
Contents
Research Report
Temporal Changes in Epinephrine Dosing in Out-of-Hospital Cardiac Arrest: A Review of EMS Protocols across the United States
-
- Published online by Cambridge University Press:
- 21 October 2022, pp. 832-835
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Original Research
A Market Review of Available Airway Suction Technology
-
- Published online by Cambridge University Press:
- 31 March 2022, pp. 390-396
-
- Article
- Export citation
Systematic Review
METASTART: A Systematic Review and Meta-Analysis of the Diagnostic Accuracy of the Simple Triage and Rapid Treatment (START) Algorithm for Disaster Triage
-
- Published online by Cambridge University Press:
- 17 December 2021, pp. 106-116
-
- Article
- Export citation
Meeting Abstracts
Establishing an Emergency Medical Team in LMIC Setup; Experience from Ethiopia’s Challenges and Opportunity
-
- Published online by Cambridge University Press:
- 22 November 2022, p. s67
-
- Article
-
- You have access
- Export citation
-
Background/Introduction:
Natural and man-made catastrophes have caused significant destruction and loss of lives throughout human history. Disasters accompany various events with multiple causes and consequences, often leading to a cascade of health-related events. Ethiopia, amongst the developing countries in the horn of Africa, is vulnerable to natural and man-made disasters. Over the last few years, Ethiopia learned the hardest way to transform its disaster management from a mere apparatus of response and recovery to preparedness and mitigation.
Objectives:Review the challenges and opportunities for establishing the Ethiopian EMT and its disaster response experience.
Method/Description:This was a mixed-methods, cross-sectional Intra-Action Review of activities of country EMT. It included a review of documents and key informant interviews. All data were analyzed thematically.
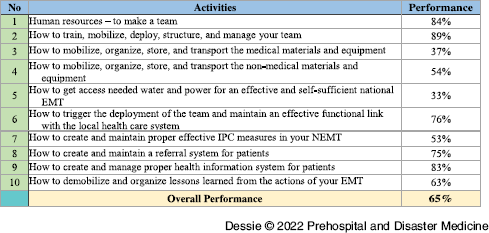
Results/Outcomes:In May 2022, the Ethiopian Federal MOH, in collaboration with WHO, adapted the WHO EMT initiative to tackle the identified challenges. Ethiopia’s EMT implementation plan was created, which included ten steps and 50 detailed activities. This initiative aims to have a classified Type I fixed EMT in the coming six months. Based on the objective evaluation of the last four months’ performance toward plan implementation, activities show that 65% of the overall plan has been completed.
Conclusion:Implementing the EMT initiative in Ethiopia has positively impacted the clinical quality of care, enhanced coordination, and improved health outcomes for the population served at times of great need. However, the implementation requires collaboration in support, guidance, and experience sharing from stakeholders and partners, including twinning with other organizations.
Tables and Figures (optional)
Table 1. Ethiopian EMT Ten Steps Implementation

Research Report
The Response by International Emergency Medical Teams Following the Beirut Harbor Explosion in 2020 – Who Were They, When Did They Arrive, What Did They Do, and Were They Needed?
-
- Published online by Cambridge University Press:
- 20 May 2022, pp. 529-534
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Systematic Review
The Use of Portable Oxygen Concentrators in Low-Resource Settings: A Systematic Review
- Part of:
-
- Published online by Cambridge University Press:
- 02 March 2022, pp. 247-254
-
- Article
- Export citation
Research Report
Medical Evacuation and Liquidation of the Medical-Sanitary Aftereffects in Crisis
-
- Published online by Cambridge University Press:
- 28 February 2022, pp. 255-258
-
- Article
- Export citation
Systematic Review
Emergency Preparedness and Disaster Response: There’s an App for That 2.0
-
- Published online by Cambridge University Press:
- 17 December 2021, pp. 117-123
-
- Article
- Export citation
Research Report
Can Non-Physician Providers Use Ultrasound to Aid in Establishing Peripheral IV Access in Patients Who are Difficult to Cannulate? A Scoping Review
-
- Published online by Cambridge University Press:
- 20 May 2022, pp. 535-546
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Meeting Abstracts
Rapid Response Mobile Laboratories (RRML): Standardization as a Tool to Maximize Interoperability
-
- Published online by Cambridge University Press:
- 22 November 2022, p. s68
-
- Article
-
- You have access
- Export citation
Research Report
Malaysian Disaster Medicine Research: A Bibliographic Study of Publication Trends
-
- Published online by Cambridge University Press:
- 14 November 2022, pp. 836-842
-
- Article
- Export citation
Treatment of Presumed Hyperkalemia in the Prehospital Setting
-
- Published online by Cambridge University Press:
- 04 August 2022, pp. 693-697
-
- Article
- Export citation
Hockey Puck Strike Rates and Injuries at National Hockey League Games: A Retrospective Analysis of Data from Six Seasons
-
- Published online by Cambridge University Press:
- 18 April 2022, pp. 397-400
-
- Article
- Export citation
Case Report
A Storm, An Explosion, and Flying Rocks - An Unusual Injury due to a Lightning Strike in the Mountains
-
- Published online by Cambridge University Press:
- 27 June 2022, pp. 547-549
-
- Article
- Export citation
A Successful Case of Cardiac Arrest due to Acute Myocarditis with COVID-19: 120 Minutes on Manual Cardiopulmonary Resuscitation then Veno-Arterial Extracorporeal Membrane Oxygenation
-
- Published online by Cambridge University Press:
- 04 October 2022, pp. 843-846
-
- Article
- Export citation
Research Report
Health Care Organizations’ Interoperability during Multi-Organizational Disaster Management: A Scoping Review
-
- Published online by Cambridge University Press:
- 05 April 2022, pp. 401-408
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Heat Health Management in a Quarantine and Isolation Facility in the Tropics
-
- Published online by Cambridge University Press:
- 28 February 2022, pp. 259-264
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Case Report
Vaccine-Induced Myocarditis in Two Intern Doctors in the Same Night Shift
-
- Published online by Cambridge University Press:
- 19 July 2022, pp. 698-700
-
- Article
- Export citation
Meeting Abstracts
The Ethical Triage and Management Guidelines of the Entrapped and Mangled Extremity in Resource Scarce Environments: A Systematic Literature Review
-
- Published online by Cambridge University Press:
- 22 November 2022, p. s69
-
- Article
-
- You have access
- Export citation
Research Report
General Practitioners’ Roles in Disaster Health Management: Perspectives of Disaster Managers
-
- Published online by Cambridge University Press:
- 03 December 2021, pp. 124-131
-
- Article
- Export citation