

No CrossRef data available.
Article contents
Ambulatory antibiotic prescribing for children in a practice research network
Published online by Cambridge University Press: 29 September 2023
Abstract
Core share and HTML view are not available for this content. However, as you have access to this content, a full PDF is available via the ‘Save PDF’ action button.
Background: Most antibiotic use occurs in ambulatory settings. Antibiotic prescribing for children living in the United States in medically underserved areas or in populations is not well understood.
Objective: To characterize antibiotic prescribing for children in a practice-based research network (PBRN).
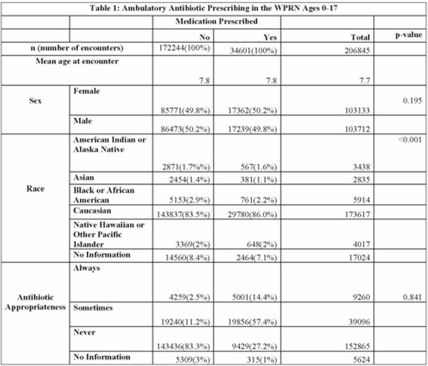
Design and Methods: In this retrospective cohort study, we characterized oral antibiotic prescribing in a large PBRN. Patients aged 0–17 years with at least 1 in-person visit between January 1, 2014, and December 31, 2018, at 1 of 25 primary-care clinics located within the WWAMI (Washington, Wyoming, Alaska, Montana, and Idaho) region of the Practice and Research Network (WPRN) were included. Data were extracted from DataQUEST, a centralized data repository from included primary-care clinics. Encounters for wellness visits or those lacking a diagnosis code and patients with complex chronic conditions were excluded. Diagnoses were categorized using International Classification of Disease, Ninth Revision (ICD-9) and ICD-10 codes. Oral antibiotics prescribed within 3 days of an encounter were associated with that encounter. Demographic data included age, sex, race, and ethnicity. Antibiotic appropriateness was determined using a previously published 3-tiered classification system using diagnosis codes as always, sometimes, or never appropriate. Patient-level data (ZIP codes) were used to designate medically underserved areas (MUAs) and medically underserved populations (MUPs). Antibiotic prescribing was then analyzed within these groups. Results: In total, 37,314 patients across 206,845 encounters were included, of which 34,601 encounters (17%) resulted in antibiotic prescription (Table 1). Of those, appropriateness data were available for 34,286 (99%). Of the antibiotics prescribed, 14% were always appropriate, 57% were sometimes appropriate, and 27% were never appropriate (1% missing). In total, 64% and 35% of encounters occurred with patients from an MUA and MUP, respectively. Conclusions: Targets to improve oral antibiotic prescribing for children in a large PBRN include antibiotic prescribing for diagnoses that never require an antibiotic. Larger comparative studies may focus on the role (if any) that MUA/MUP has on antibiotic prescribing.
Disclosures: None
- Type
- Antibiotic Stewardship
- Information
- Antimicrobial Stewardship & Healthcare Epidemiology , Volume 3 , Issue S2: SHEA Spring 2023 Abstracts , June 2023 , pp. s40 - s41
- Creative Commons

 This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution licence (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted re-use, distribution, and reproduction in any medium, provided the original work is properly cited.- Copyright
- © The Author(s), 2023. Published by Cambridge University Press on behalf of The Society for Healthcare Epidemiology of America
 You have
Access
You have
Access
 Open access
Open access