



Breast-feeding is beneficial to child’s health and development and contributes to human capital development by increasing intelligence quotient scores(Reference Victora, Bahl and Barros1). Worldwide, between 1990 and 2010, the overall prevalence of continuous breast-feeding between the ages of 6 and 11 months and between 12 and 15 months faced a slight decrease from 75·6 % to 72·5 % and from 76 % to 73 %, respectively(Reference Victora, Bahl and Barros1) and continuous breast-feeding among children aged 12–23 months increased from 31·9 % to 59·2 %(Reference Roberts, Carnahan and Gakidou2). In Latin American countries, between 1995 and 2005, the average duration of breast-feeding also increased, especially in Bolivia (16·3 months–21 months), Colombia (11·3–17·5 months) and Peru (17–21·7 months)(Reference Lutter, Chaparro and Grummer-Strawn3).
Public policies are crucial to mitigate the structural and social challenges that reduce breast-feeding rates(Reference Rollins, Bhandari and Hajeebhoy4). Positive examples that foster a supportive environment for breast-feeding are legal guidelines, policies focused on social attitudes and norms, regulation of advertisements for infant formulas, maternal working conditions (paid maternity leave, breaks at work for breast-feeding), structure of health services (joint accommodation, structure for companions, human milk bank, ten steps to breast-feeding success) and training of health professionals (management of breast-feeding)(Reference Rollins, Bhandari and Hajeebhoy4). Most studies reviewed by Rollins et al. (Reference Rollins, Bhandari and Hajeebhoy4) explored the effects of direct interventions rather than evaluating the role of policies and interventions that affect breast-feeding. In a study with fourteen countries, exclusive breast-feeding grew 1 % per year for countries with a higher number of policies and pro-breast-feeding programmes implemented(Reference Lutter and Morrow5).
Access to pro-breast-feeding actions, programmes and policies can be achieved with the use of the World Breastfeeding Trends Initiative (WBTi) developed by the International Baby Food Action Network from Asia in 2004. WBTi is composed of ten indicators related to policies and pro-breast-feeding programmes and five related to indicators of infant feeding practices(6). The objectives of this initiative are to assist public administrators in assessing the status and evolution in the implementation of the Global Strategy for Infant and Young Child Feeding in a standardised manner and to enable the identification of strengths and gaps in the programmes and policies for protection, promotion and support of breast-feeding developed in each country. The assessment process is described in a ‘report card’ and ‘report’ with scores for each indicator related to policy and programmes that protect, promote and support optimal infant and young child feeding practices.
Few studies(Reference Lutter and Morrow5,Reference Gupta, Holla and Dadhich7) have related data of this tool to breast-feeding prevalence rates, showing that we still lack consistent and sufficient results on this relationship in Latin America. This analysis is relevant considering the improvements in breast-feeding rates in this region and the context of actions and policies for breast-feeding and their possible failures, which directly influence this practice. The most recent study on the duration of breast-feeding in Latin America refers to the situation between 1995 and 2005(Reference Lutter, Chaparro and Grummer-Strawn3), and it is important to verify whether the increase in the duration of breast-feeding in the region was maintained, especially considering the profound demographic changes that occurred(8) and the development of public policies aimed at protecting and encouraging breast-feeding(Reference Thulier9). This study aims to describe the duration of breast-feeding between 1990 and 2013 and estimate the association between breast-feeding duration and sociodemographic, health and pro-breast-feeding policies and actions in Latin American countries.
Methods
Study design, data source and sampling
This is a cross-sectional study using data from the Demographic Health Survey program (DHS). The data are publicly available and were obtained from the programme’s website (https://dhsprogram.com/). These are household surveys with national representativeness and complex sampling that includes stratification, conglomeration and weighting. These surveys have data from various indicators on demographics, reproduction, health and nutrition that enable the monitoring and evaluation of public policies. In most surveys, people eligible for interview include women of reproductive age (15–49 years) and children under 3 or 5 years.
Information on pro-breast-feeding actions and policies in Latin American countries was obtained from the WBTi tool, which includes fifteen indicators: ten indicators related to pro-breast-feeding policies and programmes (pro-breast-feeding) and the other five indicators related to infant feeding practices (indicators of breast-feeding and complementary feeding). This study used only the score obtained in the ten indicators that refer to pro-breast-feeding policies and programmes. Each indicator contains a list of criteria, a key question and a set of questions to be considered when evaluating the progress of the implementation and assigning a score for each indicator between 0 and 10 points. The total score for each item ranges between 0 and 10 and the final score for this study ranged between 0 and 100 points (https://worldbreastfeedingtrends.org/). Higher scores indicate that the country develops more pro-breast-feeding actions and policies. The indicators with the respective key questions are available in supplementary material (see online supplementary material, Supplemental Table S1).
Country and sample selection
This study chose Latin American countries presenting the most recent WBTi scores and having DHS surveys later in the same year that the country was scored by the tool. The only exception occurred for Brazil, in which the WBTi scoring year was 2008 and the survey selected with greater proximity was 2006/2007. Two changes occurred in Brazil in 2008: implementation of the Brazilian Breastfeeding Network and maternity leave extended to 6 months in the public sector and in the group Citizen Company (Empresa Cidadã – EC). The EC programme allows extension of maternity leave from 120 to 180 d, and mother chooses to take advantage of the additional 60 d or not. Remuneration for the two additional months of leave is paid by the employer, and the amount spent on the EC programme can be deducted from the companys tax payments. Although the EC programme was approved in 2008, it was only in January 2010 that the programme was effectively enforced with the decree 7052/2009 and Normative Instruction RFB No. 99/2010.
Thus, the countries selected were: Bolivia (WBTi-2008 and DHS-2008), Brazil (WBTi-2008 and DHS-2006), Colombia (WBTi-2009 and DHS-2010), Peru (WBTi-2009 and DHS-2010) and the Dominican Republic (WBTi-2012 and DHS-2013) (see online supplementary material, Supplemental Figure S1). Guatemala met the aforementioned criteria, but the variable used to estimate the duration of breast-feeding was different from other surveys, and there was no information on the exact time of breast-feeding for children who were breastfed. The only information for these children was that they were breastfed.
We included children under 24 months of age, who were alive and who lived with their mother at the time of the interview, totalling 17 318 children (Bolivia: 3354; Brazil: 1904; Colombia: 6959; Dominican Republic: 1399 and Peru: 3702). After adopting these criteria, the percentage of losses ranged between 0 and 4 % (Bolivia: 3·3 %; Brazil: 0 %; Colombia: 1·8 %; Peru: 1·5 % and Dominican Republic: 4·0 %).
All surveys conducted between 1990 and 2013 for each country were selected to estimate the evolution of the duration of breast-feeding in these countries (trend analyses). Thus, the following surveys were included: Bolivia (1994–2008), Brazil (1996–2006), Colombia (1990–2010), Peru (1991–2012) and the Dominican Republic (1991–2013).
Study variables
The study outcome was the duration of breast-feeding obtained based on the variable ‘duration of the child’s breastfeeding in months’ available from DHS. Each country score acquired by the WBTi tool was analysed as an exposure variable, to verify the association between the score obtained with actions and policies of the countries and the duration of breast-feeding. In addition to the WBTi score, other exposure variables were selected following the conceptual model proposed by Rollins et al. (Reference Rollins, Bhandari and Hajeebhoy4), who categorised factors as individual, environmental and structural factors, namely: maternal age (<20, 20–24, 25–29, ≥30 years); maternal education level (no education, primary, secondary, higher); type of maternal work (not working, informal work, formal work)(10); smoking status of mother (yes, no); BMI (<25, 25–29, ≥30 kg/m2)(11); area of residence (urban, rural); number of children (1, 2–3, ≥4); sex of child (male, female); breast-feeding in the first hour (no, yes); child was consulted within 2 months (no, yes); partner lives at home (no partner, no, yes) and wealth index (1st, 2st, 3st, 4st, 5st quintiles). In the first quintile are the people with the lowest incomes and the fifth quintile those with highest income(12).
Statistical analysis
The duration of breast-feeding was expressed as median (months) and defined by survival analysis with Kaplan–Meier curves. In this analysis, children who were being breastfed at the time of interview were classified as ‘censoring’ and those who were not being breastfed were classified as ‘failure.’ Breast-feeding time was censored at 24 months. The variable available in the databases was configured to perform the survival analysis as follows: for children who were never breastfed, 0·0001 was the value assigned in the analysis; for children who breastfed only 1 d, 0·0164 was assigned (represents the division of 1 d by 30·4537 d–1 month); for children who were still breast-feeding, the value was replaced by the child’s age; and for ‘I don’t know-DK’ answers, the value assigned was 0·0164, attributing that the child was breastfed 1 d. The percentage of DK answer was <1 %, ranged from 0·05 % in Peru to 0·8 % in Dominican Republic.
The comparison of sociodemographic and health characteristics between countries was performed by random effects and population-averaged logit model for binary variables and random effects ordered logistic model for ordinal variables.
The analysis of the factors associated with breast-feeding was performed only with the last survey available in the country, as explained above. Categorical variables were expressed in relative frequencies. The adjusted Cox regression model was used to verify the association of the exposure variables at the individual level with the duration of breast-feeding for each country, and estimates were expressed as hazard ratio and 95 % CI. The multilevel survival analysis with random intercept was used to estimate the association between WBTi score and duration of breast-feeding in the pooled analysis, adjusting the individual variables, related to the mother–child dyad and sociodemographic variables. In the first level (level 1), demographic, socio-economic and health care variables about mother and child (individual characteristics) were selected; and in the second level (level 2), the WBTi score (contextual characteristics) was selected. The intraclass correlation coefficient to measure the proportion of the variance (of the outcome variable) due to the countries was calculated. For multilevel survival analysis, the intraclass correlation coefficient is calculated using variance value from contextual (var_cons) and individual level (ln_p).
The variables ‘smoking status of mother’ and ‘child was consulted by a health professional within 2 months after birth’ were not included in the multilevel model because Colombia presented no data for these two variables and Brazil did not present data for the second variable.
The sample design and weighting factor were used in all analyses as a function of the sample being complex (command svy). The significance level adopted was 5 %. All statistical analyses were performed in the Software Stata se® version 15.0.
Ethical considerations
The Demographics and Health Surveys maintain strict standards to protect the participants’ privacy. All surveys were previously approved by the Ethics Research Committee of each country (https://www.dhsprogram.com/What-We-Do/Protecting-the-Privacy-of-DHS-Survey-Respondents.cfm).
Results
Sample characterisation and duration of breast-feeding
The sociodemographic profile and characteristics of the mother–child dyad for each country are described in Table 1. Most mothers were aged 30 years or older (higher prevalence in Peru), with high school education (higher prevalence in Dominican Republic and Peru), who did not work (formal work was higher at Colombia and Dominican Republic) and who had between two and three children (≥4 children were higher in Bolivia and Peru). In all countries, most mothers were non-smokers (variable not available in Colombia), were classified as BMI < 25 kg/m2 (lower prevalence in Brazil) and living in an urban area (higher prevalence in Brazil). Most mothers breastfed in the first hour in Bolivia, Colombia and Peru. In Bolivia, Peru and the Dominican Republic, more than 90 % of mothers reported that their children were consulted by a health professional up to 2 months old. In all countries, most mothers lived with their partner (higher prevalence in Bolivia, Brazil and Peru) (Table 1).
Table 1 Sociodemographic and health characterisation of the mother and child in five Latin American countries, Demographic Health Survey programme (DHS), 2006–2013
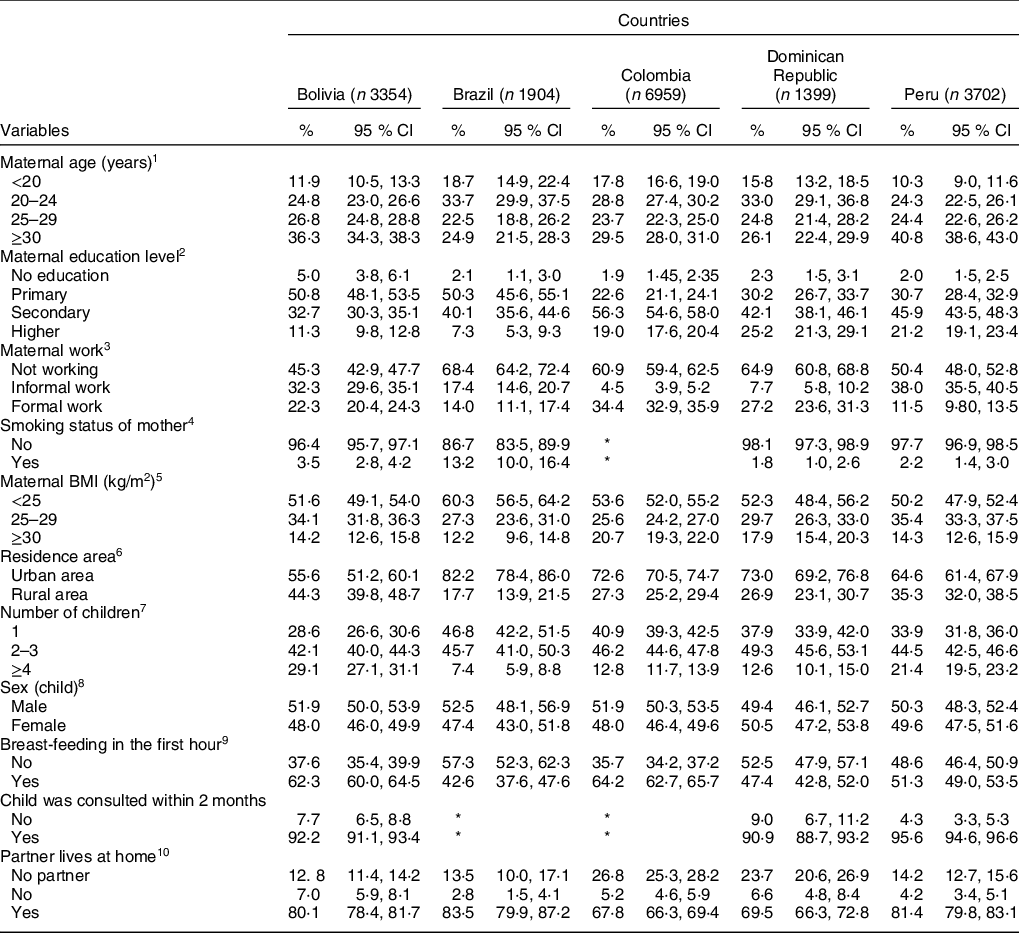
Comparison between countries (P-values) (Peru was considered the reference for comparison): 1 - P < 0·001; 2 - P < 0·001; 3 - P < 0·001 (for Colombia, P = 0·558); 4; 5 - P < 0·001 for Brazil (P = 0·499 for Colombia, P = 0·558 for Bolivia, P = 0·830); 6 - P < 0·001; 7 - P < 0·001; 8 - (for Colombia, P = 0·174; for Brazil, P = 0·103; for Bolivia, P = 0·560; for Dominican Republic, P = 0·723); 9 - P < 0·001; 10 - P < 0·001 (for Brazil, P = 0·625).
* Data not available in the country database.
A significant increase in the duration of breast-feeding occurred in all countries analysed over the years, except in the Dominican Republic (P = 0·162). In Bolivia, the median duration increased from 18 to 20 months between 1994 and 2003 and decreased to 19 months in 2008. In Brazil, between 1996 and 2006, the median duration increased from 6 to 12 months. In Colombia, the duration of breast-feeding increased from 9 to 14 months between 1990 and 2010. In Peru, between 1991 and 2011, the duration increased from 18 to 22 months, and in 2012 was higher than 22 months. In the Dominican Republic, in addition to the increase of 2 months between 1991 and 2013, the initial rate was lower than in other countries (Fig. 1).
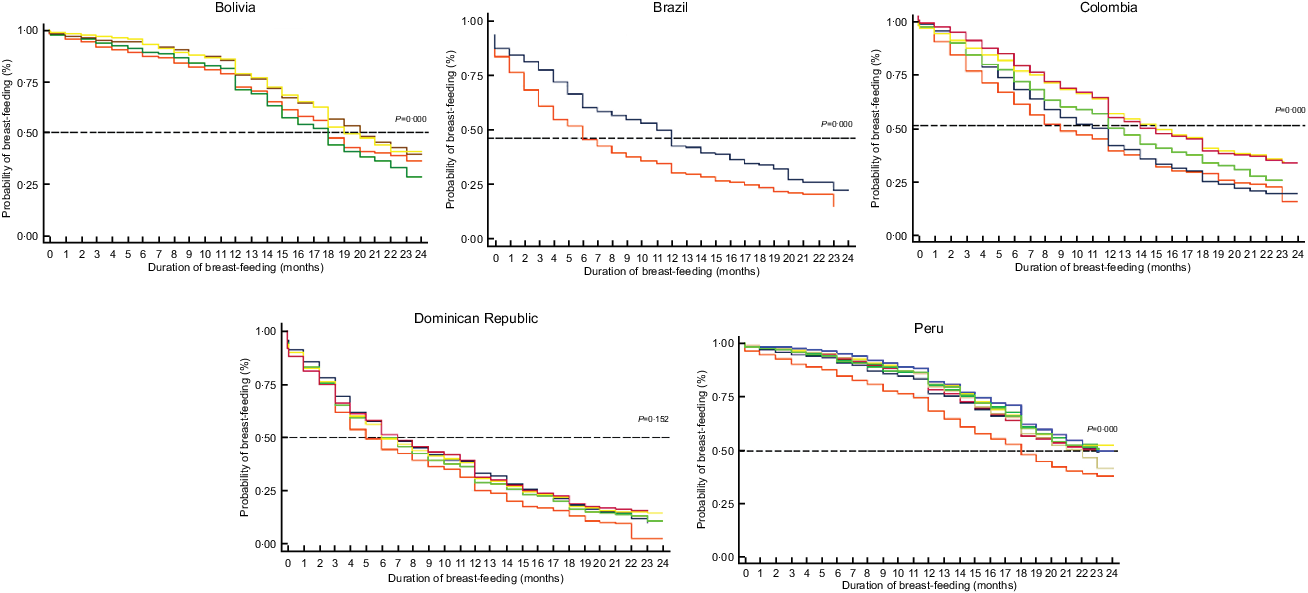
Fig. 1 Survival curves (Kaplan–Meier) of breast-feeding duration in children under 24 months of age in five Latin American countries. Demographic Health Survey programme (DHS), 1990 to 2013. Bolivia: ![]() , 1994;
, 1994; ![]() , 1998;
, 1998; ![]() , 2003;
, 2003; ![]() , 2008. Brazil:
, 2008. Brazil: ![]() , 1996;
, 1996; ![]() , 2006. Colombia:
, 2006. Colombia: ![]() , 1990;
, 1990; ![]() , 1995;
, 1995; ![]() , 2000;
, 2000; ![]() , 2005;
, 2005; ![]() , 2010. Dominican Republic:
, 2010. Dominican Republic: ![]() , 1991;
, 1991; ![]() , 1996;
, 1996; ![]() , 2002;
, 2002; ![]() , 2007;
, 2007; ![]() , 2013. Peru:
, 2013. Peru: ![]() , 1991;
, 1991; ![]() , 1996;
, 1996; ![]() , 2000;
, 2000; ![]() , 2006;
, 2006; ![]() , 2009;
, 2009; ![]() , 2010;
, 2010; ![]() , 2011;
, 2011; ![]() , 2012
, 2012
Factors associated with the duration of breast-feeding
In Colombia (HR = 0·79, 95 % CI 0·65, 0·97) and Peru (HR = 0·61, 95 % CI 0·38, 0·95), mothers who were 30 years or older breastfed for longer, when compared with mothers who were under 20 years of age. Regarding maternal schooling, it was observed that the higher the schooling, the higher the risk of weaning in Colombia (HR = 1·76, 95 % CI 1·14, 2·70), Peru (HR = 2·70, 95 % CI 1·34, 5·42) and the Dominican Republic (HR = 3·06, 95 % CI 1·54, 6·07). Mother working in the informal sector was associated with longer duration of breast-feeding in Brazil (HR = 0·66, 95 % CI 0·48, 0·91) and working in the formal sector was associated with short duration of breast-feeding in Colombia (HR = 1·12, 95 % CI 1·00, 1·26). Mothers with BMI ≥ 30 kg/m2 had a higher risk of weaning in Bolivia (HR = 1·48, 95 % CI 1·12, 1·95), Brazil (HR = 1·54, 95 % CI 1·10, 2·16) and Dominican Republic (HR = 1·31, 95 % CI 1·01, 171) compared with mothers with BMI < 25 kg/m2. Only Peru presented an association on the housing area, and mothers living in rural area (HR = 0·65, 95 % CI 0·51, 0·84) breastfed for longer periods when compared with mothers living in the urban area. Mothers classified in the upper income quintiles breastfed for a shorter time. Breast-feeding in the first hour of life was a protective factor for a longer duration of breast-feeding in all countries, except Peru. The child being consulted by a health professional within 2 months of life was also considered a protective factor to increase the time of breast-feeding in Bolivia (HR = 0·27, 95 % CI 0·21, 0·35) and Peru (HR = 0·38, 95 % CI 0·26, 0·54). Mother not living with her partner was associated with short duration of breast-feeding in Peru (HR = 1·66, 95 % CI 1·02, 2·71) (Table 2).
Table 2 Association of breast-feeding duration and sociodemographic and health characteristics according to country, Demographic Health Survey programme (DHS), 2006–2013
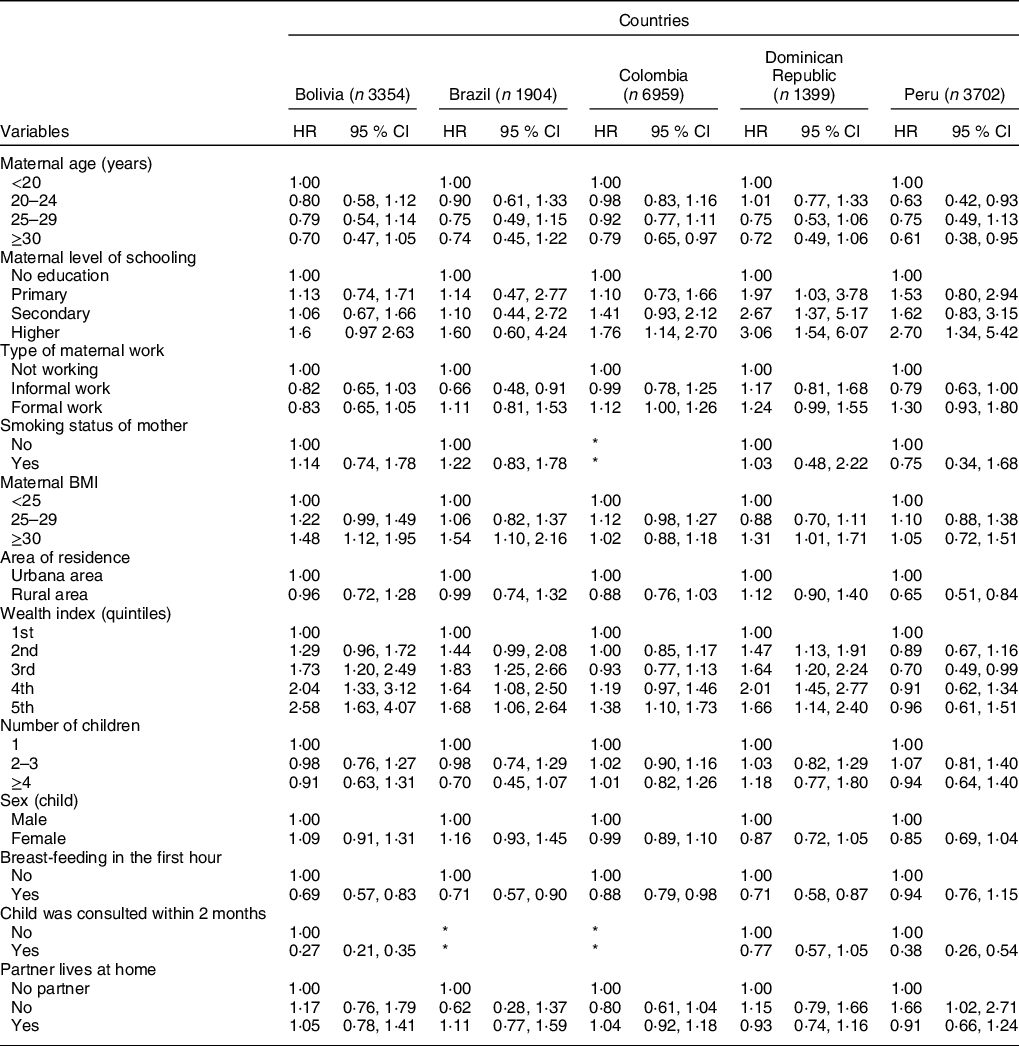
* Data not available in the country database.
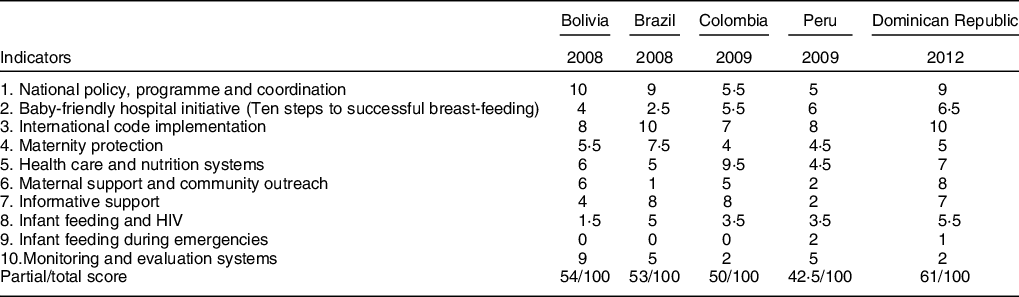
A descriptive analysis of pro-breast-feeding actions based on the WBTi was performed, as well as their association with the duration of breast-feeding. The Dominican Republic performed the highest score, with 61 points, while Peru scored the lowest score (42·5). In general, the indicators with the highest score were ‘National policy, program and coordination’ (item 1) and ‘Implementation of the International Code’ (item 4), while the indicators with the lowest scores were ‘Infant Feeding and HIV’ (item 8) and ‘Infant Feeding during emergencies’ (item 9) (Table 3).
Table 3 Partial and total scores of the World Breastfeeding Trends Initiative (WBTi) tool for each country
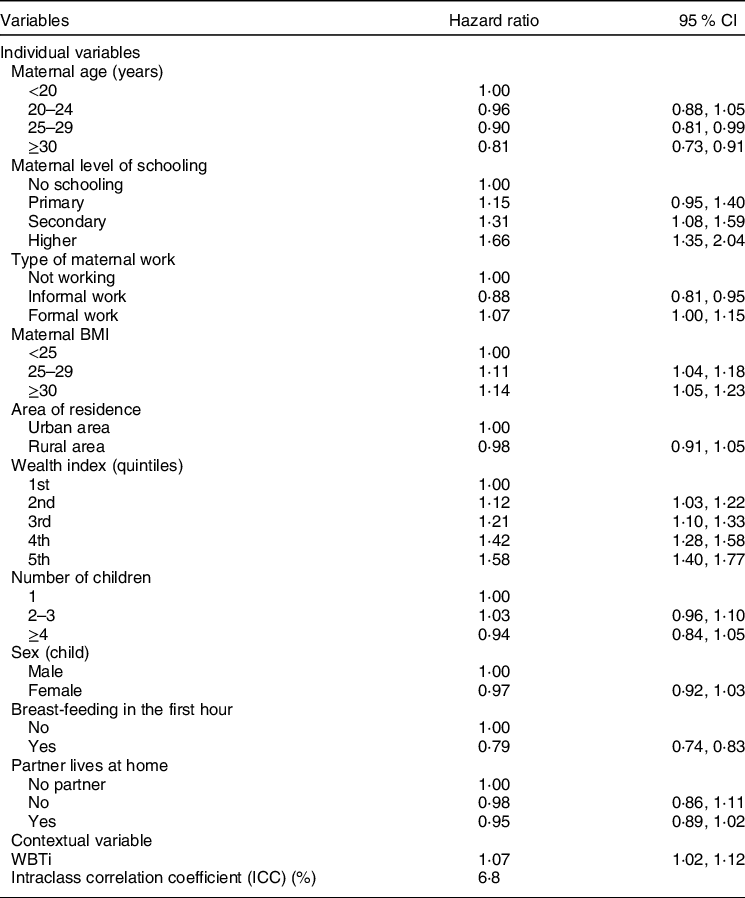
In the joint analysis of all countries, higher maternal age (HR = 0·81, 95 % CI 0·73, 0·91) and breast-feeding the infant within the first hour of life (HR = 0·79, 95 % CI 0·74, 0·83) were factors associated with a longer time of breast-feeding. Higher maternal education, mother working in the formal sector, BMI and wealth index were associated short duration of breast-feeding. Regarding the score of the WBTi variable, we observed a shorter duration of breast-feeding in countries with higher scores (HR = 1·07, 95 % CI 1·02, 1·12). We found that 6·8 % of the variation in the duration of breast-feeding was explained by the country level (intraclass correlation coefficient) (Table 4).
Table 4 Association between sociodemographic, health and World on Breastfeeding Trends Initiative (WBTi) and breast-feeding duration in five Latin American countries, Demographic Health Survey programme (DHS), 2006–2013
The Dominican Republic was the only country with stagnation of the duration of breast-feeding in the last 20 years, presenting the highest score in the WBTi (an outlier in the set of countries). Therefore, we performed further multilevel analysis without this country, and the association between WBTi and the duration of breast-feeding was no longer statistically significant (HR = 1·06, 95 % CI 0·98, 1·15).
Discussion
The duration of breast-feeding increased significantly in all countries analysed over the selected period, except in the Dominican Republic. We highlight that the initial duration of breast-feeding was already higher in Bolivia and Peru when compared with that of other countries. Higher levels of maternal schooling, higher quintiles of income and higher BMI were associated with shorter duration of breast-feeding. Breast-feeding in the first hour of life and infant being consulted by a health professional within 2 months of life were factors associated with longer duration of breast-feeding. Regarding the score of the WBTi variable (context variable), the Dominican Republic was the country with the highest score but presenting the lowest duration of breast-feeding. On the other hand, Peru presented the lowest score in the tool and the longest duration of breast-feeding. Generally, higher WBTi scores were not associated with longer durations of breast-feeding.
In this study, higher maternal schooling was associated with shorter duration of breast-feeding, corroborating results from other studies(Reference Chu, Guo and Jay13–Reference Witwer18). Higher schooling levels mean that women have more job opportunities, thus prioritising their professional career(Reference Wang, Wang and Zhang19). Moreover, mothers with higher education level work full time(Reference Kang, Liang and Liu20,Reference Wu and Qiu21) and maybe the work environment does not offer a supportive place for breast-feeding(Reference Nardi, Frankenberg and Franzosi22). Mothers with higher education level probably have jobs with higher wages and, therefore, higher income to buy infant formula at any time and maintain this consumption for longer time. Prevalence of infant formula under 6 months was higher in the wealthiest families in fifty-nine low- and middle-income countries(Reference Neves, Gatica-Domínguez and Rollins23).
Mothers classified in the highest quintiles of income breastfed for a shorter time. A similar result was found in another study, in which mothers in the higher income quintiles had an increased risk of discontinuation of breast-feeding when compared with mothers with lower income(Reference Oliveira, Boccolini and Faerstein24). Lower-income mothers tend to breastfeed for longer periods when compared with mothers with higher incomes in the ninety-eight low- and middle-income countries(Reference Victora, Bahl and Barros1). These results suggest that the patterns related to breast-feeding are contributing to reduce the health differences between rich and poor children in low- and middle-income countries, which would be even higher without breast-feeding(Reference Victora, Bahl and Barros1).
Overweight women were more likely to wean in our study, as already documented in previous studies(Reference Amir and Donath25–Reference Wojcicki28). The reasons are related to knowledge about breast-feeding, social influence on breast-feeding and lower maternal confidence(Reference Hauff, Leonard and Rasmussen29), as well as physical obstacles, such as larger breasts, larger areolas, excessive body tissue, difficulties with position and handling the baby while breast-feeding(Reference Garner, McKenzie and Devine30–Reference Massov32). The prevalence of overweight condition in Latin America is growing, with almost 28 % of the adult women population in the region being classified as obese(Reference FAO33). Thus, health professionals working directly with mothers must be trained to provide more individualised support during and after pregnancy, especially for overweight or obese women, so they can start and continue breast-feeding(Reference Chang, Glaria and Davie34).
Regarding the factors increasing the duration of the breast-feeding, we highlight the breast-feeding in the first hour of life. Recent evidence shows that skin-to-skin contact between mother and child soon after childbirth supports early breast-feeding onset and increases the chance of exclusive breast-feeding and the total duration of breast-feeding(Reference Moore, Bergman and Anderson35,Reference Jaafar, Ho and Lee36) . Another factor associated with longer duration of breast-feeding was that the baby was consulted with a health professional within 2 months after childbirth. Possibly, mothers who went to consultations with health professionals in the postpartum period were able to have their doubts answered and receive support from health professionals about the management of breast-feeding. Qualified health professionals are needed to provide the appropriate support that mothers need, as well as to overcome the difficulties with breast-feeding(Reference Pérez-Escamilla, Curry and Minhas37). Paediatricians are trained to promote and support breast-feeding. However, shortcomings during their training may occur, especially in the management of breast-feeding. Furthermore, these professionals must participate in continuing education courses. The adequate support in the management of breast-feeding in the first days and weeks after childbirth is extremely relevant for long-term breast-feeding(Reference Pérez-Escamilla38).
The Dominican Republic was the country with the highest score for the WBTi variable and the lowest duration of breast-feeding, whereas Peru had the lowest score in the tool and the longest duration of breast-feeding. A possible explanation for this result is that countries with lower breast-feeding rates make more efforts to implement actions and policies for breast-feeding, thus aiming to increase the rates and obtaining higher scores in the tool. The process of WBTi assessment is based on objective criteria, and each country has a trained team to perform the assessment. Therefore, the scoring process is not subjective, but there is no assessment of whether the country actually complies with existing policies and legislation. This may help to explain the results in Dominican Republic, which has the best score but shortest duration of breast-feeding, potentially due to problems in the implementation of policies.
In the study by Lutter and Morrow(Reference Lutter and Morrow5), the relationship between the implementation of the Global Strategy for Infant and Young Child Feeding measured by WBTi and trends in the duration of exclusive breast-feeding and breast-feeding in the last 20 years was verified. All countries evaluated presented an increase in exclusive breast-feeding values, being strongly associated with higher WBTi scores. However, no association was found between the annual change of breast-feeding and the WBTi score, as noted in our study after removing the Dominican Republic from analysis.
Bolivia was one of the countries with the longest duration of breast-feeding, emphasising that the initial duration of the country was already higher when compared with other countries. Despite Bolivia being one of the poorest countries in the region, their national policies and pro-breast-feeding programmes cover several strategies and multisectoral actions for protection and support breast-feeding(Reference Pérez-Escamilla39,40) , promoting better breast-feeding practices at national level when compared with richer countries.
Brazil significantly increased the duration of breast-feeding in the period. Due to low rates in the past, intense national mobilisation occurred with the implementation of many actions and pro-breast-feeding policies in the country to increase such indicators. Currently, the country has a very comprehensive policy to ensure breast-feeding and adequate infant feeding. Brazil’s National Strategy for Promotion of Breast-feeding, maternity leave from 4 months to 6 months, implementation of the Brazilian Rule for the Marketing of Infant Foods (NBCAL – Norma Brasileira para Comercialização de Alimentos para Lactentes), implementation of the Baby-Friendly Hospital Initiative, counselling courses, breast-feeding management courses, NBCAL review, pro-breast-feeding events every 2 years and World Breastfeeding Week(41) are some of the programmes and actions for breast-feeding implemented in the country and that contributed to the increase in the duration of breast-feeding.
Colombia also presented a relevant increase in the duration of breast-feeding between 1990 and 2010. Note that the country is in the middle of an armed conflict scenario that may have indirect influence in the practice of breast-feeding; however, it was one of the countries that presented the greatest evolution in the duration of breast-feeding(Reference Eckstein and Wickham-Crowley42). Between 1990 and 2000, Colombia underwent a process of political and institutional change, and after years of political and civil violence, the government focused on the reconstitution of State dominance over the entire country. Therefore, the coverage of services and public policies grew, especially in the health area(Reference Eckstein and Wickham-Crowley42), with expanded public funding that prioritised comprehensive social programmes such as education and health. In Colombia, investment in health funded the National Food and Nutrition Plan from 1996 to 2005 and began to promote breast-feeding(43,44) . The risk of weaning in rural Colombia may increase given the backdrop of civil violence and armed political conflicts in these areas(44).
Peru was the country with the longest duration of breast-feeding since the 1990s. The greatest force for breast-feeding in the country is the cultural issue, and it is more frequent among mothers belonging to the lowest income quintile(45). In 2009, Peru was in an economic growth with resources to invest in priority problems such as infant feeding and pro-breast-feeding programmes and actions. Peru was the only country where breast-feeding was higher in the rural area. In the country, a relevant factor to prioritise is the dissemination of adequate information material for rural and urban populations(45).
The Dominican Republic is the country with the shortest duration of breast-feeding and the lowest evolution of this indicator over the years. These results are even more significant, since almost all childbirths are performed in health units and are attended by health professionals, who must follow the provisions of Law 8–95 and its regulations on breast-feeding(46). There is no rooming in policy(47), and infant formula is distributed in hospitals, even with maximum score for this item in the tool (item 3–legislation for regulating the commercialisation of infant formulas). These factors may contribute to the onset of breast-feeding not occurring as recommended thus impacting in its continuity. According to the information available in the official DHS reports conducted in this country in 2002 and 2007, exclusive breast-feeding was already low and continued to decline and due to this trend, complementary feeding begins early in most children. The results also indicate that most children are fed with baby bottle soon after childbirth(48,49) , which also influences the low rates of duration of breast-feeding in the country.
The promotion of breast-feeding is one of the cheapest interventions to promote the health of the mother–child dyad. However, investments are necessary in all determining factors as proposed by Rollins et al. (Reference Rollins, Bhandari and Hajeebhoy4). Pérez-Escamilla(Reference Pérez-Escamilla, Curry and Minhas37) proposes the ‘model of breast-feeding gears,’ which indicates the need for several main gears to be functioning in sync and in a coordinated manner. Evidence-based awareness is important to produce the fundamental political will to pass legislation and policies aimed at protecting, promoting and supporting breast-feeding at hospital and community level. The policy axis leads to appropriate resources to encourage the development of workforce and the delivery of programmes and the promotion of breast-feeding. Constant research and evaluation are important for the creation of goals and system feedback(Reference Pérez-Escamilla, Curry and Minhas37). Discrepant scores can be observed between indicators of the same country and for the maintenance and effective applicability of pro-breast-feeding policies and actions, countries should present better scores in all indicators, and not only in some.
This study has some limitations. First, the absence of variables relevant to the outcome, such as the mother’s intention to breastfeed, support of both partner and family for the breast-feeding (support network), mother receiving guidance and training on breast-feeding in prenatal care and especially in the postnatal period. Another limitation is related to maternal work; we selected two questions about maternal work – “currently working – yes or no” and standardised woman occupation groups – classified as “informal and formal work” – but DHS surveys do not present variables about maternity leave or a variable about work load. Therefore, it was impossible to identify mothers who are not working because of maternity leave or if who were not working at all. Formal work was associated with shorter duration of breast-feeding; we can assume some reasons to explain such results, including working full-time (formal sector); a higher percentage of mothers within formal work who had already taken their maternity leave (our sample was composed mainly of children aged at least 4 months); mothers’ work environment was not supportive of breast-feeding. In a systematic review, part-time jobs and later or no return to work were associated with longer duration of breast-feeding, whereas full-time work was associated with shorter duration(Reference Nardi, Frankenberg and Franzosi22). Lactation rooms in work environments can support mothers pump breast milk during work time(Reference Nardi, Frankenberg and Franzosi22). Another limitation refers to the WBTi tool. The first refers to the lack of information from the year of implementation of policies or actions, which prevents us from knowing when they were enforced. If these actions were implemented recently, it is likely that the time is insufficient to analyse the effect on breast-feeding. The items scored in the tool do not accurately measure the coverage and monitoring of action or policies, but rather the existence of such instruments in countries. The lack of more recent data on duration of breast-feeding is another limitation. Our study selected the WBTi assessment developed prior to or in the same year of breast-feeding (outcome). This limits our ability to discuss current prevalence of breast-feeding and current policies; however, the associations we explored are less likely to have been affected by the year of data available.
This study also has some strengths. First, an observational study for evaluation of national public policies and public health interventions is relevant since randomised clinical trials alone would not be sufficient or ideal. Evaluating the effect of public health programmes on population is not easy since several interventions are usually performed and their effects are complex and susceptible to modifications. Evidence-based public health requires multiple types of evidence, usually combined(Reference Victora, Habicht and Bryce50). Second, the incorporation of actions and policies for breast-feeding in analyses using information summarised in the WBTi scores. The last is the use of national representativeness data, allowing the results to be extrapolated to the infant population of each country.
We suggest future studies to focus on exploring the scores and indicators of the tool, as well as longitudinal analyses to actually evaluate the evolution occurring over time in relation to pro-breast-feeding policies and improvement in breast-feeding rates, as well as to determine items that may be added to this tool.
Conclusion
The duration of breast-feeding increased significantly in four of the five countries analysed. We found that breast-feeding in the first hour of life and the baby having been consulted by a health professional within 2 months of life were factors associated with the increase in the duration of breast-feeding. Such factors are behaviours closer to mother–child dyad and reflect the training of health professionals to support and assist the mother in establishing breast-feeding. Regarding risk factors, we found that mothers with higher BMI and mothers classified in the higher income quintiles were factors associated with the shorter duration of breast-feeding. Higher scores from the WBTi tool did not result in longer breast-feeding duration. In Latin America, few studies exist relating the status of these actions to the situation of breast-feeding. This study contributes to fill this gap with new analytical perspectives.
Acknowledgements
Acknowledgements: The National Council for Scientific and Technological Development (CNPq), no. 427673/2016-0. Financial support: This work was funded by the National Council for Scientific and Technological Development (CNPq), no. 427673/2016-0. The financial support was for translation of the article and purchase of software for additional statistical analysis. Conflict of interest: None. Authorship: D.M.B.L. configuration of the databases, statistical analysis and writing of the manuscript. A.E.M.R. study design, statistical data analysis and final review of the manuscript writing. C.M.A. contributions to analytical decisions and revision of the manuscript writing. J.L.F.A. and W.L.C. contributions to statistical analysis and final review of the manuscript. Ethics of human subject participation: This study was conducted in accordance with the Helsinki declaration rules and all procedures involving research participants that were approved by the Research Ethics Committee of each country (https://www.dhsprogram.com/What-We-Do/Protecting-Privacy-DHS-Survey-Respondents.cfm).
Supplementary material
For supplementary material accompanying this paper visit https://doi.org/10.1017/S1368980020005145







