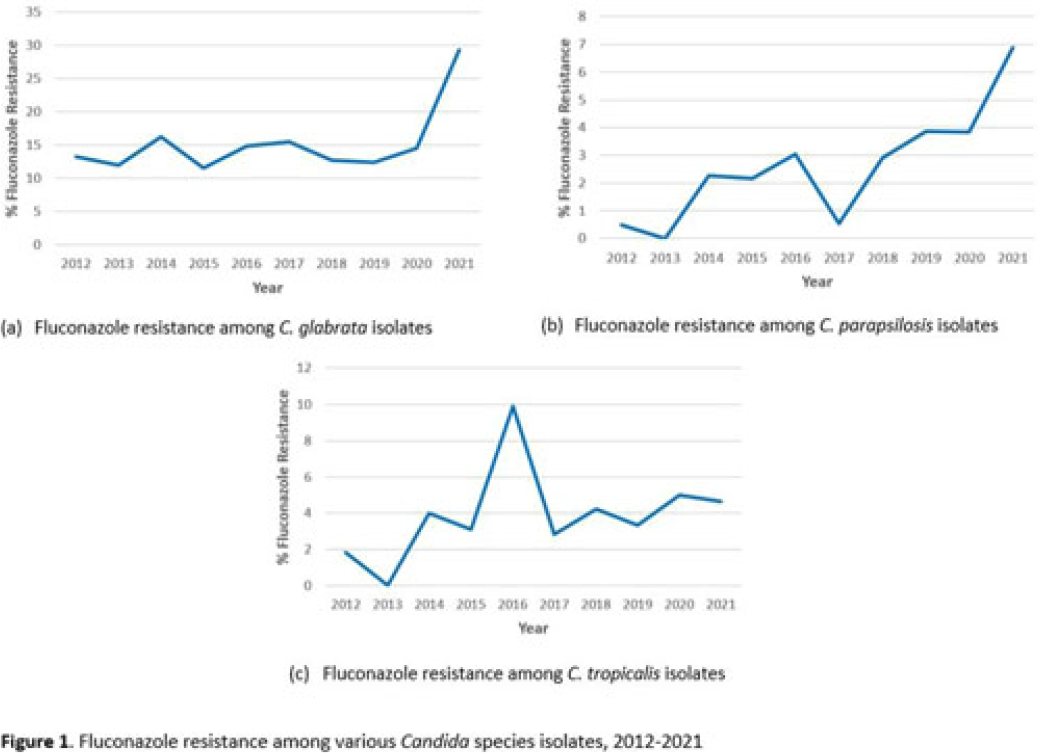
Background: Candida spp can cause a variety of infections known as candidiasis, ranging from severe invasive infections to superficial mucosal infections of the mouth and vagina. Fluconazole, a triazole antifungal, is commonly prescribed to treat candidiasis but increasing fluconazole resistance is a growing concern for several Candida spp. Although C. albicans has historically been the most common cause of candidiasis, other species are increasingly common and antifungal resistance is more prevalent in these non-albicans species, including C. glabrata, C. parapsilosis, and C. tropicalis, which were the focus of this analysis. Methods: We used the PINC AI healthcare data (PHD) database to examine fluconazole resistance for inpatient isolates between 2012 and 2021 from 187 US acute-care hospitals with at least 1 Candida spp culture with a fluconazole susceptibility result over the entire period. We calculated annual percentage fluconazole resistance for C. glabrata, C. tropicalis, and C. parapsilosis isolates using the clinical laboratory interpretation for resistance. Results: We identified 4,264 C. glabrata, 2,482 C. parapsilosis, and 2,283 C. tropicalis isolates between 2012 and 2021 with susceptibility results. The percentage of C. glabrata isolates resistant to fluconazole doubled between 2020 and 2021 (14.6% vs 29.3%) (Fig. 1a). The percentage of C. parapsilosis isolates resistant to fluconazole steadily increased since 2017 (Fig. 1b), with an 82% increase in 2021 compared with 2020 (3.8% in 2020 vs 6.9% in 2021). Fluconazole resistance among C. tropicalis isolates varied over the years, with a 0.3% decrease in 2021 from 2020 (Fig. 1c). Of hospitals reporting at least 1 result each year 2020–2021, 44% observed an increase in the proportion of C. glabrata isolates resistant to fluconazole in 2021 compared to 2020. Conclusions: Our analysis highlights a concerning increase in fluconazole resistance among C. glabrata and C. parapsilosis isolates in 2021 compared with previous years. Further investigation of the observed increases in fluconazole resistance among these Candida spp could provide further insight on potential drivers of resistance or limitations in reported results from large databases. More analyses are needed to understand rates, sites of Candida infections, and risk factors (eg, antifungal exposure) associated with resistance.
Disclosures: None

Decolonization of hospital patients may aid efforts to reduce transmission of carbapenem-resistant Enterobacterales
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s59-s60
-
- Article
-
- You have access
- Open access
- Export citation
-
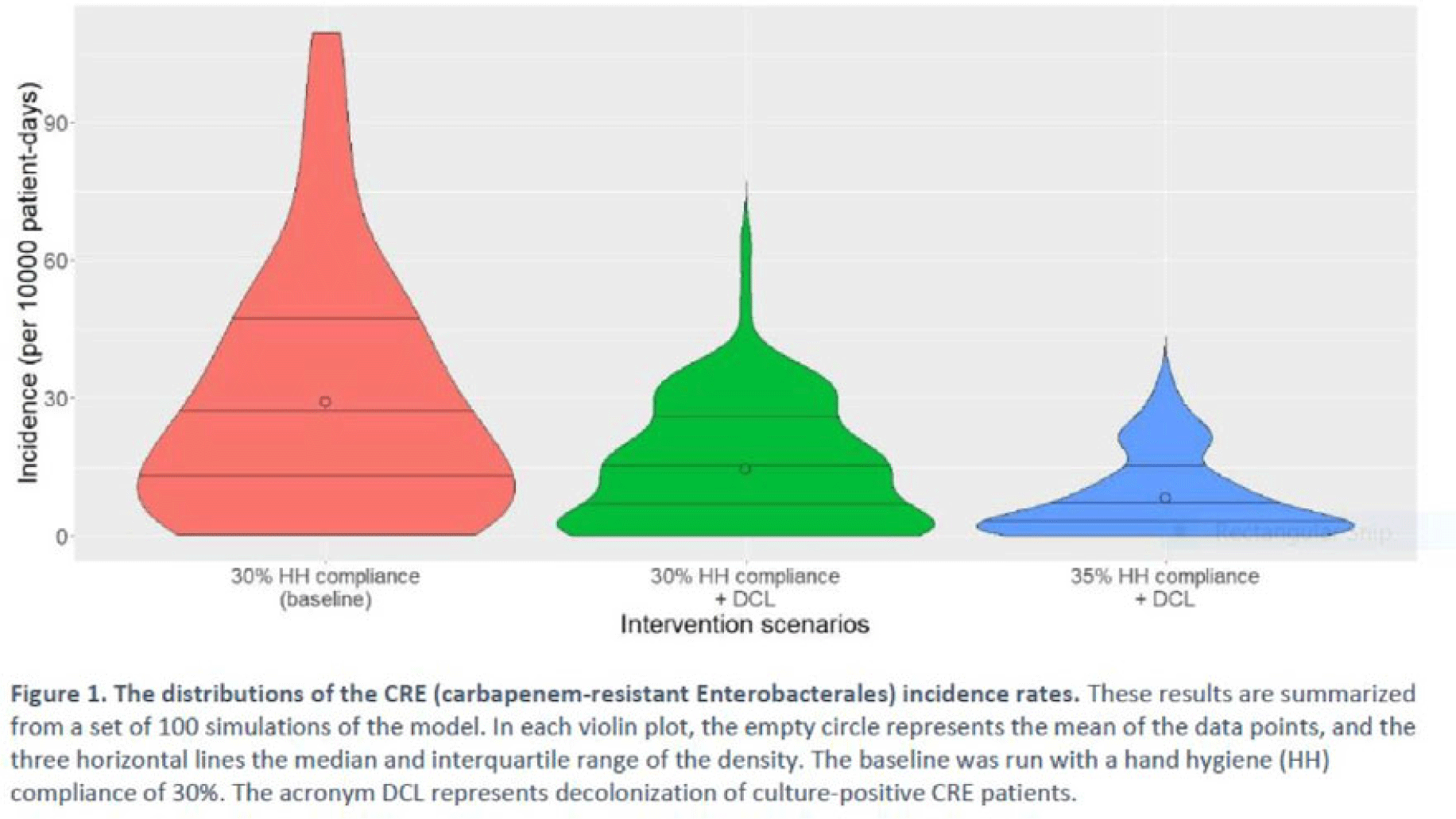
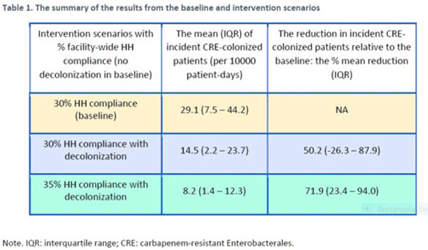
Background: Multimodal approaches are often used to prevent transmission of antimicrobial-resistant pathogens among patients in healthcare settings; understanding the effect of individual interventions is challenging. We designed a model to compare the effectiveness of hand hygiene (HH) with or without decolonization in reducing patient colonization with carbapenem-resistant Enterobacterales (CRE). Methods: We developed an agent-based model to represent transmission of CRE in an acute-care hospital comprising 3 general wards and 2 ICUs, each with 20 single-occupancy rooms, located in a community of 85,000 people. The model accounted for the movement of healthcare personnel (HCP), including their visits to patients. CRE dynamics were modeled using a susceptible–infectious–susceptible framework with transmission occurring via HCP–patient contacts. The mean time to clearance of CRE colonization without intervention was 387 days (Zimmerman et al, 2013). Our baseline included a facility-level HH compliance of 30%, with an assumed efficacy of 50%. Contact precautions were employed for patients with CRE-positive cultures with assumed adherence and efficacy of 80% and 50%, respectively. Intervention scenarios included decolonization of culture-positive CRE patients, with a mean time to decolonization of 3 days. We considered 2 hypothetical intervention scenarios: (A) decolonization of patients with the baseline HH compliance and (B) decolonization with a slightly improved HH compliance of 35%. The hospital-level CRE incidence rate was used to compare the results from these intervention scenarios. Results: CRE incidence rates were lower in intervention scenarios than the baseline scenario (Fig. 1). The baseline mean incidence rate was 29.1 per 10,000 patient days. For decolonization with the baseline HH, the mean incidence rate decreased to 14.5 per 10,000 patient days, which is a 50.2% decrease relative to the baseline incidence (Table 1). The decolonization scenario with a slightly improved HH compliance of 35% produced a relative reduction of 71.9% relative to the baseline incidence. Conclusions: Our analysis shows that decolonization, combined with modest improvement in HH compliance, could lead to large decreases in pathogen transmission. In turn, this model implies that efforts to identify and improve decolonization strategies for better patient safety in health care may be needed and are worth exploring.
Disclosures: None


Empiric antibiotic selection for community-acquired pneumonia in US hospitals, 2013–2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s26-s27
-
- Article
-
- You have access
- Open access
- Export citation
-
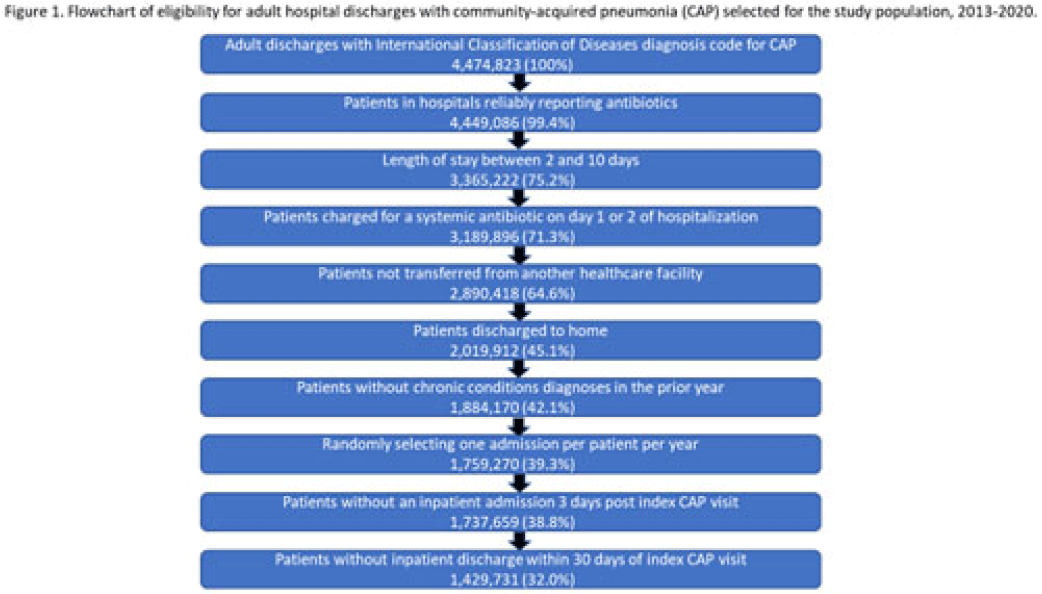
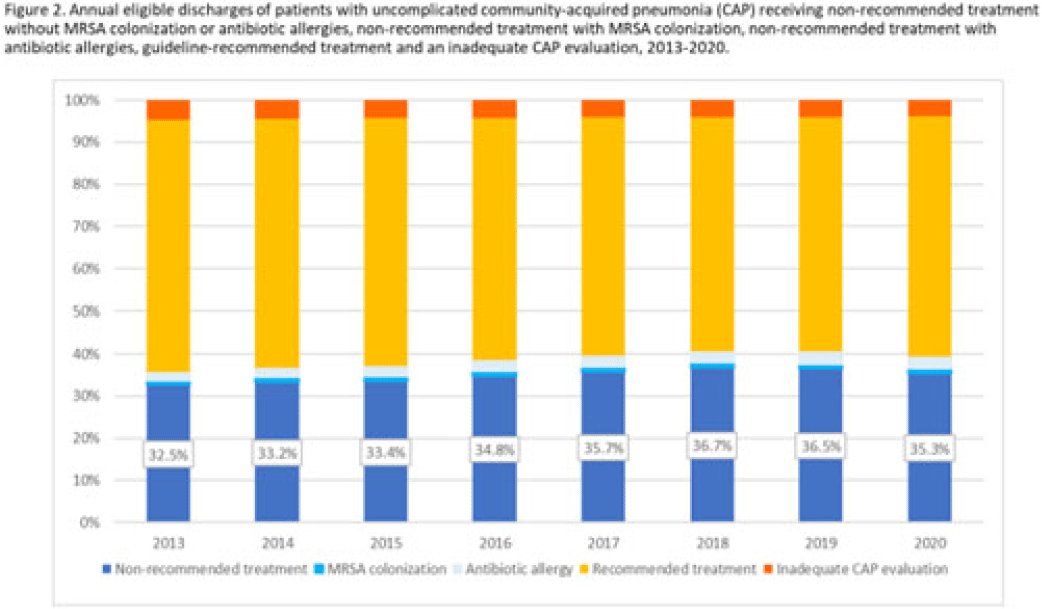
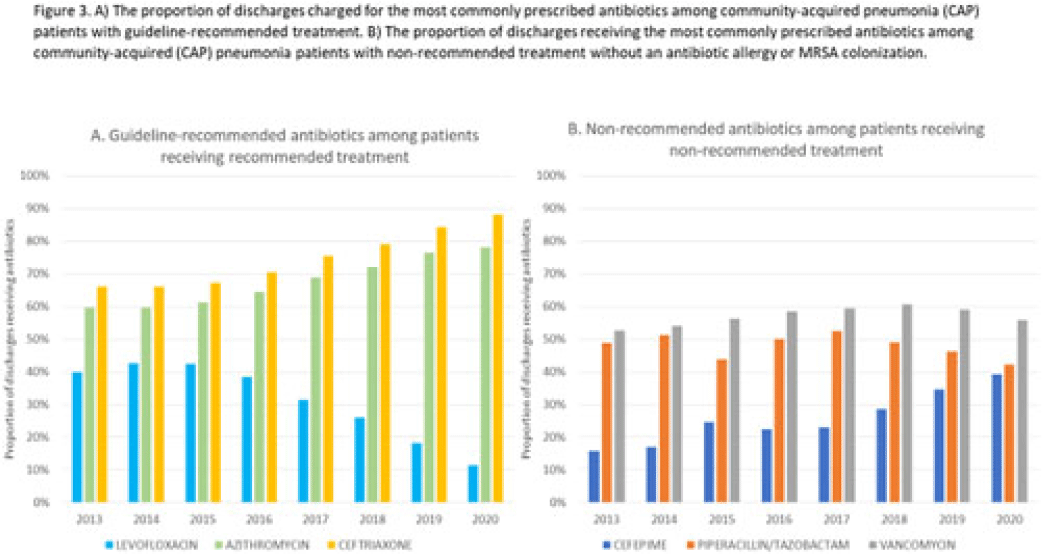
Background: Community-acquired pneumonia (CAP) is a common indication for antibiotic prescribing in hospitalized patients. Professional societies’ clinical guidelines recommend specific antibiotics for empiric treatment of CAP based on clinical factors. Manual assessments of appropriateness are time-consuming and are often conducted on a smaller scale. We evaluated empiric antibiotic selection among a large cohort of adults hospitalized with CAP using electronic health records. Methods: In this study, we used the PINC-AI healthcare database to define a cohort of adults hospitalized with CAP from 2013 to 2020. CAP was identified by International Classification of Diseases (ICD) diagnosis codes. Exclusions were applied to identify uncomplicated CAP (Fig. 1). Treatment was only evaluated if a chest radiograph or computerized tomography (CT) scan was charged during the first 2 days of hospitalization, otherwise it was considered an inadequate CAP evaluation. Administrative billing data were used to identify antibiotics charged within the first 2 days of hospitalization. Empiric guideline-recommended treatment was determined based on 2019 CAP guidelines and more recent studies. Patients who received nonrecommended treatment were evaluated for antibiotic allergies in the current hospitalization or methicillin-resistant Staphylococcus aureus (MRSA) colonization or infection in the year prior or on admission using International Classification of Disease, Tenth Revision (ICD-10) diagnosis codes. Results: We identified 4.47 million adult hospitalizations with CAP from 2013 to 2020; 32% (1.43 million) were included in this analysis (Fig. 1). Among discharges with adequate CAP evaluation (1.37 million), 59.7% received recommended antibiotics in the first 2 days of hospitalization, ranging from 62.6% in 2013 to 57.5% in 2019. Overall, 34.8% of our study population received a nonrecommended antibiotic without documentation of an antibiotic allergy or MRSA colonization (2013: 32.5%; 2018: 36.7%) (Fig. 2). Most patients in our study population received >1 antibiotic (92.3%) in the first 2 days of hospitalization. The most common antibiotics among patients receiving recommended treatment were ceftriaxone (74.2% of patients receiving recommended treatment), azithromycin (67.2%), and levofloxacin (31.8%) (Fig. 3a). The most common nonrecommended antibiotics were vancomycin (57.2% of patients receiving nonrecommended treatment), piperacillin-tazobactam (48.1%), and cefepime (25.7%) (Fig. 3b). From 2013 to 2020, cefepime charges consistently increased among CAP patients treated with nonrecommended antibiotics, whereas levofloxacin charges consistently decreased among CAP patients treated with only recommended antibiotics. Conclusions: Approximately one-third of patients with uncomplicated CAP received nonrecommended empiric antibiotics, and from 2013 to 2020 that proportion increased by 9%. Additional strategies are needed to help identify opportunities to optimize antibiotic selection among patients with CAP.
Disclosures: None



Length of antibiotic therapy among adults aged ≥65 years hospitalized with uncomplicated community-acquired pneumonia, 2013-2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, p. s26
-
- Article
-
- You have access
- Open access
- Export citation
-
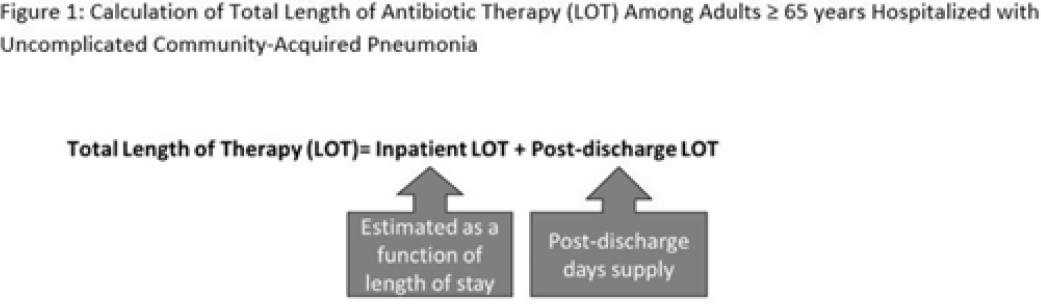
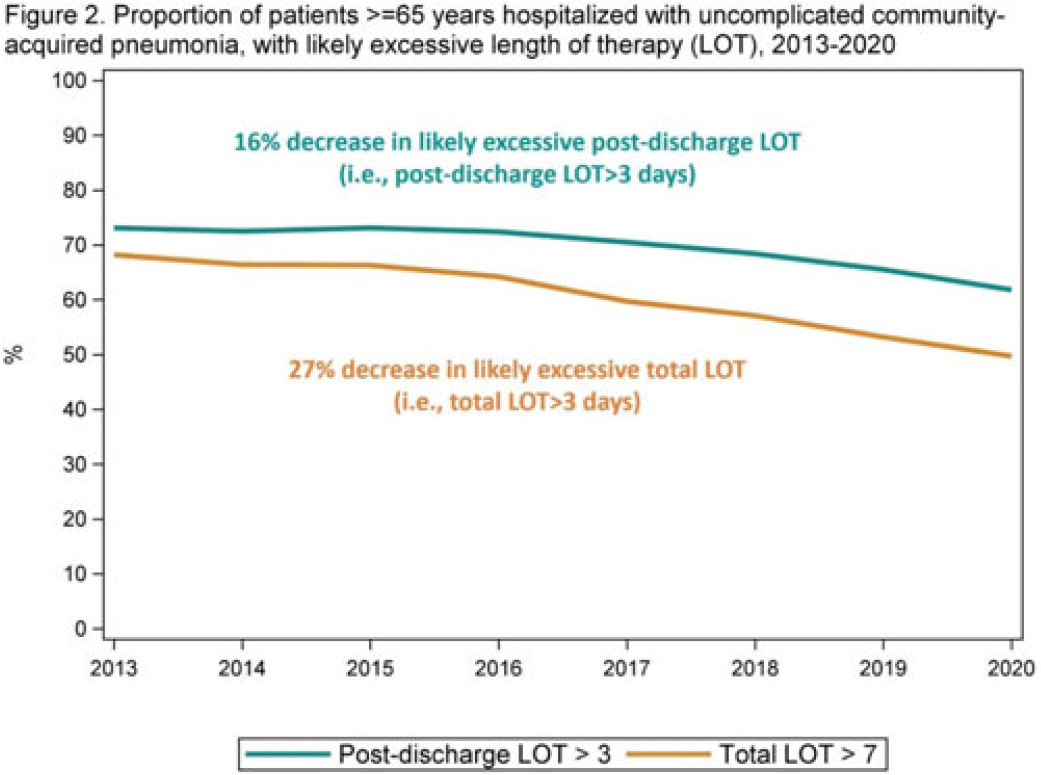
Background: The 2014 US National Strategy for Combating Antibiotic-Resistant Bacteria aimed to reduce inappropriate inpatient antibiotic use by 20% for monitored conditions, such as community-acquired pneumonia (CAP), by 2020. Clinical guidelines recommend treating uncomplicated CAP with a minimum of 5 days of antibiotic therapy. Total length of therapy (LOT) >7 days or >3 days after clinical improvement is rarely necessary. In a previous study estimating LOT in uncomplicated CAP patients, 71% of patients ≥65 years exceeded recommended duration of antibiotics in 2012–2013 (Yi et al, 2018). We evaluated annual trends in LOT in adults ≥65 years hospitalized with uncomplicated CAP from 2013 to 2020. Methods: We conducted a retrospective cohort study among patients in the CMS database with a primary diagnosis of bacterial or unspecified pneumonia using International Classification of Diseases 9th and 10th Revision codes, length of stay (LOS) of 2–10 days, discharged home with self-care, and not rehospitalized in the 3 days following discharge. Discharge home was used as a surrogate for clinical improvement. Because inpatient LOT is not available in CMS data, we used linear regression to model inpatient LOT as a function of LOS using data on CAP patients ≥65 years from the PINC AI healthcare database. Postdischarge LOT was based on prescriptions filled following discharge. Total LOT was calculated by summing estimated inpatient LOT and actual postdischarge LOT (Fig. 1). Total LOT >7 days and postdischarge LOT >3 days were considered indicators of likely excessive LOT. We reported trends in the proportion of patients with likely excessive LOT during the study period. Results: From 2013 through 2020, there were 400,928 uncomplicated CAP hospitalizations among patients aged ≥65 years. Patients were more likely to be female (55%), and they had a median age of 76 years and a median LOS of 3 days. The median total LOT decreased from 9.5 days in 2013 to 7.7 days in 2020. The proportion of patients with total LOT >7 days decreased from 68% in 2013 to 50% in 2020 (% change, −27%); the proportion with postdischarge LOT >3 days decreased from 73% in 2013 to 62% in 2020 (% change, −16%) (Fig. 2). Conclusions: Likely excessive total LOT for adults ≥65 years hospitalized with uncomplicated CAP decreased by 27% in 2020, a considerable improvement from 2013. However, the high proportion of patients with likely excessive postdischarge LOT in 2020 (62%) demonstrates the need for antibiotic stewardship to optimize prescribing at hospital discharge.
Disclosures: None


Characteristics of nursing home residents and healthcare personnel with repeated severe acute respiratory coronavirus virus 2 (SARS-CoV-2) tests positive ≥90 days after initial infection: Four US jurisdictions, July 2020–March 2021
- Part of
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 5 / May 2023
- Published online by Cambridge University Press:
- 20 May 2022, pp. 809-812
- Print publication:
- May 2023
-
- Article
- Export citation
Trends in facility-level rates of Clostridioides difficile infections in US hospitals, 2019–2020
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 44 / Issue 2 / February 2023
- Published online by Cambridge University Press:
- 19 May 2022, pp. 238-245
- Print publication:
- February 2023
-
- Article
- Export citation
Temporal trends in urine-culture rates in the US acute-care hospitals, 2017–2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s12
-
- Article
-
- You have access
- Open access
- Export citation
-
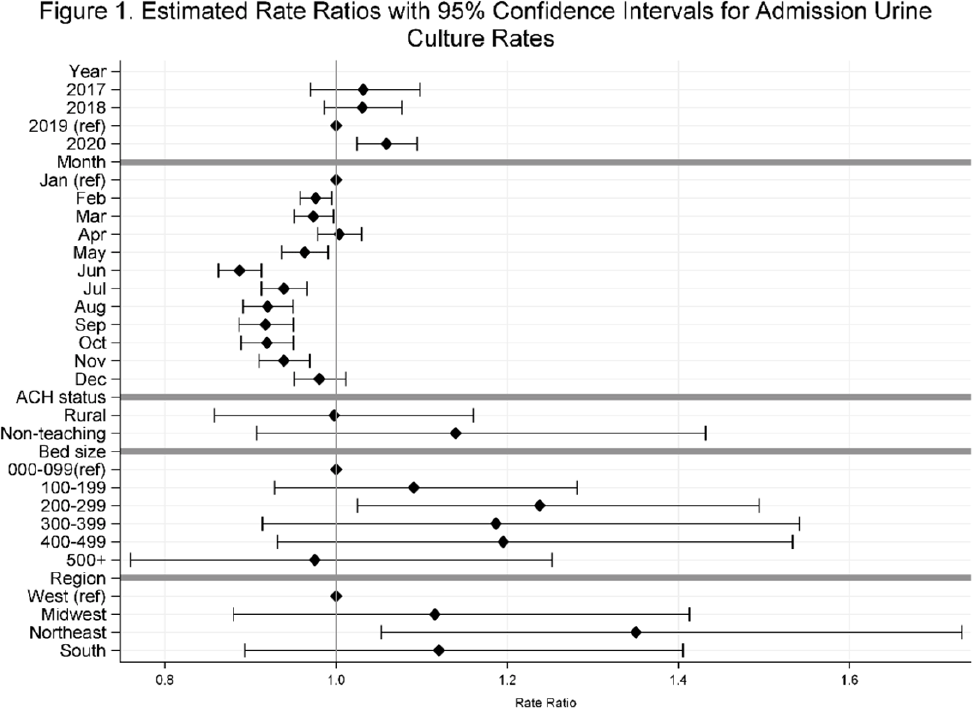
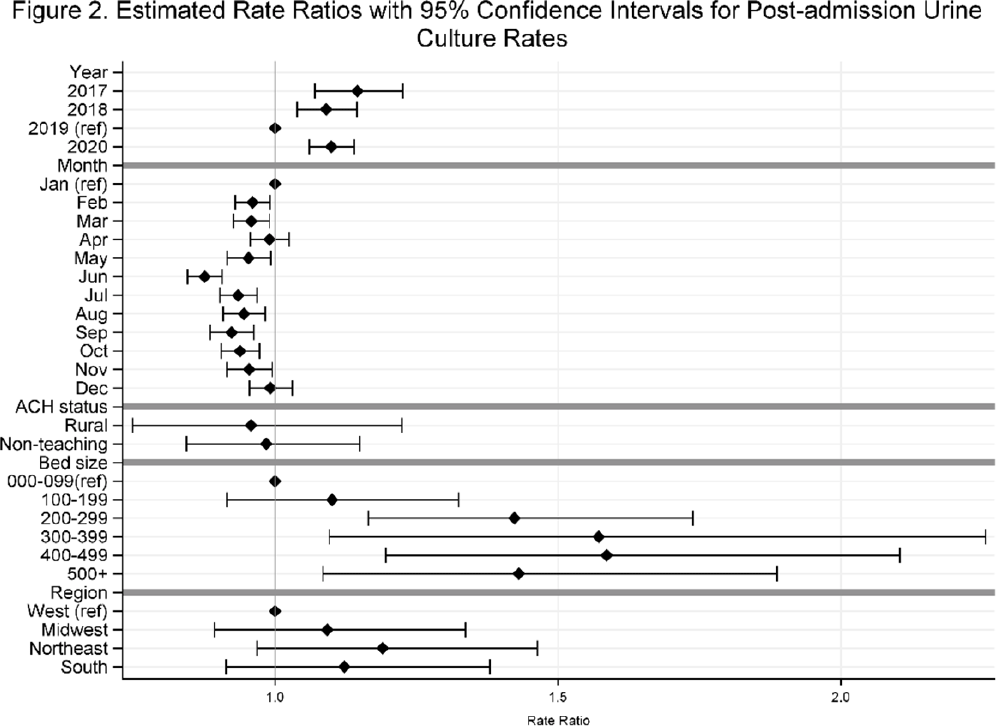
Background: Previously, we reported decreasing postadmission urine-culture rates in hospitalized patients between 2012 and 2017, indicating a possible decrease in hospital-onset urinary tract infections or changes in diagnostic practices in acute-care hospitals (ACHs). In this study, we re-evaluated the trends using more recent data from 2017–2020 to assess whether new trends in hospital urine-culturing practices had emerged. Method: We conducted a longitudinal analysis of monthly urine-culture rates using microbiology data from 355 ACHs participating in the Premier Healthcare Database in 2017–2020. All cultures from the urinary tract collected on or before day 3 were defined as admission urine cultures and those collected on day 4 or later were defined as postadmission urine cultures. We included discharges from months where a hospital reported at least 1 urine culture with microbiology and antimicrobial susceptibility test results. Annual estimates of rates of admission culture and postadmission urine-culture rates were assessed using general estimating equation models with a negative binomial distribution accounting for hospital-level clustering and adjusting for hospital bed size, teaching status, urban–rural designation, discharge month, and census division. Estimated rate for each year (2018, 2019, and 2020) was compared to previous year’s estimated rate using rate ratios (RRs) and 95% confidence intervals (CIs) generated through the multivariable GEE models. Results: From 2017 to 2020, we included 8.7 million discharges and 1,943,540 urine cultures, of which 299,013 (15.4%) were postadmission urine cultures. In 2017–2020, unadjusted admission culture rates were 20.0, 19.6, 17.9, and 18.2 per 100 discharges respectively; similarly, unadjusted postadmission urine-culture rates were 8.6, 7.8, 7.0, and 7.5 per 1,000 patient days. In the multivariable analysis, adjusting for hospital characteristics, no significant changes in admission urine-culture rates were detected during 2017–2019; however, in 2020, admission urine-culture rates increased 6% compared to 2019 (RR, 1.06; 95% CI, 1.02–1.09) (Fig. 1). Postadmission urine-culture rates decreased 4% in 2018 compared to 2017 (RR, 0.96; 95% CI, 0.91–0.99) and 8% in 2019 compared to 2018 (RR, 0.92; 95% CI, 0.87–0.96). In 2020, postadmission urine-culture rates increased 10% compared to 2019 (RR, 1.10; 95% CI, 1.06–1.14) (Fig. 2). Factors significantly associated with postadmission urine-culture rates included discharge month and hospital bed size. For admission urine cultures, discharge month was the only significant factor. Conclusions: Between 2017–2019, postadmission urine-culture rates continued a decreasing trend, while admission culture rates remained unchanged. However, in 2020 both admission and postadmission urine culture rates increased significantly in comparison to 2019.
Funding: None
Disclosures: None


Associations of facility-level antibiotic use and hospital-onset Clostridioides difficile infection in US acute-care hospitals, 2012–2018
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 43 / Issue 8 / August 2022
- Published online by Cambridge University Press:
- 07 May 2021, pp. 1067-1069
- Print publication:
- August 2022
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Pediatric research priorities in healthcare-associated infections and antimicrobial stewardship
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 5 / May 2021
- Published online by Cambridge University Press:
- 26 November 2020, pp. 519-522
- Print publication:
- May 2021
-
- Article
- Export citation
Regional Impact of a CRE Intervention Targeting High Risk Postacute Care Facilities (Chicago PROTECT)
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s48-s49
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Burden and Trends of Hospital-Associated Community-Onset (HACO) Infections From Antibiotic Resistant and Nonresistant Bacteria
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s145
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Substance Use Diagnoses Among Persons with Community-Onset Methicillin-Resistant Staphylococcus aureus Bloodstream Infections
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s392-s393
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Evaluation of Care Interactions Between Healthcare Personnel and Residents in Nursing Homes Across the United States
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s36-s38
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Chlorhexidine MICs Remain Stable Among Antibiotic-Resistant Bacterial Isolates Collected from 2005 to 2019 at Three US Sites
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, p. s26
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
An Interactive Sociotechnical Analysis of the Implementation of Electronic Decision Support in Antimicrobial Stewardship
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s115-s116
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Variability and Trends in Blood Culture Utilization, US Hospitals, 2012–2017
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s430-s431
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
Prescriber perceptions of fluoroquinolones, extended-spectrum cephalosporins, and Clostridioides difficile infection
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 8 / August 2020
- Published online by Cambridge University Press:
- 29 May 2020, pp. 914-920
- Print publication:
- August 2020
-
- Article
- Export citation
Investigation of healthcare infection risks from water-related organisms: Summary of CDC consultations, 2014—2017
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 40 / Issue 6 / June 2019
- Published online by Cambridge University Press:
- 03 April 2019, pp. 621-626
- Print publication:
- June 2019
-
- Article
- Export citation
