
4 results
Transition to Psychosis in Individuals at Clinical High Risk: Meta-analysis
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, p. S367
-
- Article
-
- You have access
- Open access
- Export citation
Lurasidone augmentation to clozapine in treatment resistant schizophrenia: A pilot study
-
- Journal:
- European Psychiatry / Volume 66 / Issue S1 / March 2023
- Published online by Cambridge University Press:
- 19 July 2023, pp. S306-S307
-
- Article
-
- You have access
- Open access
- Export citation
Efficacy and tolerability of brexpiprazole in patients with psychotic and mood disorders: a pilot study
-
- Journal:
- European Psychiatry / Volume 65 / Issue S1 / June 2022
- Published online by Cambridge University Press:
- 01 September 2022, pp. S346-S347
-
- Article
-
- You have access
- Open access
- Export citation
-
Introduction
Brexpiprazole is a novel antipsychotic drug. It exerts antagonistic activity at the serotonin 5HT2A, 5HT2B, 5HT7 and noradrenaline alpha 1b/2c receptors; it also acts as partial agonist of serotonin 5HT1 and dopamine D2, D3 receptors. Brexpiprazole is approved for the treatment of schizophrenia and as an add-on therapy for major depression.
ObjectivesThis pilot study aims at exploring efficacy and tolerability of Brexpiprazole in a small sample of patients diagnosed with either a psychotic or a mood disorder.
MethodsThis observational study was conducted at our Acute Psychiatric Inpatient Unit. We included 7 patients (5 males, 2 females) hospitalized between 2020 and 2021, diagnosed with schizophrenia spectrum disorders or mood disorders with psychotic symptoms confirmed by Mini International Neuropsychiatric Interview. Patients who participated signed an informed consent. Information concerning diagnosis, demographic characteristics (age, sex, education, marital status) and pharmacological therapy were collected examining clinical records. The average lenght of hospitalization was 13.4 days. Psychopathology was assessed by means of the PANSS and the severity of the illness was evaluated with CGI severity scale (CGI-S), both on admission and discharge. We also administered the UKU scale to evaluate the tolerability profile.
Results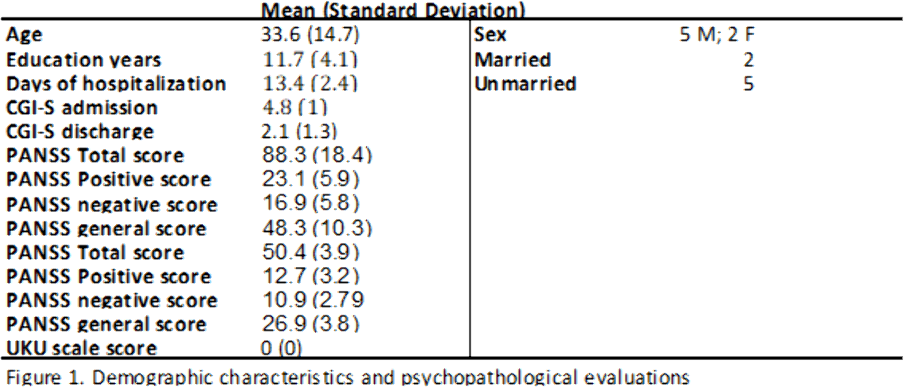

.
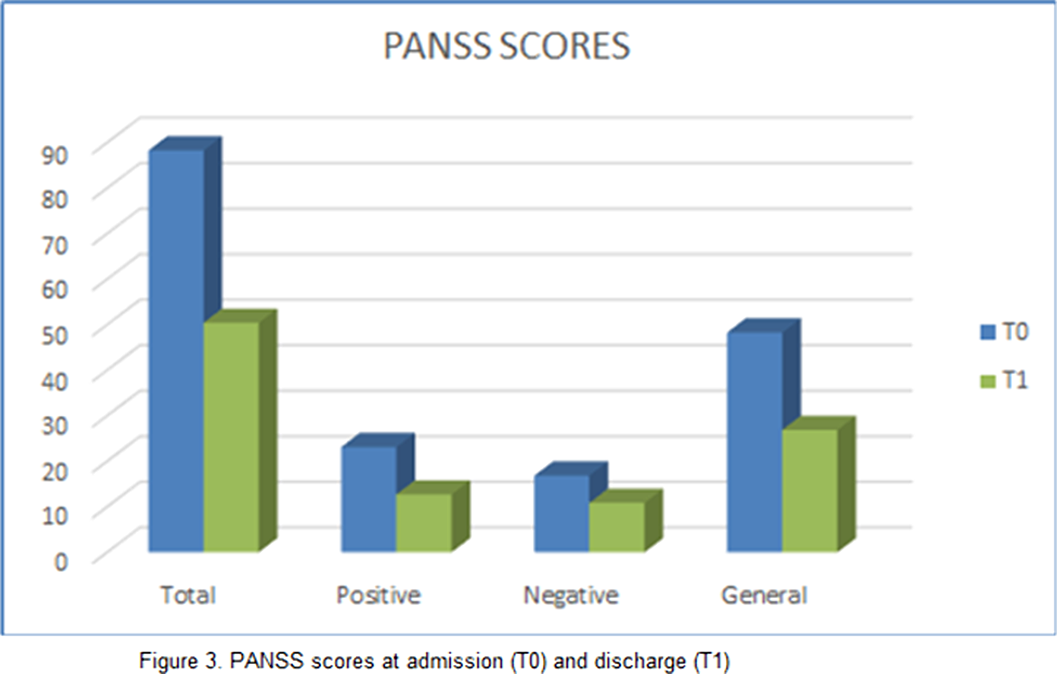
Results can be seen in figures 1, 2, 3
ConclusionsOur study found a significant improvement in both positive and negative symptoms, with good tolerability. Limitations of our study are: small sample size and limited period of observation. These premises suggest that further research is needed in order to elucidate the exact mechanisms underlying Brexpiprazole’s action and the possible implication in mood disorders.
DisclosureNo significant relationships.



Clinical outcomes in individuals at clinical high risk of psychosis who do not transition to psychosis: a meta-analysis
-
- Journal:
- Epidemiology and Psychiatric Sciences / Volume 31 / 2022
- Published online by Cambridge University Press:
- 19 January 2022, e9
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
