
19 results
How cultural factors along with mental health diagnoses influence the treatment of a stroke patient with no previous mental health history: a case report
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S822-S823
-
- Article
-
- You have access
- Open access
- Export citation
Suicide behaviour after hospitalisation and related factors: a case report.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S1115
-
- Article
-
- You have access
- Open access
- Export citation
New-Onset Bipolar Disorder in Late Life: a case report and review of literature
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S691
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
The elderly represents the fastest growing group of the population. It is fair to assume that the portion of old age patients suffering from bipolar disorder will grow in a similar manner. Elderly patients represent approximately 25% of the bipolar population. Summarizing, 5–10% of patients were 50 years of age when they experienced their first manic episode, constituting the subgroup of late onset bipolar disorder (LOBD).
ObjectivesThe purpose of this case report and literature review is to emphasise the importance of LOBD in old population and to highlight its still sparse-knowledge.
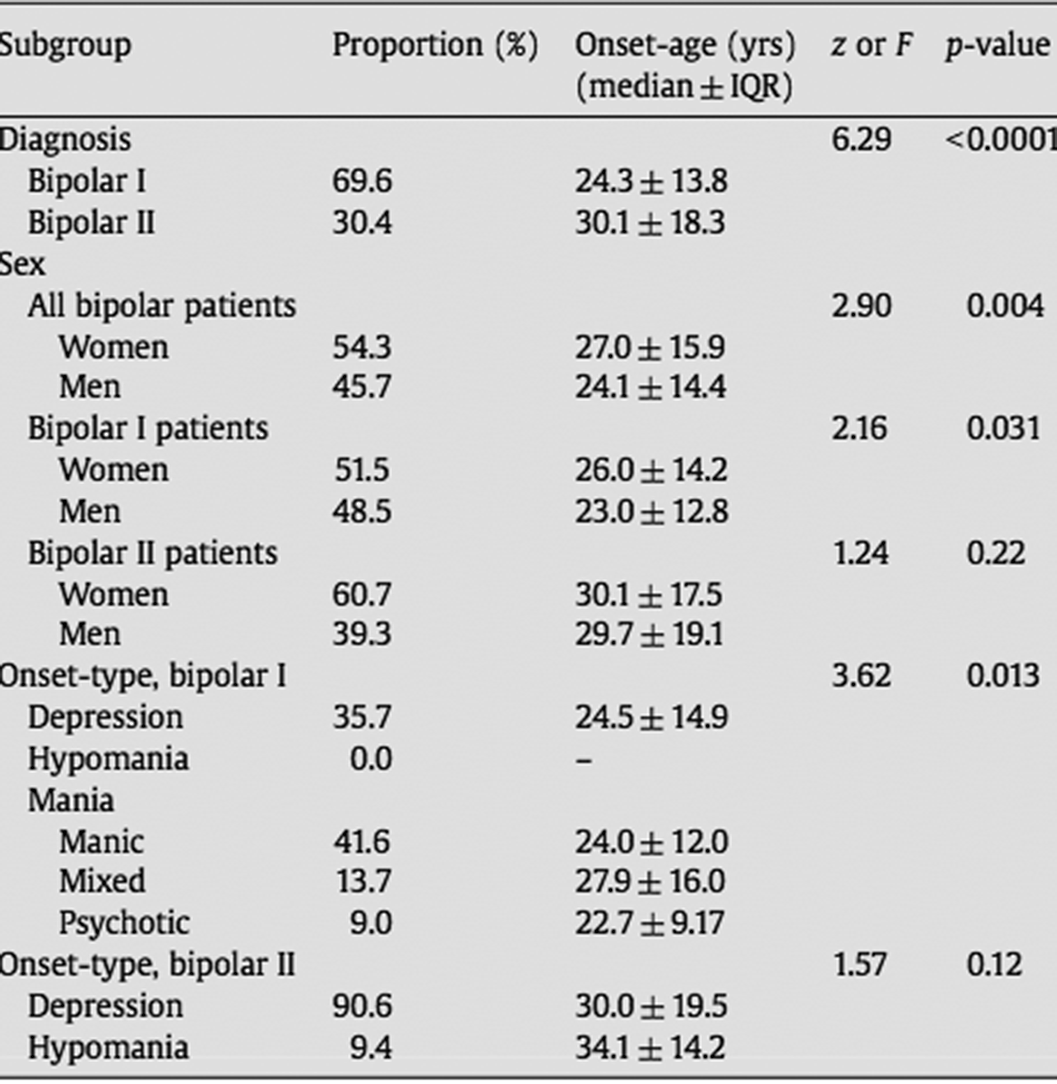
MethodsDescriptive case study and review of literature (Arnold,I. et al. Old Age Bipolar Disorder—Epidemiology, Aetiology and Treatment. Medicina 2021,57,587; Baldessarini et al. Onset-age of bipolar disorders at six international sites. J Affect Disord 2010;121(1-2):143-6).
ResultsA 60-year-old woman is brought to the emergency department for evaluation by her family. Over the past 7 days, the patient has become increasingly irritable and argumentative, is sleeping less, is talking faster than usual and has begun to express paranoid concerns about her students “stealing my exam”. The patient is a university professor.
In the assessment interview she is hyperverbal, expansive, and grandiose. The family has also just recently discovered that she has spent a large sum of money on the Internet.
She has no history of psychiatric contact or substance use disorders; however, she has a family history of severe depression.
In the absence of any plausible non-psychiatric condition that could mimic or induce mania, the working diagnosis is bipolar I disorder, most recent episode (MRE) manic with psychotic features.
Image:
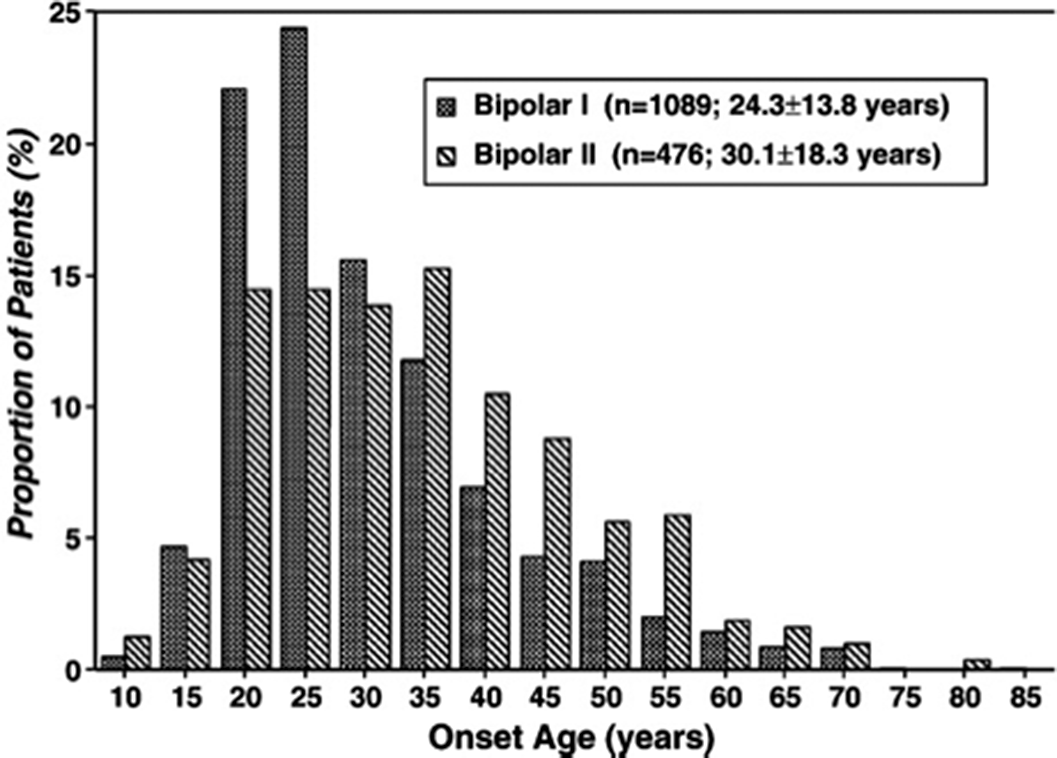
Image 2:
 Conclusions
ConclusionsThe share of older age bipolar disorder will grow constantly in the next decades and further research on this neglected patient group is urgently required.
Disclosure of InterestNone Declared


Lithium management in pregnant patients with bipolar disorder
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S198
-
- Article
-
- You have access
- Open access
- Export citation
Clozapine use in drug induced psychosis in Parkinson´s disease: a case report and review of literature.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S1041
-
- Article
-
- You have access
- Open access
- Export citation
Psychotic denial of pregnancy: case report and narrative literature review.
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S1129
-
- Article
-
- You have access
- Open access
- Export citation
Application of family therapy in a case of anorexia nervosa
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S848
-
- Article
-
- You have access
- Open access
- Export citation
Mania induced after corticosteroid treatment: a case report
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S697
-
- Article
-
- You have access
- Open access
- Export citation
Psychotic symptoms in eating disorders: a case report
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S848-S849
-
- Article
-
- You have access
- Open access
- Export citation
Hysteria in neurology: a diagnostic approach to conversive disorder
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S395
-
- Article
-
- You have access
- Open access
- Export citation
Proposal of a therapeutic algorithm for the psychopharmacological management of treatment-resistant depression
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S567
-
- Article
-
- You have access
- Open access
- Export citation
Functional Neurological Disorder: a multidisciplinary approach
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S396
-
- Article
-
- You have access
- Open access
- Export citation
Hysteria: history of a conceptual and clinical pathomorphosis
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S545-S546
-
- Article
-
- You have access
- Open access
- Export citation
Dealing with Posttraumatic Nightmares
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S674
-
- Article
-
- You have access
- Open access
- Export citation
Griefing reaction and social networks
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S577
-
- Article
-
- You have access
- Open access
- Export citation
Image testing in psychiatrics: a bibliografic review
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S641-S642
-
- Article
-
- You have access
- Open access
- Export citation
Ischemic colitis induced by psychotropics drugs: a case report
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, p. S710
-
- Article
-
- You have access
- Open access
- Export citation
The overlap between complex posttraumatic stress disorder and borderline personality disorder
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, p. S754
-
- Article
-
- You have access
- Open access
- Export citation
Electroconvulsive therapy in the medical comorbidities context: A case report
-
- Journal:
- European Psychiatry / Volume 64 / Issue S1 / April 2021
- Published online by Cambridge University Press:
- 13 August 2021, pp. S689-S690
-
- Article
-
- You have access
- Open access
- Export citation
