Introduction
Human-induced climate change is increasing the likelihood of fire weather (periods of weather conditions comprising a combination of high temperatures, low humidity, low rainfall, and often high winds). Reference Jones, Smith and Betts1 Evidence indicates that the frequency, intensity, and duration of wildfires is increasing globally. Reference Dutta, Das and Aryal2,Reference Borchers Arriagada, Bowman and Palmer3 Australia has always experienced wildfires (which will be referred to in this paper by the Australian terminology “bushfires”). However, longer, hotter, and more intense heatwaves along with droughts of increasing frequency and severity have contributed to a very high risk of bushfires, particularly in the southeast and southwest. Reference Hughes and Fenwick4 The increased frequency, intensity, and duration of bushfires in Australia due to climate change and the increasing pressures on Australia’s firefighting resources to contain these fires has implications for the health of the Australian population. Reference Hanna and McIver5,Reference FitzGerald, Capon and Aitken6
Wildfires have negative health consequences for affected communities. Wildfires directly impact population health through respiratory illness from air pollution, Reference Borchers Arriagada, Bowman and Palmer3,Reference Hanna and McIver5-Reference Zara, Parkinson and Duncan10 and injuries and burns, Reference Hanna and McIver5 as well as indirect impacts such as exacerbation of existing chronic conditions, and chronic mental health effects due to loss and grief, and sometimes guilt. Reference Zara, Parkinson and Duncan10 The loss of health systems’ infrastructure and disrupted health services causing lack of access to on-going health care also has indirect negative impacts on population health. Reference FitzGerald, Capon and Aitken6 Pharmacists in Australia have been identified as the most easily accessible health care professional and are more accessible to the community than supermarkets, banks, or medical centres. 11 As such, community pharmacies are a central hub between patients and the health care system and are uniquely placed to provide continuity of care during natural disasters, including bushfires. Reference Watson, Singleton and Tippett12 For example, the Final Report of the Victorian Government Inspector-General for Emergency Management (IGEM; Melbourne, Victoria, Australia) on the thunderstorm asthma event of November 21-22, 2016 in Melbourne included a comment on the significant role that pharmacists had played:
IGEM finds that on 21-22 November 2016, community pharmacies played a central role in meeting community needs during the thunderstorm asthma event. Given their community focus and their geographic coverage, community pharmacists can provide valuable support to the management of health emergencies or emergencies with health impacts. 13, p.36
There have been numerous media reports of Australian community pharmacists continuing to operate their pharmacies during bushfire events, despite having no power or mobile phone service, or while their own homes were under threat or had burned down. These reports cover the Tasmanian bushfires of the 2018-2019 summer, Reference Haggan14-Reference Humphries16 as well as the recent bushfire crisis in Australia (June 2019 – March 2020). Reference Bain and Baker17,Reference Winkle and Neilson18 However, there is little in peer-reviewed literature about the impacts of bushfires on Australian community pharmacy operations. Therefore, the aim of this study was to explore the impacts of the 2018/2019 summer bushfires in Tasmania, Australia on community pharmacy operations in affected areas.
Methods
Study Design
This research utilized qualitative research methods to explore community pharmacists’ experiences and opinions of operating community pharmacies during a bushfire event. Semi-structured interviews were conducted with four community pharmacists in July 2019 who were working in community pharmacies impacted by the bushfire event that occurred in the summer of 2018-2019 in Tasmania, Australia. The interview questions were designed to explore pharmacists’ experiences before, during, and after the bushfire event. They were developed from an interview format used in previously published research exploring community pharmacists’ experiences of community pharmacy operations during a bushfire event. Reference Mak and Singleton19 Questions relating to the Prevention – Preparedness – Response – Recovery (PPRR) phases of the disaster management model were added to the previously developed interview format. Reference Rogers20 These additional questions aimed to explore community pharmacists’ actions across the PPRR continuum during the bushfire event.
Ethical approval was obtained from the Queensland University of Technology Human Research Ethics Committee (Brisbane, Queensland, Australia; Approval Number 1900000230) prior to conducting interviews. Purposive and snowball sampling methods were used to recruit participants. To be eligible for inclusion in this study, participants had to be a registered pharmacist with the Australian Health Practitioner Agency (AHPRA; Melbourne, Victoria, Australia) and worked in Tasmania during the summer of 2018-2019 in a community pharmacy which was affected by the bushfire event. Potential community pharmacies were recruited by identifying bushfire-affected regions and then cold calling community pharmacies in these areas to assess eligibility and willingness to participate in the study. These bushfires impacted four small regional pharmacies. All four pharmacies had pharmacist owner-managers who met the eligibility criteria. They were asked if they were interested in participating and provided with a participant information sheet and a written consent form. To ensure participant confidentiality, each participant was assigned a unique ID code before the interview commenced. The interview was audio recorded and the audio files transcribed verbatim using a professional transcription service.
Data Analysis
The interview transcript qualitative data were analyzed by two different methods to provide triangulation of methods. First, the data were coded manually, and secondly, the data were analyzed using the text analytics tool, Leximancer Version 4 (Leximancer Pty Ltd; Brisbane, Australia).
Manual Coding Analysis
NVivo Version 11 software (QSR International; Doncaster, Victoria, Australia) was used for the manual coding process with data coded into codes, categories, and themes using open and axial coding methods as described by Saldaña. Reference Saldana21 To ensure inter-rater reliability, two researchers coded the data independently. Differences in coding were discussed by the team as a whole and agreement reached through discussion and negotiation.
Leximancer Analysis
Leximancer analyzes text by converting lexical co-occurrence information from natural language into semantic patterns in an automated manner: 22
It employs two stages of co-occurrence information extraction – semantic and relational – using a different algorithm for each stage. The algorithms used are statistical, but they employ non-linear dynamics and machine learning. Reference Smith and Humphreys23, p.262
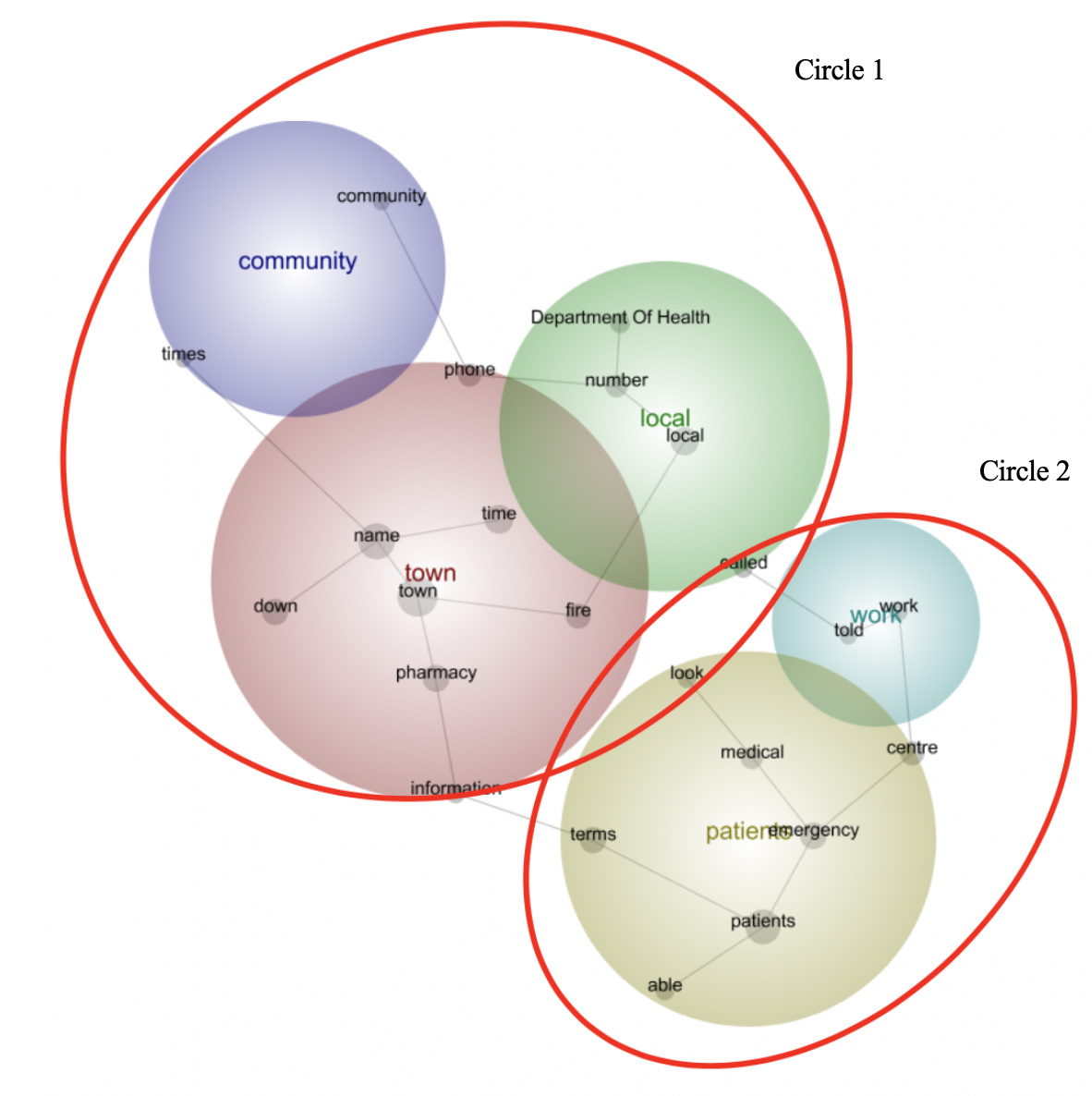
Leximancer was used to analyze the content of the text and display the extracted information visually as a concept map. Reference Smith and Humphreys23 Rather than analyzing the data for each question separately, the four interviews’ transcripts were analyzed together in their entirety. Concepts in Leximancer are collections of words that generally appear together throughout the text. The concept map provides a bird’s eye view of the data, depicting the main concepts and how they interrelate. Concepts that appear often together in the text are clustered together into themes that are heat mapped - the hotter the color, the more important the theme, with red being the hottest, then orange, and so on as per the color wheel. Thus, Leximancer provides a means of quantifying and displaying the conceptual structure of the text, enabling an exploration of relationships between the identified concepts. Reference Smith and Humphreys23 The entire process was run several times to check that the relative positioning of the concepts was similar between iterations. This confirmed that the concept map is representative of the data set.
Results
References were made by participants to two pharmacy organizations – the Pharmacy Guild of Australia (PGA; Canberra, Australia) and the Pharmaceutical Society of Australia (PSA; Deakin, Australian Capital Territory, Australia). These two professional organizations differ in their membership. The PGA’s members comprise solely of pharmacy owners, whereas the PSA offers membership to all pharmacists.
The concept map for the Leximancer analysis was recorded at theme size 52% with visual concepts set at 100%. The themes in the concept map in order of importance (hottest color to coolest color) were: town; patients; local; work; and community (Supplementary Material; available online only). These aligned with the five themes that emerged from the manual coding analysis (Figure 1) – communication and collaboration; support; patient health challenges; pharmacist experiences in delivering health care; and future planning. The Leximancer themes community, town, and local refer to the integration of community pharmacies as a key local health care resource and align with the manual coding themes of communication and collaboration and support. The Leximancer themes of patients and work align with the manual coding themes of patient health challenges, pharmacist experiences in delivering health care, and future planning and reflect the impact of bushfires on the continuity of pharmacy operations.

Figure 1. Manual Coding Analysis of Interview Data.
Communication and Collaboration
Communication was a key issue identified by the participants. It was often conducted through informal channels, such as social media, and was important for disaster response. Participants highlighted the lack of communication or disjointed lines of communication at all levels with one participant revealing they became a communication conduit:
I just told people through Facebook … that I was here and that if they didn’t need any medical attention but just medication, that I was open. I actually ended up being the liaison between the Department of Health and the local fire service. It was just a comedy of errors where, for example, a number that I’d been given from the Department to hand over to the local fire chief that he tried to ring, it didn’t work. So, he then rings me to try and find the right number but when I called the Department of Health, they’re not allowed to hand out any numbers, which I understand. I ended up being the go-between for different things, which was quite stressful because I was not an official person on - like we’re not part of any disaster plan. [E022; unique participant ID code]
I was using the ABC [Australian Broadcasting Commission] website that was talking about the bushfire, had the warnings, but the warnings were very generic and really didn’t mean anything. It was essentially the highest level of emergency, so essentially evacuate. Emergency personnel, you’d sort of get little titbits here and there and there were lots of rumors flying around, so other people who had stayed, they had family in the fire service, they were getting all sorts of weird information and yeah, it was horrible. We just didn’t know what was going on. [H182]
That was one of my gripes, that we had no heads up as who to talk to, you know, more direct managerial sort of sense. [B152]
Pharmacists were left out of planning discussions, even when potential decisions would impact them and their pharmacy operations:
We’ll [Department of Health] go and have a meeting and we’ll decide what we think you’ll need and we’ll send it to you. I said, well okay, that’s interesting. I didn’t understand how they were going to ascertain how much was needed, having information that an unknown population [those evacuated] was moving down potentially to us. [E022]
Support
This theme describes the sense of duty of care demonstrated by pharmacists during this event through staying open and minimizing interruptions to pharmacy operations in order to continue supporting their community:
As far as actually doing the job, we’ll do the job because that’s what we’re here for. We manage in times of stress and getting people things. [B152]
Well for my community, that was probably the most important thing. It was about just being there and there was still quite a few people left behind, and because there were no medical services, the doctors were closed for two weeks, so the local GP [General Practitioner] wasn’t there, … it was mainly just bringing the psychological support, because a lot of people were really stressed, … just being there for the community as well. [H182]
This theme also encompassed participants’ comments about the support they received to help them maintain their pharmacy operations. They received support from their local council and the Tasmanian branches of the PGA and the PSA rather than from the Tasmanian Department of Health:
The Pharmaceutical Society [PSA] and also the Guild [PGA], they called me and asked if I was okay and asked if I needed any help just to let them know. [B143]
The Guild [PGA] was quite proactive. I think the PSA followed it along a little bit when they realized how serious it was and actually how stressful it was. We were all going above and beyond. [B152]
So PSA, the TGA [Therapeutic Good Administration], and the wholesalers were fantastic and the local council. I didn’t get that much help from the Department of Health. The Department got in touch with me quite early and called me on the day before the emergency, they said, the fires starting and we’re just going through our chains and looking at the health care service provisions, are you prepared? I said, well yes, I’m prepared… We’re kind of ready. They said, well we’re not just talking about tomorrow and… I said, okay … How long are you thinking? She said, well we can’t say and I said, well okay I can’t answer your question then. We sort of argued like this back and forth and in the end the person said, well for my reporting purposes, are you prepared? I then said well, you’re going to have to tick a maybe box, because I just don’t know how long we now are looking at. [E022]
However, one pharmacy did report the Department of Health had supplied them with a generator:
The generator was supplied by the Health Department, but it looks like it’ll be something I’ll be getting later on…. It was about five days after the bushfires started it was supplied. [H182]
The participants also reported that they would have liked support in the form of pharmacist locum relief (free of charge) both during the event and in the aftermath to help them cope with the stress arising from the increased workload of managing either increased patient numbers due to other pharmacies having to close, and/or operating on their own or with reduced staff during the event:
What would have nice would have been two weeks with a pharmacist for free, no charge. That wasn’t going to happen. It was I think the PSA was… [said] oh we may be able to send XX or whoever. [B152]
Patient Health Challenges
This theme refers to the challenges experienced by patients who required health care during the bushfire. The biggest health challenges appeared to be experienced by people evacuated to a crisis center:
It was about the third or the fourth day of the emergency when the center organizers, at that stage they still hadn’t organized a medical officer, a management officer of the medications. They had St John’s there and they had a GP [general practitioner] there and there was loads of liaising between the two and the local pharmacies as such, we’re the local pharmacy. I’d given my phone number because we’d had a couple of requests from the council to send some Ventolin and spacers and look after people who’d had issues or out fighting the fires. I remember we gave them something to help this person who was fighting the fires with their gastro issue … I’d get the phone call saying look, so-and-so’s just rocked up and they don’t have this, that or the other, can you help them? …. I’d go and find out what they needed and sort it out and get it to them. [B152]
The community also suffered health effects from the smoke:
They had an air quality warning out. Anybody who had heart issues or breathing issues they were … recommended to leave the area. It was indirect because of the bush fires. That was another load that we had to deal with but it wasn’t fire as such, it was just the smoke. We’re still dealing now with people who have lung issues that can pin it down to the bush fires…… our Ventolin sales doubled at least, probably even quadrupled at some stages of the [disaster] period. [B152]
Pharmacists’ Experiences Delivering Health Care
Pharmacists reported numerous challenges in maintaining medication supplies to their community. Reduced staff numbers, logistic challenges due to roads being cut off, and lack of medical support were reported. Three of the participants commented that constantly needing to speak to people on the phone put them under pressure to complete routine tasks, particularly with reduced staff numbers and only one pharmacist:
We were too busy selling Ventolin, managing breathing issues, liaising with doctors to get people to see their doctors. Yes, normal things really were popped to the back of the list of day-to-day necessities really. [B152]
The number of patients were greatly reduced that were physically present within the pharmacy but the number of phone calls from other health providers and patients who had evacuated was exponentially - I was always on the phone. It was … the hardest part of the whole thing, really, was trying to do everything and be on the phone for the entire eight hours. [H182]
Pharmacy deliveries of medications from wholesalers experienced delays, which added stress to pharmacy staff:
The Department of Health didn’t help us with deliveries. The local council did because they … understood that they had to get groceries in and medication. We kept going for about six or seven days, I think, until we got the first delivery. So, we ran low, but we managed to work around it until we got the first delivery and that was escorted in by police. [E022]
The participants acknowledged the need to ensure that patients’ medication supplies were not interrupted while considering the impacts of the fires on the pharmacy staff personally and on the safety of the pharmacy work environment:
Well they [staff] wanted to come in and I said, no. They wouldn’t have been able to come in anyway because the roads were blocked with the only entry into that region. I told them not to come to work. As it went by and the restrictions were less severe, so locals were then allowed back in, then my staff did start coming back, but that was after about five or six days. [H182]
Well, we would all turn up to work as needed but we were extremely busy. Each day I’d allow time to go and call around to the … crisis center where all the people who’d been evacuated were sent. Make sure somebody had my phone number. If they needed anything I could come back into the pharmacy and get it for them and take it back around. [B152]
Pharmacists also described difficulties in supplying medications to patients who presented to the pharmacy without prescriptions. At that time, pharmacists could legally only supply three days’ worth of medication or a single unit, such as one bottle of eye drops, to bushfire-affected patients:
I supplied two lots of eye drops to her and I’ll never see a script for them. She needed to have them so I think, oh my gosh, technically I would be in trouble. I had to use my discretion and judgment at the time. There’s no allowance for that in the Pharmacy Act. We did “owings” and we had people who needed packs made up like dosing medication packs. We just did a lot of contacting with prescribers or surgeries, sometimes with pharmacies just to see what the correct medications were. I think we mostly got scripts back for everything except for one person, maybe one or two people. [B152]
From a medico-legal perspective, it was probably one of my biggest issues, because there were no prescribing doctors, patients couldn’t leave the area and it was two weeks before the medical profession would actually be physically there. So, I was asked incessantly …like their blood pressure, cholesterol, antidepressants. … At times it was antibiotics … I have a good relationship with the local doctor and she said that she’d cover anything that I thought was needed. There were a few occasions there where I had to really step outside of the bounds of legislation and pretty much broke the law because if you’re the A-type personality, the law is the law, I wouldn’t have been able to help these people and they probably would have had to be airlifted to hospital. [H182]
Future Planning
All four participants commented that community pharmacy should be included in future disaster management planning, highlighting that community pharmacies are ideally positioned to act as a central hub for information dissemination. Involvement would also highlight remuneration issues to the government:
Evacuated from their house and had to leave their medication and then they’ve got to go and purchase it again. We ended up bearing the brunt of that angst quite often. That was disheartening because we’re just trying to do the right thing and help people, and here we were the baddies making money. Whereas in a perfect world, there’d be some sort of allowance from the government for medications … to be provided at no charge. [B152]
Yes, I think we need to be part of the official disaster planning…so if something happens down here and I call up the Department of Health, then I am somebody that if I do need help, or I need to get in touch with somebody that is, they know that I am an okay person to hand out a phone number or to relay information. [E022]
Discussion
This research clearly demonstrates that during the Tasmanian bushfires in the summer of 2018-2019, the pharmacists in the bushfire-affected communities continued to work under stressful conditions to support their communities, ensure continuity of medication supply, and handle minor ailments. Participants described their work environments at this time as difficult, facing numerous challenges such as communication difficulties, including lack of up-to-date information on the bushfires themselves, legislation barriers, logistical issues, lack of preparation, lack of inclusion in disaster management planning, and lack of tangible support including remuneration from government bodies such as the Tasmanian government’s Department of Health. Fragmented care was reported, particularly for those evacuated and staying in crisis centers. Much of the stresses on community pharmacists during these events could be reduced if primary care practitioners (GPs and pharmacists) were included in disaster management planning and in communication channels prior to, and during, disasters. This corroborates the findings of a previous study on the impacts to community pharmacy services of the Tasmanian 2012/2013 summer bushfires, Reference Mak and Singleton19 as well as the findings of Burns, et al Reference Burns, Douglas and Hu24 who argued for improved incorporation of primary care in disaster management planning. Research has also highlighted that pharmacists are able to fulfil a number of roles during disasters Reference Watson, Singleton and Tippett12,Reference Watson, Singleton and Tippett25 and would most likely report to work during a disaster because they believe their pharmacy provides an essential service to their community. Reference McCourt, Watson and Singleton26
Following disasters, Australians will seek medical assistance from local GP practices, community pharmacies, and public hospitals. Reference Burns, Douglas and Hu24 Immediately following a disaster, both pharmacists Reference Mak and Singleton19 and GPs Reference Burns, Douglas and Hu24 have reported being inundated with patients seeking medical assistance or medication supplies. Pharmacists and GPs play an important role in helping the community in the recovery phase, which will continue long after first responders and the media have left. Reference Burns, Douglas and Hu24 To help primary care health care providers support their communities before, during, and after disasters and to reduce instances of fragmented care, there needs to be increased inclusion of the primary health sector in disaster management planning. Reference Burns, Douglas and Hu24 Improved preparation for future bushfire events therefore requires a systems thinking approach involving all stakeholders in the health system (including GPs and pharmacists) across the PPRR continuum. Reference FitzGerald, Capon and Aitken6
During these bushfires, pharmacists faced legislative barriers and ethical and moral dilemmas regarding the number of days emergency supply of medication they could provide without a prescription. These legislative issues were also reported in a study looking at the impacts of the Tasmanian bushfires in the summer of 2012-2013 on community pharmacy operations. Reference Mak and Singleton19 With the increasing number of disasters, the PGA and the PSA have lobbied the Australian government to change the arrangements for the provision of medications without a prescription during disasters. As a response to the on-going Australian 2019-2020 bushfire crisis in New South Wales (NSW) and Queensland (Qld), the Federal Department of Health introduced a special authority to pharmacists for emergency supply of medications without a prescription in bushfire-affected areas. This allows pharmacists to provide continuing supply of a patient’s essential medication in the standard Pharmaceutical Benefits Scheme (PBS) quantity (usually one month’s supply). 27 It is expected that this temporary authority will reduce stress to both patients and pharmacists.
This research also highlighted the lack of financial reimbursement community pharmacy owners receive from the government to cover supplies of medications, toiletries, and other items for which they never received payment. Lack of payment was due to either patients presenting to the pharmacy with no means of paying, or pharmacists never receiving a prescription from the patient’s prescriber for an emergency supply of a PBS item and therefore unable to claim reimbursement from Medicare. This corroborates the findings of the study looking at the Tasmanian 2012-2013 summer bushfires. Reference Mak and Singleton19 Also, unlike other health care professionals, pharmacists are directly involved in financial transactions and are sometimes made to feel they are profiting from others’ misfortune. Future consideration could be given to an emergency funding pool to cover free resupplies of medication to bushfire-affected patients. This study also identified that pharmacists who worked during the disaster needed financial assistance to cover the hire of locum pharmacists during the disaster and/or in the aftermath to give them a much-needed rest.
Limitations
As with the previous Tasmanian bushfire study, this study also had a small sample size of four pharmacists due to the localized area of these bushfires.
Conclusions
Community pharmacists play an important role in disasters. However, they need support to carry out this role across the entire PPRR continuum. It requires support through improved communication by including them in disaster management planning, and financial support to cover costs of supply to patients who have no money, costs for supplies on owed prescriptions which are never provided, and to cover costs to hire locum pharmacists to help during and in the aftermath. Including pharmacists in all government levels of disaster planning in Australia - local, state, and federal – will raise the issues identified in this research and help them to continue to support their communities.
Acknowledgements
The authors wish to thank the Tasmanian pharmacists who participated in this research for their generosity in taking the time to be interviewed.
Conflicts of interest/funding
All authors have declared there are no conflicts of interest. This project was funded by a pilot data seeding grant from QUT Institute of Health and Biomedical Innovation, Health Determinants, and Health Systems stream and an Advance Queensland Women’s Research Assistance Program grant.
Supplementary Material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1049023X20001077