
FirstView
Contents
Original Article
Outcomes and characteristics in term infants with necrotising enterocolitis and CHD
- Sean T. Kelleher, John Coleman, Colin J. McMahon, Adam James
-
- Published online by Cambridge University Press:
- 02 January 2024, pp. 1-7
-
- Article
-
- You have access Access
- Open access
- HTML
- Export citation
-
Background:
CHD is a significant risk factor for the development of necrotising enterocolitis. Existing literature does not differentiate between term and preterm populations. Long-term outcomes of these patients are not well understood. The aim was to investigate the baseline characteristics and outcomes of term normal birth weight infants with CHD who developed necrotising enterocolitis.
Methods:A retrospective review was performed of infants from a single tertiary centre with CHD who developed necrotising enterocolitis of Bell’s Stage 1–3, over a ten-year period. Inclusion criteria was those born greater than 36 weeks’ gestation and birth weight over 2500g. Exclusion criteria included congenital gastro-intestinal abnormalities. Sub-group analysis was performed using Fisher’s exact test.
Results:Twenty-five patients were identified, with a median gestational age of 38 weeks. Patients with univentricular physiology accounted for 32% (n = 8) and 52% of patients (n = 13) had a duct-dependent lesion. Atrioventricular septal defect was the most common cardiac diagnosis (n = 6, 24%). Patients with trisomy 21 accounted for 20% of cases. Mortality within 30 days of necrotising enterocolitis was 20%. Long-term mortality was 40%, which increased with increasing Bell’s Stage. In total, 36% (n = 9) required surgical management of necrotising enterocolitis, the rate of which was significantly higher in trisomy 21 cases (p < 0.05).
Conclusion:Not previously described in term infants is the high rate of trisomy 21 and atrioventricular septal defect. This may reflect higher baseline incidence in our population. Infants with trisomy 21 were more likely to develop surgical necrotising enterocolitis. Mortality at long-term follow-up was high in patients with Bell’s Stage 2–3.
Predictors of early peritoneal dialysis initiation in newborns and young infants following cardiac surgery
- Elvia Rivera-Figueroa, Md Abu Yusuf M Ansari, Emily Turner Mallory, Padma Garg, Ali Mirza Onder
-
- Published online by Cambridge University Press:
- 02 January 2024, pp. 1-8
-
- Article
- Export citation
-
Objective:
This single-centre, retrospective cohort study was conducted to investigate the predictors of early peritoneal dialysis initiation in newborns and young infants undergoing cardiac surgery.
Methods:There were fifty-seven newborns and young infants. All subjects received peritoneal dialysis catheter after completion of the cardiopulmonary bypass. Worsening post-operative (post-op) positive fluid balance and oliguria (<1 ml/kg/hour) despite furosemide were the clinical indications to start early peritoneal dialysis (peritoneal dialysis +). Demographic, clinical, and laboratory data were collected from the pre-operative, intra-operative, and immediately post-operative periods.
Results:Baseline demographic data were indifferent except that peritoneal dialysis + group had more newborns. Pre-operative serum creatinine was higher for peritoneal dialysis + group (p = 0.025). Peritoneal dialysis + group had longer cardiopulmonary bypass time (p = 0.044), longer aorta cross-clamp time (p = 0.044), and less urine output during post-op 24 hours (p = 0.008). In the univariate logistic regression model, pre-op serum creatinine was significantly associated with higher odds of being in peritoneal dialysis + (p = 0.021) and post-op systolic blood pressure (p = 0.018) and post-op mean arterial pressure (p=0.001) were significantly associated with reduced odds of being in peritoneal dialysis + (p = 0.018 and p = 0.001, respectively). Post-op mean arterial pressure showed a statistically significant association adjusted odds ratio = 0.89, 95% confidence interval [0.81, 0.96], p = 0.004) with peritoneal dialysis + in multivariate analysis after adjusting for age at surgery.
Conclusions:In our single-centre cohort, pre-op serum creatinine, post-op systolic blood pressure, and mean arterial pressure demonstrated statistically significant association with peritoneal dialysis +. This finding may help to better risk stratify newborns and young infants for early peritoneal dialysis start following cardiac surgery.
Patient factors and geographic barriers influencing excess time between paediatric and adult CHD care
- Jessica Patzer, Maryna Yaskina, Alyssa Chappell, David Patton, Nanette Alvarez, Frank Dicke, Andrew S. Mackie
-
- Published online by Cambridge University Press:
- 27 December 2023, pp. 1-8
-
- Article
-
- You have access Access
- Open access
- HTML
- Export citation
-
Introduction:
Over 90% of children with CHD survive into adulthood and require lifelong cardiology care. Delays in care predispose patients to cardiac complications. We sought to determine the time interval to accessing adult CHD care beyond what was recommended by the referring paediatric cardiologist (excess time) and determine risk factors for prolonged excess time.
Materials and Methods:Retrospective cohort study including all patients in the province of Alberta, Canada, age 16–18 years at their last paediatric cardiology visit, with moderate or complex lesions. Excess time between paediatric and adult care was defined as the interval (months) between the final paediatric visit and the first adult visit, minus the recommended interval between these appointments. Patients whose first adult CHD appointment occurred earlier than the recommended interval were assigned an excess time of zero.
Results:We included 286 patients (66% male, mean age 17.6 years). Mean excess time was 7.9 ± 15.9 months. Twenty-nine (10%) had an excess time > 24 months. Not having a pacemaker (p = 0.03) and not needing cardiac medications at transfer (p = 0.02) were risk factors for excess time >3 months. Excess time was not influenced by CHD complexity.
Discussion:The mean delay to first adult CHD appointment was almost 8 months longer than recommended by referring paediatric cardiologists. Not having a pacemaker and not needing cardiac medication(s) were risk factors for excess time > 3 months. Greater outpatient resources are required to accommodate the growing number of adult CHD survivors.
Should pediatric cardiologists refer all patients with unexplained chest pain to a psychiatrist?
- Fatos Alkan, Sermin Yalın Sapmaz, Cansın Kardelen, Onur Bircan, Oznur Bilac, Hasan Kandemir, Senol Coskun
-
- Published online by Cambridge University Press:
- 27 December 2023, pp. 1-7
-
- Article
- Export citation
-
Objective:
The present study aimed to investigate the relationship between unexplained chest pain in children with parents’ mental problems, parental attitudes, family functionality, and the child’s mental problems.
Material and Method:A total of 433 children (between 11 and 18 years of age) applied to the Pediatric Cardiology Outpatient Clinic due to chest pain in the last year. A clinical interview was conducted by a child psychiatrist with 43 patients and 33 controls included in the study due to unexplained chest pain.
Results:Family history of physical illness was significantly higher in the chest pain group. When evaluated in terms of psychosocial risk factors, life events causing difficulties, derangement in the family, loss of a close person, and exposure to violence were statistically significantly higher in the group with chest pain. Mental disorders were observed in 67.4% of the children in the chest pain group as a result of the clinical interview. The total score of the DSM-5 somatic symptoms scale, which evaluates other somatic complaints in the chest pain group, was also significantly higher. When the family functions of both groups were evaluated, communication, emotional response, behaviour control, and general functions sub-dimensions were statistically significantly higher in families in the chest pain group.
Conclusion:We recommend that psychiatric evaluation be included in diagnostic research to prevent unnecessary medical diagnostic procedures in children describing unexplained chest pain, as well as to prevent the potential for diagnosing mental disorders in both children and adults.
British Congenital Cardiac Association Fetal Cardiology Standards: impact of Patient and Public involvement exercise on the development of clinical standards
- Myra Bluebond-Langner, Sara Wakeling, Katherine Vincent, Ashleigh Butler, Kate Brown, Victoria Jowett
-
- Published online by Cambridge University Press:
- 22 December 2023, pp. 1-5
-
- Article
-
- You have access Access
- Open access
- HTML
- Export citation
-
Objective:
To examine the impact of a Patient and Public Involvement exercise on the development of British Congenital Cardiac Association Fetal Cardiology Standards 2021.
Design:Open-ended, semi-structured interviews were undertaken to inform the design of a study to improve the quality of parents’ experiences during antenatal and perinatal care of their child with CHD. This Patient and Public Involvement exercise was used to inform the final version of the drafted ‘Standards’.
Setting:One-on-one interviews with parents who responded to a request on the closed Facebook page of the user group “Little Hearts Matter”: “Would you be interested in helping us to design a study about parents’ experience on learning that their child had CHD”?
Patients:Parents of children with single ventricle CHD.
Results:Twenty-one parents (18 mothers, 3 fathers) participated. Parents responses were reported to have variably reinforced, augmented, and added specificity in the later stages of drafting to six of the seven subsections of Section C Information and Support for Parents including: “At the time of the Scan”; “Counselling following the identification of an abnormality”; “Written information/resources”; “Parent support”; “Communication with other teams and ongoing care”; and “Bereavement support”.
Conclusions:This Patient and Public Involvement exercise successfully informed the development of Standards after the initial drafting. It contributed to the establishment of face validity of the ‘Standards’, especially when consistent with what is reported in the literature. Further research is needed to explore approaches to involving and standardising Patient and Public Involvement in the development of clinical standards.
Evaluation of the use of visual storytelling as an educational intervention in the cardiac ICU: reaching parents before they are in crisis
- Meghan M. Chlebowski, Christiana Stark, Philip R. Khoury, Huaiyu Zang, Julia Baenziger, Nadine A. Kasparian
-
- Published online by Cambridge University Press:
- 22 December 2023, pp. 1-9
-
- Article
-
- You have access Access
- Open access
- HTML
- Export citation
-
Objective:
To evaluate the acceptability and safety of educational videos utilising visual storytelling to provide information about the cardiac ICU and post-operative care to parents. Videos were designed to educate, further encourage parents to engage in their child’s cardiac care, and address common sources of distress.
Study Design:Two educational videos and survey were sent to 29 families of children previously admitted to the cardiac ICU (April 2020–March 2021). Views regarding information quality, quantity, format, and relevance were assessed, as were parents’ emotional responses. Quantitative thresholds for safety and acceptability were set a priori. An inductive approach to content analysis was applied to identify themes in qualitative data.
Results:Sixteen parents participated (response rate: 55%). All acceptability and safety thresholds were met; 92% of parents rated the videos as helpful and 85% were “very” or “extremely likely” to recommend them to other families of children with CHD. No participants reported significant distress after viewing the videos. Expressions of parental engagement with their child’s care team were common (92%). In qualitative responses, parents perceived the videos as potentially helpful in reducing distress if viewed prior to cardiac ICU admission.
Conclusion:Visual storytelling to orient parents to the cardiac ICU and address common stressors was found to be safe and acceptable when tested with parents of children previously admitted to the cardiac ICU. Further prospective studies are needed to test intervention effects when videos are viewed before or during cardiac ICU admission, especially for mitigating anxiety and traumatic stress associated with admission.
Ketorolac in neonates and infants following congenital heart surgery: a retrospective review
- Amy L. Kiskaddon, Arabela C. Stock, Jamie L. Fierstein, Alexandra Miller, James A. Quintessenza, Neil Goldenberg
-
- Published online by Cambridge University Press:
- 22 December 2023, pp. 1-7
-
- Article
-
- You have access Access
- Open access
- HTML
- Export citation
-
Introduction:
Pain management is essential in the immediate post-surgical period. We sought to describe the ketorolac dose regimen in neonates and infants following cardiac surgery. Secondary outcomes included renal dysfunction, bleeding, and pain management.
Methods:We performed a single-centre retrospective cohort study of neonates and infants (aged < 12 months) who received ketorolac following cardiac surgery, from November 2020 through November 2021 (inclusive). Ketorolac was administered at 0.5 mg/kg every 6 hours. Safety was defined by absence of a clinically significant decline in renal function (i.e., increase in serum creatinine [SCr] by ≥ 0.3 mg/dL from baseline within 48 hours and/or urine output ≤ 0.5 mL/kg/hour for 6 hours) and absence of clinically significant bleeding defined as major by International Society on Thrombosis and Hemostasis paediatric criteria or Severe/Fatal Bleeding Events by Nellis et al. Efficacy measures included pain scores and opioid utilisation.
Results:Fifty-five patients met eligibility criteria. The median (range) dose and duration of ketorolac administration was 0.5 mg/kg/dose for 48 (6–90) hours. Among all patients, there was not a statistically significant difference observed in median SCr within 48 hours of baseline (p > .9). There were no major or severe bleeding events. The median (range) opioid requirements (morphine intravenous equivalents per kg per day) at 48 hours post-ketorolac initiation was 0.1 (0–0.8) mg/kg/day.
Conclusions:If validated prospectively, these findings suggest that a ketorolac regimen 0.5 mg/kg/dose every 6 hours in neonates and infants post-cardiac surgery may be safe with regard to renal function and bleeding risk, and effective regarding opioid-sparing capacity.
Bullying among children with heart conditions, National Survey of Children’s Health, 2018–2020
- Brittany N. Wright, M. Jill Glidewell, Karrie F. Downing, Kevin J. Vagi, Michael P. Fundora, Sherry L. Farr
-
- Published online by Cambridge University Press:
- 19 December 2023, pp. 1-9
-
- Article
- Export citation
-
Children with chronic illnesses report being bullied by peers, yet little is known about bullying among children with heart conditions. Using 2018–2020 National Survey of Children’s Health data, the prevalence and frequency of being bullied in the past year (never; annually or monthly; weekly or daily) were compared between children aged 6–17 years with and without heart conditions. Among children with heart conditions, associations between demographic and health characteristics and being bullied, and prevalence of diagnosed anxiety or depression by bullying status were examined. Differences were assessed with chi-square tests and multivariable logistic regression using predicted marginals to produce adjusted prevalence ratios and 95% confidence intervals. Weights yielded national estimates. Of 69,428 children, 2.2% had heart conditions. Children with heart conditions, compared to those without, were more likely to be bullied (56.3% and 43.3% respectively; adjusted prevalence ratio [95% confidence interval] = 1.3 [1.2, 1.4]) and bullied more frequently (weekly or daily = 11.2% and 5.3%; p < 0.001). Among children with heart conditions, characteristics associated with greater odds of weekly or daily bullying included ages 9–11 years compared to 15–17 years (3.4 [2.0, 5.7]), other genetic or inherited condition (1.7 [1.0, 3.0]), ever overweight (1.7 [1.0, 2.8]), and a functional limitation (4.8 [2.7, 8.5]). Children with heart conditions who were bullied, compared to never, more commonly had anxiety (40.1%, 25.9%, and 12.8%, respectively) and depression (18.0%, 9.3%, and 4.7%; p < 0.01 for both). Findings highlight the social and psychological needs of children with heart conditions.
Conjugated hyperbilirubinemia is associated with increased morbidity and mortality after neonatal heart surgery
- Mallory Hunt, Iris E.M. de Jong, Rebecca G. Wells, Amit A. Shah, Pierre Russo, Marlene Mahle, Monique M. Gardner, Stephanie Fuller, Jonathan Chen, J. William Gaynor
-
- Published online by Cambridge University Press:
- 18 December 2023, pp. 1-8
-
- Article
- Export citation
-
Background:
Cholestasis characterised by conjugated hyperbilirubinemia is a marker of hepatobiliary dysfunction following neonatal cardiac surgery. We aimed to characterise the incidence of conjugated hyperbilirubinemia following neonatal heart surgery and examine the effect of conjugated hyperbilirubinemia on post-operative morbidity and mortality.
Methods:This was a retrospective study of all neonates who underwent surgery for congenital heart disease (CHD) at our institution between 1/1/2010 and 12/31/2020. Patient- and surgery-specific data were abstracted from local registry data and review of the medical record. Conjugated hyperbilirubinemia was defined as perioperative maximum conjugated bilirubin level > 1 mg/dL. The primary outcome was in-hospital mortality. Survival analysis was conducted using the Kaplan–Meier survival function.
Results:Conjugated hyperbilirubinemia occurred in 8.5% of patients during the study period. Neonates with conjugated hyperbilirubinemia were more likely to be of younger gestational age, lower birth weight, and non-Caucasian race (all p < 0.001). Patients with conjugated hyperbilirubinemia were more likely to have chromosomal and non-cardiac anomalies and require ECMO pre-operatively. In-hospital mortality among patients with conjugated hyperbilirubinemia was increased compared to those without (odds ratio 5.4). Post-operative complications including mechanical circulatory support, reoperation, prolonged ventilator dependence, and multi-system organ failure were more common with conjugated hyperbilirubinemia (all p < 0.04). Patients with higher levels of conjugated bilirubin had worst intermediate-term survival, with patients in the highest conjugated bilirubin group (>10 mg/dL) having a 1-year survival of only 6%.
Conclusions:Conjugated hyperbilirubinemia is associated with post-operative complications and worse survival following neonatal heart surgery. Cholestasis is more common in patients with chromosomal abnormalities and non-cardiac anomalies, but the underlying mechanisms have not been delineated.
Current practices for refractory chylothorax following congenital heart surgery
- Gregory T. Adamson, Melissa M. Winder, Kirsti G. Catton, Aaron G. Dewitt, Benjamin W. Kozyak, Emilee T. Glenn, David K. Bailly
-
- Published online by Cambridge University Press:
- 11 December 2023, pp. 1-5
-
- Article
-
- You have access Access
- Open access
- HTML
- Export citation
-
Introduction:
Chylothorax following paediatric cardiac surgery is associated with significant morbidity, particularly those that are refractory to conservative therapy. It is our impression that there is important variability in the medical, surgical, and interventional therapies used to manage refractory chylothorax between congenital heart programmes. We therefore conducted a survey study of current practices for managing refractory chylothorax.
Methods:The Chylothorax Work Group, formed with the support of the Pediatric Cardiac Critical Care Consortium, designed this multi-centre survey study with a focus on the timing and indication for utilising known therapies for refractory chylothorax. The survey was sent to one chylothorax expert from each Work Group centre, and results were summarised and reported as the frequency of given responses.
Results:Of the 20 centres invited to participate, 17 (85%) submitted complete responses. Octreotide (13/17, 76%) and sildenafil (8/17, 47%) were the most utilised medications. Presently, 9 (53%) centres perform pleurodesis, 15 (88%) perform surgical thoracic duct ligation, 8 (47%) perform percutaneous lymphatic interventions, 6 (35%) utilise thoracic duct decompression procedures, and 3 (18%) perform pleuroperitoneal shunts. Diagnostic lymphatic imaging is performed prior to surgical thoracic duct ligation in only 7 of the 15 (47%) centres that perform the procedure. Respondents identified barriers to referring and transporting patients to centres with expertise in lymphatic interventions.
Conclusions:There is variability in the treatment of refractory post-operative chylothorax across a large group of academic heart centres. Few surveyed heart centres have replaced surgical thoracic duct ligation or pleurodesis with image-guided selective lymphatic interventions.
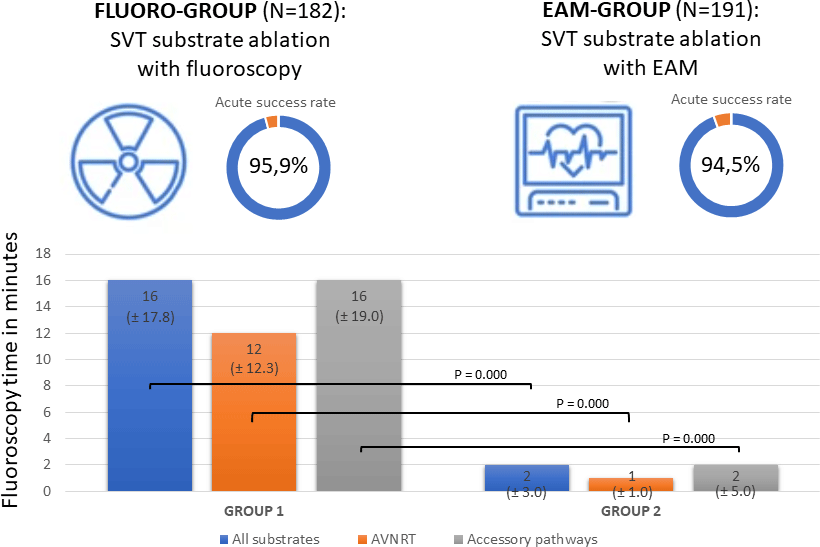
The effect of electro-anatomical mapping on the success rate and fluoroscopy time in supra-ventricular tachycardia ablation in children: single centre retrospective study
- Robin A. Bertels, Maud W. Françoijs, Catharina W. Averdieck, Janneke A.E. Kammeraad, Luc H. Filippini, Charlotte C.A. de Kezel, Stefan Frerich, Zina Fejzic, Frederik A. du Plessis, Lucas A.J. Rammeloo, Irene M. Kuipers, Nico A. Blom
-
- Published online by Cambridge University Press:
- 11 December 2023, pp. 1-6
-
- Article
-
- You have access Access
- Open access
- HTML
- Export citation
-
Aims:
To evaluate the effect of electro-anatomical mapping on success rate and fluoroscopy time in ablation of supraventricular tachycardia substrates in a large group of children.
Methods:Patients referred from multiple centres in the Netherlands and who received a first ablation for supraventricular tachycardia substrates in the Leiden University Medical Center between 2014 and 2020 were included in this retrospective cohort study. They were divided in procedures in patients with fluoroscopy and procedures in patients using electro-anatomical mapping.
Results:Outcomes of ablation of 373 electro-anatomical substrates were analysed. Acute success rate in the fluoro-group (n = 170) was 95.9% compared to 94.5% in the electro-anatomical mapping group (n = 181) (p = 0.539); recurrence rate was 6.1% in the fluoro-group and 6.4% in the electro-anatomical mapping group (p = 0.911) after a 12-months follow-up. Redo-ablations were performed in 12 cases in the fluoro-group and 10 cases in the electro-anatomical mapping group, with a success rate of 83.3% versus 80.0%, resulting in an overall success rate of 95.9% in the fluoro-group and 92.8% in the electro-anatomical mapping group (p = 0.216) after 12 months. Fluoroscopy time and dose area product decreased significantly from 16.00 ± 17.75 minutes (median ± interquartile range) to 2.00 ± 3.00 minutes (p = 0.000) and 210.5 µGym2 ± 249.3 to 32.9 µGym2 ± 78.6 (p = 0.000), respectively. In the fluoro-group, four complications occurred (2.0%) and in the electro-anatomical mapping group no complications occurred.
Conclusion:These results demonstrate that ablations of supraventricular tachycardia substrates in children remain a highly effective and safe treatment after the introduction of electro-anatomical mapping as a standard of care, while significantly reducing fluoroscopy time and dose area product.
Evaluation of quality of life and parental attitudes in patients who underwent atrial septal defect closure in childhood
- Zeynep Torunoğlu Bek, A. Deniz Oğuz, A. Şebnem Soysal Acar, Semiha Terlemez, Fatma Hayvacı Canbeyli, Serdar Kula, Fatma Sedef Tunaoğlu
-
- Published online by Cambridge University Press:
- 11 December 2023, pp. 1-6
-
- Article
- Export citation
-
Objective:
In this study, we aimed to evaluate quality of life and parental attitudes in children who underwent an atrial septal defect closure procedure with a transcatheter or surgical method in childhood and whether they continued their lives with similar activities to their healthy peers by comparing the two groups.
Methods:Patient forms to define sociodemographic and clinical features, the Questionnaire for Measuring Health-Related Quality of Life in Children and Adolescents (KINDL) to measure the quality of life of children, and the Parent-Child Relationship Test (Parental Attitude Research Instrument) to measure parental attitudes were used.
Results:The groups were similar in terms of age and sex. The mean quality of life scale scores were high in all groups, and there was no statistically significant difference between the scores. Parents of the patients who underwent closure received higher scores from the demographic attitudes and recognition of quality subdimension compared to the parents of the healthy group.
Conclusions:The quality of life of children with atrial septal defect closure was found to be similar to their healthy peers. Additionally, the effects of surgical or percutaneous closure of atrial septal defect on quality of life are similar. Children with atrial septal defect closure perceive their health status as well as their healthy peers, and this perception does not cause any difference in the attitudes and behaviours of families.
The impact of physical activity changes on exercise capacity and health-related quality of life in young patients with CHD: a 3-year follow-up study
- Hyun Jeong Kim, Ja-kyoung Yoon, Min Jeong Cho, Setor K. Kunutsor, Seong-Ho Kim, Sae Young Jae
-
- Published online by Cambridge University Press:
- 11 December 2023, pp. 1-8
-
- Article
- Export citation
-
Objective:
This study examined the relationship between changes in physical activity and their impact on exercise capacity and health-related quality of life over a 3-year span in patients with CHD.
Methods:We evaluated 99 young patients with CHD, aged 13–18 years at the outset. Physical activity, health-related quality of life, and exercise capacity were assessed via questionnaires and peak oxygen uptake measurements at baseline and after 3 years; changes in measures were estimated between the two time points and categorised into quartiles. Participants were stratified according to achieved (active) or not-achieved (inactive) recommended levels of physical activity (≥150 minutes/week) at both time points.
Results:Despite increases in physical activity, exercise capacity, and health-related quality of life over 3 years, the changes were not statistically significant (all p > 0.05). However, a positive association was found between physical activity changes and exercise capacity (ß = 0.250, p = 0.040) and health-related quality of life improvements (ß = 0.380, p < 0.001). Those with the most pronounced physical activity increase showed notable exercise capacity (p < 0.001) and health-related quality of life increases (p < 0.001) compared with patients with the largest decline in physical activity. The active-inactive category demonstrated a notable decline in exercise capacity compared to the active-active group, while the inactive-active group showed health-related quality of life improvements.
Conclusions:Over 3 years, increased physical activity was consistently linked to increases in exercise capacity and health-related quality of life in patients with CHD, highlighting the potential of physical activity augmentation as an intervention strategy.
Experiences of fetal care, social support, and emotional functioning during the COVID-19 pandemic in women carrying a fetus with CHD
- Priya Nigam, Colette Gramszlo, Shubhika Srivastava, Erica Sood
-
- Published online by Cambridge University Press:
- 07 December 2023, pp. 1-7
-
- Article
- Export citation
-
Objective:
To explore how the COVID-19 pandemic affected fetal care, social support, and emotional functioning for women carrying a fetus with CHD.
Method:This was a single-centre qualitative study of 31 women who received a prenatal diagnosis of CHD during the pandemic. Patients completed semi-structured interviews about their experiences with fetal care, social support, and perceptions of risk to themselves and their fetus. Consistent themes regarding the impact of the pandemic were identified using an inductive thematic approach. Demographic data were collected via self-report and chart review.
Results:Women generally reported consistent access to fetal care throughout the pandemic, with frequent use of telemedicine in addition to in-person care, but negative impacts resulting from restrictions on family support at appointments. Limited access to social support overall and a loss of pregnancy traditions were described. Many women reported feeling isolated and experiencing worries and fears about COVID-19 but also noted feeling supported by their healthcare team. Partner/family support during appointments and connection to peer-to-peer support were identified as recommendations to mitigate negative impacts.
Conclusion:Women carrying a fetus with CHD during the COVID-19 pandemic experienced unique stressors that may affect mental health. However, many also experienced unexpected supports that may mitigate effects of pandemic-related stressors. Results can inform efforts to promote positive family outcomes during and following the COVID-19 pandemic.
Prevalence of anxiety and depression in adult patients with CHD
- Reza Keshavarzi, Parisa Divsalar, Maryam Aliramezany
-
- Published online by Cambridge University Press:
- 07 December 2023, pp. 1-6
-
- Article
- Export citation
-
Introduction:
CHD are among the most common congenital defects. Due to the chronic nature of CHD, patients face various risk factors that threaten their mental health. However, a comprehensive understanding of the medical and social predictors of mental health issues in adults with CHD is lacking. This study aims to investigate the prevalence of anxiety and depression in adults with CHD.
Methods:This cross-sectional descriptive study focused on adults with CHD in Kerman, Iran. The participants completed demographic information alongside two psychological assessment tools: the Beck Anxiety Inventory (BAI) and the Depression Anxiety Stress Scales (DASS)-21. The data were analyzed using SPSS 26.
Findings:The mean age of the participants was 29.94 ± 12.36 years, and 63.8% were female. According to the DASS, 73.4% did not have depression, 61% did not have anxiety, and 76.2% did not have stress. In total, 19% had mild stress, and 4.8% had moderate stress. According to the BAI, 27.6% did not have anxiety. Individual characteristics were not significantly associated with depression. However, gender, age, and type of surgery were significantly associated with anxiety. Cyanosis was significantly associated with stress.
Conclusion:The results show that mental disorders like depression, anxiety, and stress are highly prevalent in adults with CHD. The prevalence depends on individual factors such as age, gender, and disease severity. Therefore, it is recommended that mental disorders in this population be evaluated and treated accurately.
A descriptive assessment of the informed consent document used by congenital cardiac surgery centres
- Kristal M. Hock, Katja Gist, Pariya L. Fazeli, Hayden J. Zaccagni, Robert A. Sorabella, Patricia A. Patrician
-
- Published online by Cambridge University Press:
- 04 December 2023, pp. 1-6
-
- Article
- Export citation
-
Background:
Informed consent for surgery is a complex process particularly in paediatrics. Complexity increases with procedures such as CHD surgery. Regulatory agencies outline informed consent contents for surgery. We assessed and described CHD surgical informed consent contents through survey dissemination to paediatric CHD centres across United States of America.
Methods:Publicly available email addresses for 125 paediatric cardiac clinicians at 70 CHD surgical centres were obtained. Nine-item de-identified survey assessing adherence to The Joint Commission informed consent standards was created and distributed via RedCap® 14 March, 2023. A follow-up email was sent 29 March, 2023. Survey link was closed 18 April, 2023.
Results:Thirty-seven surveys were completed. Results showed informed consent documents were available in both paper (25, 68%) and electronic (3, 8%) format. When both (9, 24%) formats were available, decision on which format to use was based on centre protocols (1, 11%), clinician personal preference (3, 33%), procedure being performed (1, 11%), or other (4, 45%). Five (13%) centres’ informed consent documents were available only in English, with 32 (87%) centres also having a Spanish version. Review of informed consent documents demonstrated missing The Joint Commission elements including procedure specific risks, benefits, treatment alternatives, and expected outcomes.
Conclusions:Informed consent for CHD surgery is a complex process with multiple factors involved. Majority of paediatric CHD surgical centres in the United States of America used a generic informed consent document which did not uniformly contain The Joint Commission specified information nor reflect time spent in discussion with families. Further research is needed on parental comprehension during the informed consent process.
Experience of left ventricular outflow tract arrhythmia ablation in paediatric patients using limited fluoroscopy and three-dimensional mapping technique
- Şevket Ballı, Pınar Kanlıoğlu, Gokmen Akgun
-
- Published online by Cambridge University Press:
- 01 December 2023, pp. 1-6
-
- Article
- Export citation
-
Objective:
The left ventricular outflow tract is an important source of ventricular arrhythmias. Up to one-third of all idiopathic ventricular arrhythmias in patients with structurally normal hearts may arise from this region. We would like to share the results of our left ventricular outflow tract ablation using three-dimensional mapping and limited fluoroscopy.
Materials and Methods:This is a single-centre retrospective cohort study. Forty-six consecutive patients who underwent left ventricular outflow tract ablation procedures between January 2015 and June 2023 were included in the study. The EnSite Precision System (Abbott, St. Paul, MN, USA) was used to facilitate mapping and to reduce or eliminate the need for fluoroscopy.
Results:The study group comprised 29 males and 17 females, with a mean age of 13.4 ± 4.5 years. The most common location for arrhythmias was the left coronary cusp (n : 21). Other locations, in sequence, included the junction of the right and left coronary commissure (n : 10), right coronary cusp (n : 10), left ventricular outflow tract endocardium (n:4), aorto-mitral junction (n : 1), and great cardiac vein (n : 1). Nine of these patients had previously undergone unsuccessful right ventricular outflow tract ablation at another centre. Cryoablation was performed in three patients, irrigated radiofrequency ablation in three patients, and conventional radiofrequency ablation in the remaining patients. The acute success rate was 100%, and no recurrences were observed. The mean follow-up period was 49.6 ± 24.4 months. All patients were asymptomatic and were being followed without antiarrhythmic medication.
Conclusion:Although left ventricular outflow tract ablations pose a risk for coronary artery and heart valve complications, they can be performed successfully and safely with the guidance of three-dimensional mapping.
Intraoperative transit-time flow measurement of caval veins before and after bidirectional cavopulmonary anastomosis
- Sara C. Arrigoni, Joost M. A. A. van der Maaten, Marc T. R. Roofthooft, Roland F. Hoffmann, Rolf M. F. Berger, Tjark Ebels
-
- Published online by Cambridge University Press:
- 01 December 2023, pp. 1-7
-
- Article
-
- You have access Access
- Open access
- HTML
- Export citation
-
Background:
Haemodynamic changes in caval venous flow distribution occurring during bidirectional cavopulmonary anastomosis operation are still largely unknown.
Methods:Transit time flow measurements were performed in 15 cavopulmonary anastomosis operations. Superior and inferior caval vein flows were measured before and after the cavopulmonary anastomosis. Ratio of superior caval vein to overall caval veins flow was calculated.
Results:Mean superior caval vein flow ratio before cavopulmonary anastomosis was higher than previously reported for healthy children. Superior caval vein flow ratio decreased in 14/15 patients after cavopulmonary anastomosis: mean 0.63 ± 0.12 before versus 0.43 ± 0.14 after. No linear correlation between intraoperative superior caval vein pressure and superior caval vein flow after cavopulmonary anastomosis was found. Neither Nakata index nor pulmonary vascular resistance measured at preoperative cardiac catheterisation correlated with intraoperative flows. None of patients died or required a take down.
Conclusions:The higher mean superior caval vein flow ratio before cavopulmonary anastomosis compared to healthy children suggests flow redistribution in univentricular physiology to protect brain and neurodevelopment. The decrease of superior caval vein flow ratio after cavopulmonary anastomosis may reflect the flow redistribution related to trans-pulmonary gradient. The lack of correlation between superior caval vein pressure and superior caval vein flow could be explained by limited sample size and multifactorial determinants of caval veins flow, although pressure remain essential. Larger sample of measurements are needed to find flow range potentially predictive for clinical failure. To authors’ knowledge, this is the first intraoperative flow measurement of both caval veins during cavopulmonary operations.
Neurocognitive function and health-related quality of life in adolescents and young adults with CHD with pulmonary valve dysfunction
- Jeffrey D. Zampi, Kimberley P. Heinrich, Lisa Bergersen, Bryan H. Goldstein, Sarosh P. Batlivala, Stephanie Fuller, Andrew C. Glatz, Michael L. O’Byrne, Bradley Marino, Katherine Afton, Ray Lowery, Sunkyung Yu, Caren S. Goldberg
-
- Published online by Cambridge University Press:
- 30 November 2023, pp. 1-8
-
- Article
-
- You have access Access
- Open access
- HTML
- Export citation
-
Background:
Neurocognitive impairment and quality of life are two important long-term challenges for patients with complex CHD. The impact of re-interventions during adolescence and young adulthood on neurocognition and quality of life is not well understood.
Methods:In this prospective longitudinal multi-institutional study, patients 13–30 years old with severe CHD referred for surgical or transcatheter pulmonary valve replacement were enrolled. Clinical characteristics were collected, and executive function and quality of life were assessed prior to the planned pulmonary re-intervention. These results were compared to normative data and were compared between treatment strategies.
Results:Among 68 patients enrolled from 2016 to 2020, a nearly equal proportion were referred for surgical and transcatheter pulmonary valve replacement (53% versus 47%). Tetralogy of Fallot was the most common diagnosis (59%) and pulmonary re-intervention indications included stenosis (25%), insufficiency (40%), and mixed disease (35%). There were no substantial differences between patients referred for surgical and transcatheter therapy. Executive functioning deficits were evident in 19–31% of patients and quality of life was universally lower compared to normative sample data. However, measures of executive function and quality of life did not differ between the surgical and transcatheter patients.
Conclusion:In this patient group, impairments in neurocognitive function and quality of life are common and can be significant. Given similar baseline characteristics, comparing changes in neurocognitive outcomes and quality of life after surgical versus transcatheter pulmonary valve replacement will offer unique insights into how treatment approaches impact these important long-term patient outcomes.
Clinical and genetic characteristics of catecholaminergic polymorphic ventricular tachycardia combined with left ventricular non-compaction
- Bihe Xu, Jing Yang, Fang Liu, Tingting Lv, Kun Li, Yifang Yuan, Siyuan Li, Yuanwei Liu, Ping Zhang
-
- Published online by Cambridge University Press:
- 29 November 2023, pp. 1-8
-
- Article
- Export citation
-
Background:
Catecholaminergic polymorphic ventricular tachycardia is an ion channelopathy, caused by mutations in genes coding for calcium-handling proteins. It can coexist with left ventricular non-compaction. We aim to investigate the clinical and genetic characteristics of this co-phenotype.
Methods:Medical records of 24 patients diagnosed with catecholaminergic polymorphic ventricular tachycardia in two Chinese hospitals between September, 2005, and January, 2020, were retrospectively reviewed. We evaluated their clinical and genetic characteristics, including basic demographic data, electrocardiogram parameters, medications and survival during follow-up, and their gene mutations. We did structural analysis for a novel variant ryanodine receptor 2-E4005V.
Results:The patients included 19 with catecholaminergic polymorphic ventricular tachycardia mono-phenotype and 5 catecholaminergic polymorphic ventricular tachycardia-left ventricular non-compaction overlap patients. The median age of onset symptoms was 9.0 (8.0,13.5) years. Most patients (91.7%) had cardiac symptoms, and 50% had a family history of syncope. Overlap patients had lower peak heart rate and threshold heart rate for ventricular tachycardia and ventricular premature beat during the exercise stress test (p < 0.05). Sudden cardiac death risk may be higher in overlap patients during follow-up. Gene sequencing revealed 1 novel ryanodine receptor 2 missense mutation E4005V and 1 mutation previously unreported in catecholaminergic polymorphic ventricular tachycardia, but no left ventricular non-compaction-causing mutations were observed. In-silico analysis showed the novel mutation E4005V broke down the interaction between two charged residues.
Conclusions:Catecholaminergic polymorphic ventricular tachycardia overlapping with left ventricular non-compaction may lead to ventricular premature beat/ventricular tachycardia during exercise stress test at lower threshold heart rate than catecholaminergic polymorphic ventricular tachycardia alone; it may also indicate a worse prognosis and requires strict follow-up. ryanodine receptor 2 mutations disrupted interactions between residues and may interfere the function of ryanodine receptor 2.