



With the increase in the elderly population, globalisation and western lifestyle patterns, obesity and non-communicable diseases, especially cardiovascular disease (CVD), have become a major health burden in the society(Reference Hotez and Peiperl1,Reference Magnusson2) . Metabolic syndrome (MetS), defined as a cluster of cardiovascular risk factors, is strongly associated with an increased risk of CVD and premature mortality(Reference Alberti, Eckel and Grundy3,Reference Chatterjee, Harris and Leiter4) .
Reaven was the first to define MetS in 1988, hypothesising that it was a central feature in the development of diabetes and coronary disease(Reference Reaven5). Later, the WHO developed its first formal definition as the combination of insulin resistance, obesity, dyslipidaemia and hypertension(Reference Alberti and Zimmet6). Nowadays, this syndrome has been widely recognised as a pathologic condition characterised by the presence of central obesity (as elevated waist circumference (WC)), high blood pressure, high glucose and high blood lipids(Reference Huang7–Reference Kassi, Pervanidou and Kaltsas9). Some organisations have proposed cut-off points for four of its five components: plasma levels of glucose, TAG, low HDL as well as blood pressure(Reference Huang7–Reference Kassi, Pervanidou and Kaltsas9). However, although there is an increasing number of populations for which sex-specific cut-off points have been derived (e.g. Indian, African, Chinese and South Asian populations)(Reference Alberti, Eckel and Grundy3), there is not a unique recommendation for central obesity (online Supplementary Table S1). As a result, there is a large number of countries that, due to the lack of available data, are currently using cut-off points derived for white-European populations or other ethnic groups(Reference Alberti, Eckel and Grundy3).
Epidemiological studies conducted in North America and Europe suggest that some ethnic groups such as South Asian, black and Chinese people experience a higher risk of diabetes at lower levels of obesity than whites(Reference Misra, Chowbey and Makkar10–Reference Stommel and Schoenborn13). This suggests that conventional clinical thresholds for obesity that were originally derived from populations of white European background (e.g. the specific case of the body mass index (BMI) ≥ 30·0 kg/m2 or a WC ≥88·0 cm in women or ≥102·0 cm in men) may not be appropriate for non-white groups, such as the Chilean population.
As a consequence, in South American countries where ethnic-specific thresholds for WC have not been proposed, the current recommendation is the use of the already suggested cut-off points for the Asian population (≥90·0 and ≥80·0 cm in men and women, respectively(Reference Alberti, Zimmet and Shaw14)). This guidance has been proposed by the WHO and the International Diabetes Federation (IDF) until country-specific information is available(Reference Alberti, Eckel and Grundy3).
In Chile, the first adopted and used cut-off points were those recommended by the National Cholesterol Education Program Adult Treatment Panel III (ATP III) derived for the US population (≥102·0 and ≥88·0 cm in men and women, respectively)(15). However, since 2014, Chile accepted and included the WHO/IDF cut-off points recommendations, based on Asian data, to prevent CVD(16). However, it remains uncertain whether the Asian-based cut-off points are valid and represent the current anthropometric characteristics of the Chilean population.
Although some attempts have been performed to identify sex-specific cut-off points for WC in Chile, these efforts have been focused on the effect of these thresholds on overweight or cardiometabolic risk rather than MetS, a syndrome associated with a higher risk of CVD and mortality(Reference Villanueva, Arteaga and Maiz17). Therefore, by using nationally representative data from the three national health surveys, this study aimed to identify sex-specific cut-off points for WC in the definition of MetS for the Chilean adult population.
Methods
This study was based on participants aged ≥15 years from the three available Chilean National Health Surveys conducted in 2003, 2009–2010 and 2016–2017. The Chilean National Health Surveys are large, nationally representative population-based studies of biological and lifestyle risk factors, dietary status and health conducted every 6 years in both urban and rural zones(18–20). Data for each survey were collected by trained staff where participants were administered questionnaires, and anthropometrical and physiological measures, as well as biological samples, were obtained. A total of 15 145 participants (59·6 % women) completed at least one of the three surveys (2003: n 3619; 2009–2010: n 5293 and 2016–2017: n 6233). Of these, 8182 (60 % of women) had available information for WC and MetS and were, therefore, included in this study. More information about each survey can be found elsewhere(18–20).
Metabolic syndrome
WC was measured at the mid-axillary line at the midpoint between the costal margin and the iliac crest by an ergonomic circumference measuring tape. Blood samples (TAG, HDL-cholesterol and glucose) were obtained by trained nurses after 8–12 h of fasting using standardised protocols. Systolic and diastolic blood pressure were measured by trained staff and derived from the mean of three readings recorded after 15 min rest(18–20). The average value of these measures by sex is available in online Supplementary Table S2. Each MetS criterion was classified as either present or absent, following the subsequent recommendations of cut-off points: TAG ≥1·7 mmol/l; HDL-cholesterol: <1·3 mmol/l in women and <1·0 mmol/l in men; systolic blood pressure ≥ 130 mmHg and/or diastolic blood pressure ≥ 85 mmHg; and fasting glucose ≥ 5·6 mmol/l or current treatment for diabetes(Reference Huang7–Reference Kassi, Pervanidou and Kaltsas9).
MetS is usually defined as the presence of at least three out of five components(Reference Huang7–Reference Kassi, Pervanidou and Kaltsas9). However, as WC was the outcome in the current study, instead of using three out of five in the definition of MetS, at least two out of four were used to indicate its presence following previous approaches in Latin American studies(Reference Cardinal, Vigo and Duncan21,Reference Mora-García, Gómez-Camargo and Mazenett22) .
Statistical analyses
All analyses were performed in Matlab R2019a. To identify WC cut-off points for the Chilean population, the original data set was divided into two different subsets employing linear binary classification. The overall predicting ability of WC on MetS was quantified by the receiver operating characteristics (ROC) curve and the area under curve (AUC). Identification of errors and correct predictions were carried out by true positives (TP), false positives (FP), false negatives (FN), and true negatives (TN) as follows:
-
Sensitivity (or true positive rate) defined as:
 ${\rm{Sensitivity}} = {{TP} \over {TP + FN}};$
${\rm{Sensitivity}} = {{TP} \over {TP + FN}};$
-
Specificity (or true negative rate) defined as:
${\rm{Specificity}} = {{TN} \over {TN + FP}}$
-
Type I error (or false positive rate) defined as:
${R_{FP}} = {{FP} \over {TN + FP}} = 1 - {\rm{specificity}};$
-
Type II error (or false negative rate) defined as:
${R_{FN}} = {{FN} \over {TP + FN}} = 1 - {\rm{sensitivity}};$




The optimal WC value was assigned as the one that minimises the errors, that is, the sum of false positive rate and the false negative rate (RFP + RFN ). We decided to use this approach, rather than other methods (e.g. Youden index, LR+, LR−), because we think it is important to balance between the numbers of false positive and false negative. The optimal cut-off point for the Chilean population was computed by sex considering the full data set (8182 participants). Besides, a sensitivity analysis was performed to identify if the optimal cut-off points differ by age (below and above 60 years).
Additionally, we performed 10 000 bootstrapping to derive the 95 % CI of cut-off points for WC, as well as the descriptive statistic. Each bootstrapping was restricted to have at least between 40 and 60 % of the original population (i.e. 2000 participants were included in each bootstrapping). To compare the cut-off points derived in our study with those suggested by WHO/IDF and ATP III, we plotted the sensitivity/specificity of each of these guidelines using the Chilean data set.
Finally, the prevalence of MetS was computed depending on the cut-off points of WC. Three different points were considered for posterior analysis recovered with the presented methodology and the international recommendations. Differences between those thresholds’ values were estimated.
Results
Figure 1 presents the receiver operating characteristics curve derived for the Chilean population, with their corresponding 95 % CI (AUC for men 0·74 (95 % CI 0·72, 0·76); AUC for women 0·71 (95 % CI 0·68, 0·73)). The optimal cut-off points for WC, in the definition of MetS by sex, were 92·3 cm (95 % CI 90·5, 94·4) and 87·6 cm (95 % CI 85·8, 92·1) for men and women, respectively (Fig. 1 and online Supplementary Fig. S1). These derived Chilean WC cut-off points had a higher sensitivity than the cut-off points recommended by the ATP III and higher specificity in contrast to those recommended by WHO/IDF, both in men and women. When the analyses were stratified by age (below or above 60 years), the WC cut-off points for both age groups lied within the 95 % CI already derived for the whole population for both age groups (online Supplementary Fig. S2).
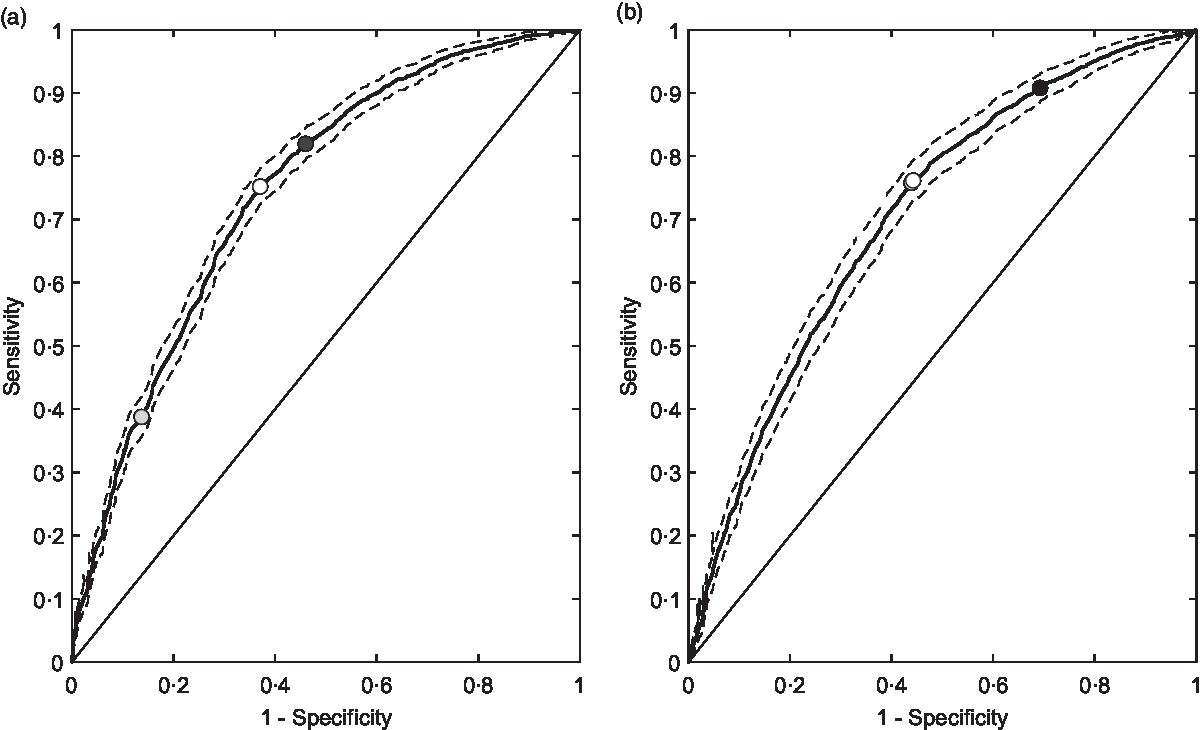
Fig. 1 Receiver operating characteristics (ROC) analyses for waist circumference in the definition of metabolic syndrome (MetS) by sex. (a) Optimal cut-off point for men in Chile, its AUC with its 95 % CI. In addition, the figure compares the threshold with the international recommendations. (b) Same information for women. MetS was defined as the presence of ≥2 of the following conditions: TAG ≥1·7 mmol/l; HDL-cholesterol: <1·3 mmol/l in women and <1·0 mmol/l in men; systolic blood pressure ≥ 130 mm Hg and/or diastolic blood pressure ≥ 85 mm Hg; fasting glucose ≥ 5·6 mmol/l or current treatment for diabetes. (a) ![]() , ROC (AUC = 0·74);
, ROC (AUC = 0·74); ![]() , Random ROC (AUC = 0·50);
, Random ROC (AUC = 0·50); ![]() , 95 % CI;
, 95 % CI; ![]() , WHO/International Diabetes Federation (IDF) = 90·0 cm;
, WHO/International Diabetes Federation (IDF) = 90·0 cm; ![]() , National Cholesterol Education Program Adult Treatment Panel III (ATP III) = 102·0 cm;
, National Cholesterol Education Program Adult Treatment Panel III (ATP III) = 102·0 cm; ![]() , Chile = 92·3 cm. (b)
, Chile = 92·3 cm. (b) ![]() , ROC (AUC = 0·71);
, ROC (AUC = 0·71); ![]() , Random ROC (AUC = 0·50);
, Random ROC (AUC = 0·50); ![]() , 95 % CI;
, 95 % CI; ![]() , WHO/IDF = 80·0 cm;
, WHO/IDF = 80·0 cm; ![]() , ATP III = 88·0 cm;
, ATP III = 88·0 cm; ![]() , Chile = 87·6 cm
, Chile = 87·6 cm
The descriptive statistic of the bootstrapping analyses is presented in online Supplementary Fig. S1 (median and mode). The probability of having a cut-off point according to the WHO/IDF was 6·6 and 0·0 % for men and women, respectively. In turn, according to ATP III, it was 0·0 and 62·2 % for men and women, respectively. Therefore, the ATP III recommendation for Chilean men and the WHO recommendation for Chilean women can be considered outliers (online Supplementary Fig. S1).
Finally, the prevalence of MetS using different cut-off points for WC is presented in Fig. 2. Using the identified cut-off point of 92·3 cm in men, the prevalence of MetS was 38·9 %. This prevalence was 2·9 % lower and 18·5 % higher than the WHO/IDF and ATP III recommendations, respectively (Fig. 2(a)). For women, the identified WC cut-off point of 87·6 cm was associated with a 33 % prevalence of MetS, which was 6·1 % lower and only 0·4 % higher than the WHO/IDF and ATP III recommendations, respectively (Fig. 2(b)).
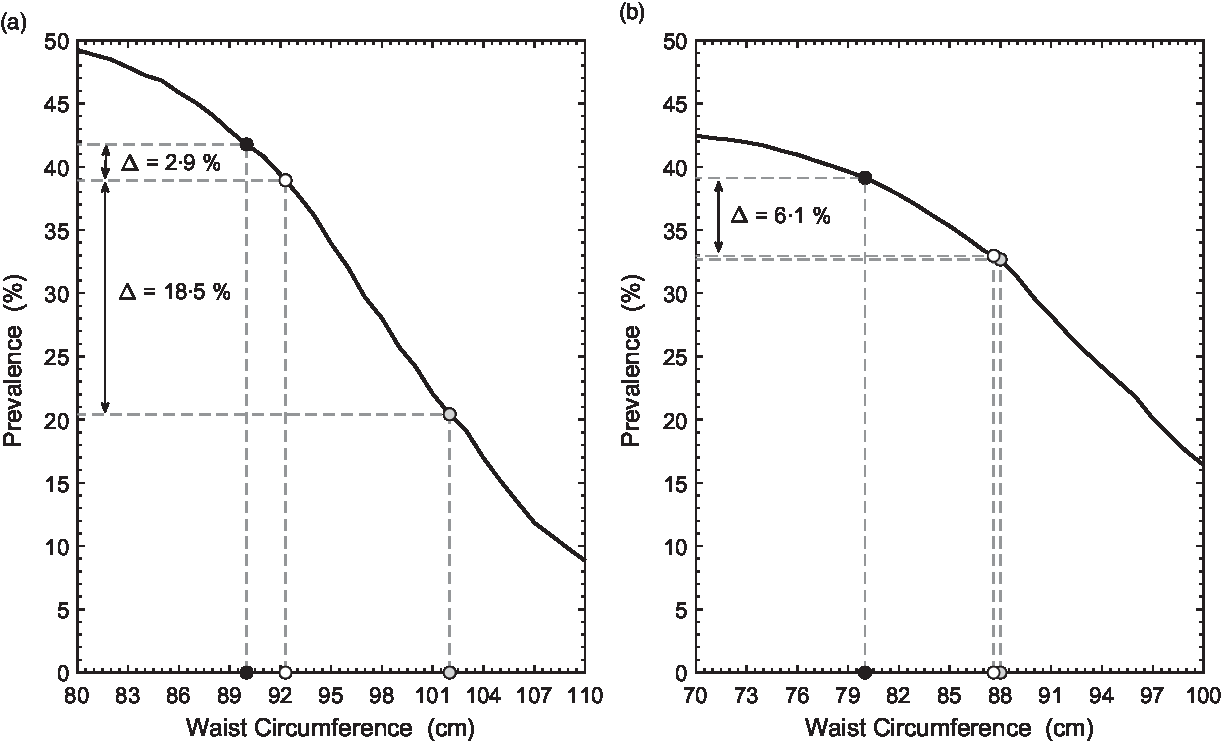
Fig. 2 Prevalence of metabolic syndrome (MetS) in Chilean adults using different cut-off points for waist circumference (WC). (a) Prevalence of MetS in men using different thresholds of WC. In addition, this figure shows the delta between the threshold identified and the international recommendations. (b) Same information for women. For this Figure, MetS was defined as the presence of ≥2 of the following conditions: TAG ≥1·7 mmol/l; HDL-cholesterol: <1·3 mmol/l in women and <1·0 mmol/l in men; systolic blood pressure ≥ 130 mm Hg and/or diastolic blood pressure ≥ 85 mm Hg; fasting glucose ≥ 5·6 mmol/l or current treatment for diabetes plus different cut-off points of WC. (a) ![]() , Prevalence of MetS;
, Prevalence of MetS; ![]() , WHO/International Diabetes Federation (IDF) = 90·0 cm;
, WHO/International Diabetes Federation (IDF) = 90·0 cm; ![]() , National Cholesterol Education Program Adult Treatment Panel III (ATP III) = 102·0 cm;
, National Cholesterol Education Program Adult Treatment Panel III (ATP III) = 102·0 cm; ![]() , Chile = 92·3 cm. (b)
, Chile = 92·3 cm. (b) ![]() , Prevalence of MetS;
, Prevalence of MetS; ![]() , WHO/IDF = 80·0 cm;
, WHO/IDF = 80·0 cm; ![]() , ATP III = 88·0 cm;
, ATP III = 88·0 cm; ![]() , Chile = 87·6 cm
, Chile = 87·6 cm
Discussion
Since 2014, Chile has used the WHO/IDF recommendation for WC cut-off points for the Asian populations(16). This recommendation was established in 2005 due to the lack of information for South and Central American populations and, after 15 years, still prevails(Reference Alberti, Zimmet and Shaw14). To our knowledge, this is the first study identifying sex-specific cut-off points for WC in the definition of MetS for the Chilean population. The main findings of this study provide evidence that the current suggestions of using WC cut-off points derived for Asian populations may not be appropriate for the Chilean population, especially for women who – based on our estimates – should have a cut-off point 7·6 cm higher than the current recommendation. In our study, the cut-off points derived for women were closer to those suggested by the ATP III recommendation for American women (88·0 cm). However, for men, we found that the WC cut-off (92·3 cm) was somehow in the middle between the Asian (90·0 cm) and the IDF recommendations for Caucasian men (94·0 cm)(Reference Alberti, Eckel and Grundy3,Reference Alberti, Zimmet and Shaw14) . In addition, using the identified cut-off points, the prevalence of MetS was 2·9 and 6·1 % lower than the current recommendation for men and women, respectively. In this regard, although our cut-off points were closer to those recommended by the WHO/IDF for men, adopting the WHO/IDF recommendation for women could overestimate the number of individuals at risk. Changing these cut-off points for women may decrease the prevalence of this syndrome in Chile. Therefore, considering that the prevalence of MetS is highly sensitive when different thresholds for WC are used, more conservative cut-off points (i.e. low values) could not be necessarily representative of the national reality. The aforementioned motivates its calibration for each population and a more in-depth study across countries.
BMI and WC are both measures of adiposity. However, the cut-off points for overweight and obesity are different in Chile and Asia (BMI ≥25 and ≥23 kg/m2, respectively)(23). Therefore, considering the same cut-off points for WC for both populations could not be justified. Moreover, the Asian population in Chile represents only 1·2 % of the total Chilean population. In consequence, there are no foundations in the use of these thresholds due to the underlying differences in anthropometry and a small proportion in the population(24).
Although this is the first study in Chile that suggests sex-specific cut-off points for WC in the definition of MetS, a previous study, conducted by Villanueva et al.(Reference Villanueva, Arteaga and Maiz17), suggested sex-specific cut-off points for abdominal obesity to identify cardiovascular risk factors in adults. The authors demonstrated that thresholds of 93 and 88 cm in non-obese men and women, and 91 and 83 cm in overweight/obese men and women were associated with cardiovascular risk factors; that is, our findings were similar to those found for Villanueva et al.(Reference Villanueva, Arteaga and Maiz17) for non-obese adults. Nevertheless, It is important to highlight that the Villanueva study and our study are different in the number of participants included and the identification of cut-off points in both studies had a different aim.
Other South American studies have also found similar results using similar approaches. Aschner et al.(Reference Aschner, Buendia and Brajkovich25), using data from 179 men and 278 women from Mexico, El Salvador, Venezuela, Colombia and Paraguay, identified that the optimal WC thresholds were 94·0 cm and between 90·0 and 92·0 cm for South American men and women, respectively(Reference Aschner, Buendia and Brajkovich25). This recommendation has also been considered by the Latin American Association of Diabetes. In Brazil, after analysing 6772 men and 8121 women, Cardinal et al.(Reference Cardinal, Vigo and Duncan21) found cut-off points of 92·0 and 86·6 cm for men and women, respectively(Reference Cardinal, Vigo and Duncan21). In Colombia, Mora-García identified a threshold of 85·0 cm in women(Reference Mora-García, Gómez-Camargo and Mazenett22). In Venezuela, Bermúdez et al.(Reference Bermúdez, Rojas and Salazar26) found that 95·2 and 90·2 cm were the cut-off points with the highest sensitivity after analysing 1902 adults from Maracaibo. Therefore, all the reported South American cut-off points (including those of this study) are far from the WHO/IDF recommendations for South Americans. Furthermore, as sex-specific cut-off points to determine central obesity should not be applied universally among different ethnicities or countries, future work should aim to define ethnic and country-specific cut-off points in other populations.
Strength and limitations
This study was performed employing all the available data from the Chilean National Health Surveys that are a nationally representative sample of the Chilean adult population. In addition, all blood samples (TAG, HDL-cholesterol and glucose), systolic blood pressure and diastolic blood pressure measures used to define MetS were obtained by trained nurses using standardised protocols(18–20). However, these data were obtained during three different periods and on different participants. Further investigations considering a larger data set should be carried out to generalise the obtained results.
Conclusion
In conclusion, the current WHO/IDF recommendation for WC was not supported by Chilean data for women, but it was closer for men. Using the three Chilean National Health Surveys, we identified that 92·3 and 87·6 cm could be better cut-off points for WC in the definition of MetS. As a result, the current ATP III recommendation for American women (88·0 cm) and the IDF for Caucasian men (94·0 cm) are closer to the Chilean reality. Future prospective studies should corroborate this information investigating the association of these cut-off points with incidence and mortality for CVD and all-cause mortality.
Acknowledgements
Acknowledgements: We thank all participants for their co-operation and the Chilean Health Ministry and School of Public Health, The Pontificia Universidad Católica de Chile for commissioning, designing and conducting the three National Health Surveys. Financial support This study was funded by the Chilean Health Ministry as part of the health surveillance in Chile. The funders of the study had no role in study design, data collection, data analysis, data interpretation or any decision related to this article. Conflict of interest: None to declare. Authorship: F.P.-R., C.C.-M. and A.P. generated the research question. F.P.-R. and A.P. planned the analysis. F.P.-R. performed the literature search. F.P.-R. and A.P. performed the analyses with support from C.C.-M. F.P.-R. and A.P. wrote the first draft of the manuscript. All authors critically reviewed this and previous drafts. All authors approved the final draft for submission. F.P.R. is the guarantor. Ethics of human subject participation: The Chilean National Health Surveys were funded by the Chilean Ministry of Health and led by the Department of Public Health of the Pontificia Universidad Católica de Chile. The Chilean National Health Surveys were approved by the Ethics Research Committee of the Faculty of Medicine at the same university. All participants who participated provided written informed consent.
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020001469




