
10 results
Evaluating indwelling devices and other risk factors for mortality in invasive Carbapenem-resistant Enterobacterales infections in Georgia, 2012–2019
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue 1 / 2023
- Published online by Cambridge University Press:
- 02 January 2024, e254
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
20 Examining the Recovery Course of Pediatric Concussion Patients with Protracted Recovery Referred to a Specialty Concussion Clinic
-
- Journal:
- Journal of the International Neuropsychological Society / Volume 29 / Issue s1 / November 2023
- Published online by Cambridge University Press:
- 21 December 2023, pp. 896-897
-
- Article
-
- You have access
- Export citation
Carbapenemase genes and mortality in patients with carbapenem-resistant Enterobacterales, Atlanta, Georgia, 2011–2020
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 3 / Issue S2 / June 2023
- Published online by Cambridge University Press:
- 29 September 2023, pp. s12-s13
-
- Article
-
- You have access
- Open access
- Export citation
-
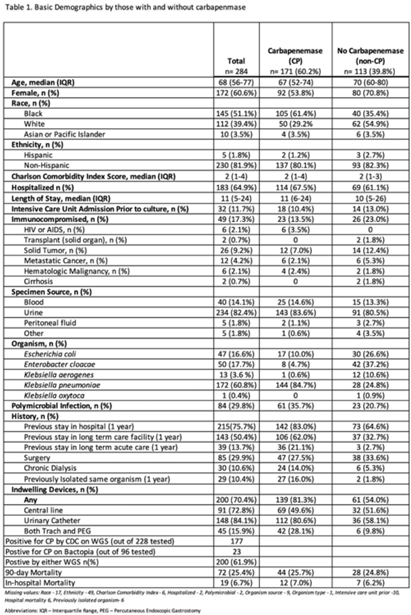
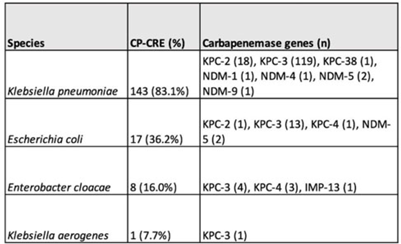
Background: Carbapenemase genes in carbapenem-resistant Enterobacterales (CP-CRE) may be transmitted between patients and bacteria. Reported rates of carbapenemase genes vary widely, and it is unclear whether having a carbapenemase gene portends worse outcomes given that all patients with CRE infections have limited treatment options. Methods: Using active population- and laboratory-based active surveillance data collected by the US CDC-funded Georgia Emerging Infections Program from 2011 to 2020, we assessed the frequency of carbapenemase genes in a convenience sample of CRE isolates using whole-genome sequencing (WGS), and we investigated risk factors for carbapenemase positivity. Only the first isolate per patient in a 30-day period was included. We compared characteristics of patients with CP-CRE and non–CP-CRE. Using multivariable log binomial regression, we assessed the association of carbapenemase gene positivity and 90-day mortality. Results: Of 284 CRE isolates, 171 isolates (60.2%) possessed a carbapenemase gene (Table 1), and KPC-3 was the most common carbapenemase gene (80.7%), with only 7 isolates possessing NDM (Table 2). No isolates possessed >1 carbapenemase gene, and most isolates were from urine (82.4%) (Table 1). Carbapenemase gene positivity was associated with lower age, male sex, black race, infection with Klebsiella pneumoniae, polymicrobial infection, having an indwelling medical device, receiving chronic dialysis, and prior stay in a long-term acute-care hospital, long-term care facility, and/or prior hospitalization in the last year. The 90-day mortality rates were similar in patients with non–CP-CRE and CP-CRE: 24.8% versus 25.7% (P = .86). In multivariable analysis, carbapenemase gene presence was not associated with 90-day mortality (adjusted risk ratio, 0.82; 95% CI, 0.50–1.35) when adjusting for CCI, infection with Klebsiella pneumoniae, and chronic dialysis use. Conclusions: The frequency of CP-CRE among CRE was high in this study, but unlike prior studies, the 90-day mortality rates wer similar in patients with CP-CRE compared to non–CP-CRE. Our results provide novel associations (eg, lower age, male sex, infection with Klebsiella pneumoniae, and indwelling medical devices) that infection preventionists could use to target high-risk patients for screening or isolation prior to CP-CRE detection.
Disclosure: None


Do hospitalists who prescribe high (risk-adjusted) rates of antibiotics do so repeatedly?
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s2
-
- Article
-
- You have access
- Open access
- Export citation
-
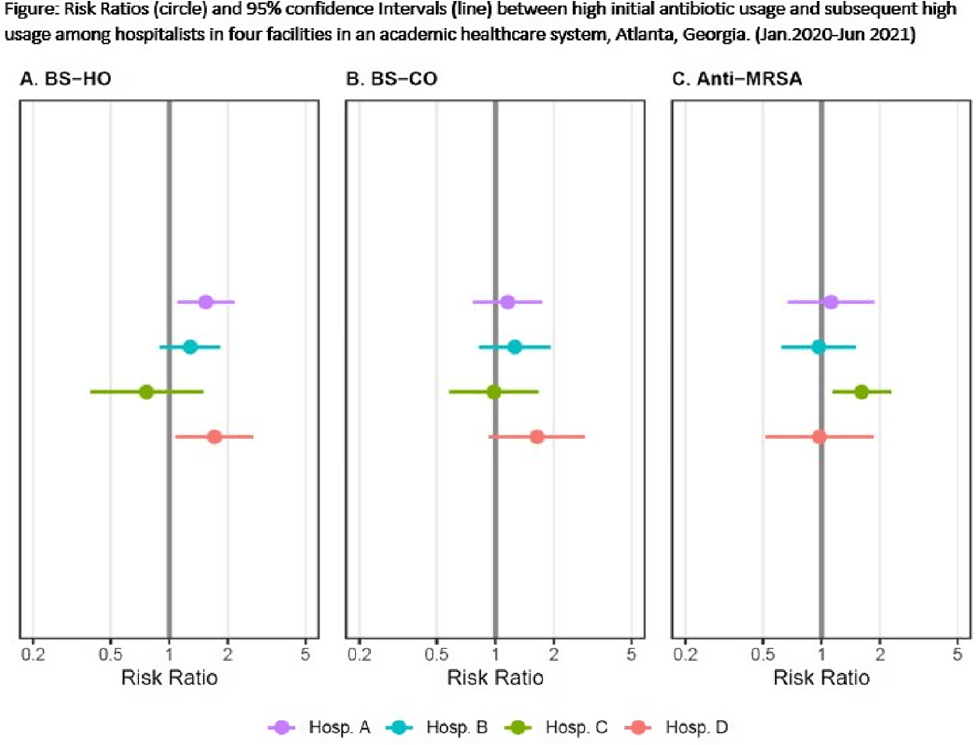
Background: Provider-specific prescribing metrics can be used for benchmarking and feedback to reduce unnecessary antibiotic use; however, metrics must be credible. To improve credibility of a recently described risk-adjusted antibiotic prescribing metric for hospital medicine service (HMS) providers, we assessed whether providers who initially prescribed excess antibiotics continued to prescribe antibiotics excessively. Methods: We linked administration and billing data among patients at 4 acute-care hospitals (1,571 beds) to calculate days of therapy (DOT) ordered by individual hospitalists for each of 3 NHSN antibiotic groupings: broad-spectrum hospital onset (BS-HO), broad-spectrum community-onset (BS-CO), or anti-MRSA for each patient day billed from January 2020 to June 2021. To incorporate repeated measures by provider, mixed models adjusted for patient-mix characteristics (eg, % encounters with urinary tract infection, etc) were used to calculate serial, bimonthly, provider-specific, observed-to-expected ratios (OERs). An OER of 1.25 indicates that the prescribing rate observed was 25% higher than predicted, adjusting for patient mix. We then used log binomial generalized estimating equations to assess whether a high prescribing rate (defined as an OER ≥ 1.25) for an individual provider in an earlier bimonthly period was associated with a persistent high rate for that provider in the following period. Results: Overall, 975 bimonthly periods were evaluated from 136 hospitalists. Most (58%) contributed data the entire 18-month study period. Median OERs were similar between hospitals: 0.94 (IQR, 0.65–1.28) for BS-HO antibiotic use, 0.99 (IQR, 0.73–1.24) for BS-CO antibiotic use, and 0.95 (IQR, 0.65–1.28) for anti-MRSA antibiotic use. At the individual prescriber level, roughly one-quarter of bimonthly OERs (range varied by group and hospital from 21% to 31%) were categorized as high. At 3 of the 4 hospitals, a provider with a high OER for either BS-HO or BS-CO antibiotic use in any bimonthly period was more likely to have a high OER in the subsequent period (Fig. 1). These observed risk ratios were statistically significant for BS-HO antibiotic use at only 2 hospitals: hospital A risk ratio (RR) was 1.54 (95% CI, 1.10–2.16); hospital B RR was 1.28 (95% CI, 0.90–1.82); hospital C RR was 0.76 (95% CI, 0.39–1.48); and ospital D RR was 1.71 (95% CI, 1.09–2.68). Conclusions: Our findings suggest that hospitalists with a higher than expected 2-month period of antibiotic prescribing are likely to continue to have elevated prescribing rates in the following period, particularly for BS-HO antibiotics. These findings increase the credibility of using a 2-month prescribing metric for BS-HO antibiotic stewardship efforts; further work is needed to evaluate utility for other antibiotic groupings.
Funding: None
Disclosures: None

Reductions in inpatient fluoroquinolone use and postdischarge Clostridioides difficile infection (CDI) from a systemwide antimicrobial stewardship intervention
- Part of
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue 1 / 2021
- Published online by Cambridge University Press:
- 22 October 2021, e32
-
- Article
-
- You have access
- Open access
- HTML
- Export citation
Reductions in Postdischarge Clostridioides difficile Infection after an Inpatient Health System Fluoroquinolone Stewardship
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, p. s4
-
- Article
-
- You have access
- Open access
- Export citation
-
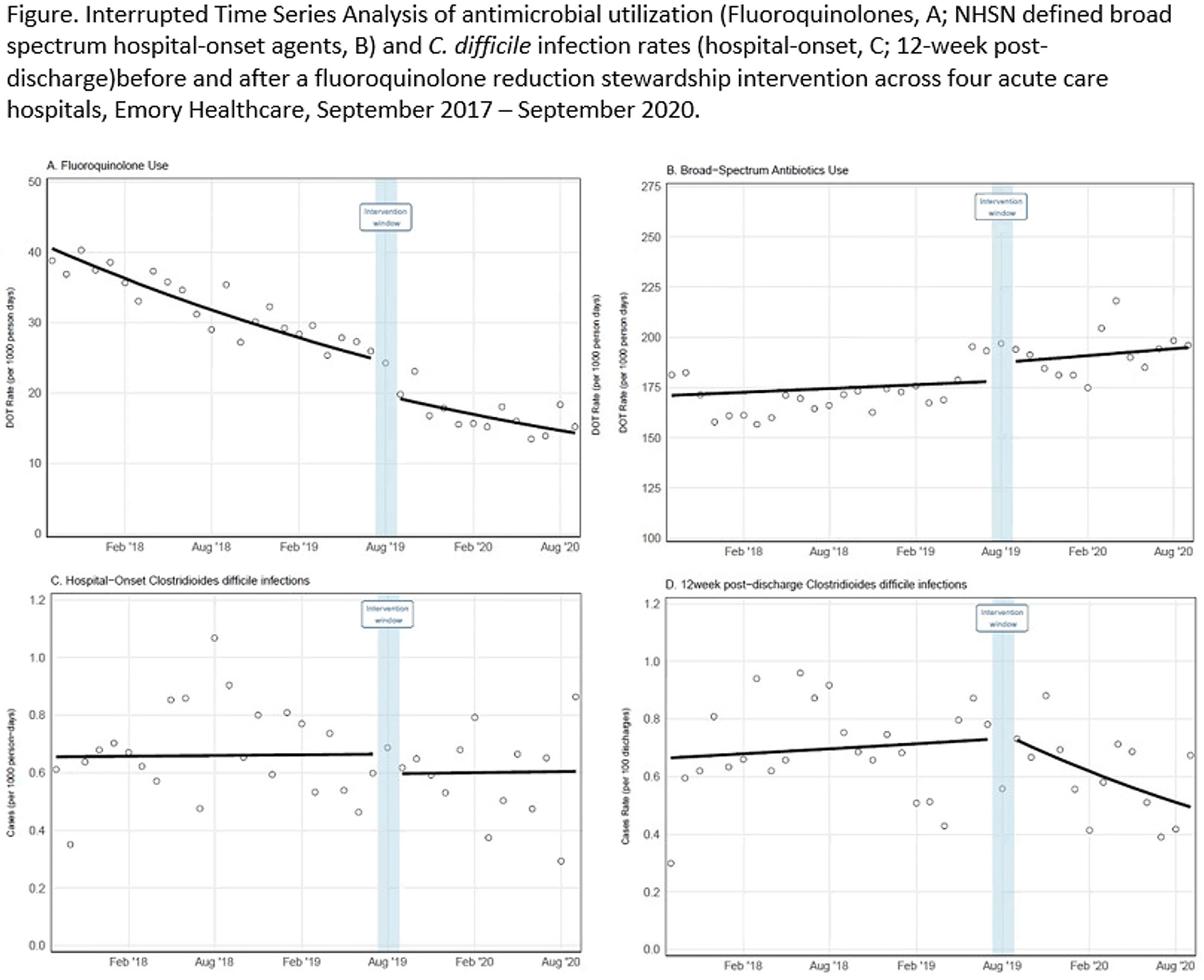
Background: Effective inpatient stewardship initiatives can improve antibiotic prescribing, but impact on outcomes like Clostridioides difficile infections (CDIs) is less apparent. However, the effect of inpatient stewardship efforts may extend to the postdischarge setting. We evaluated whether an intervention targeting inpatient fluoroquinolone (FQ) use in a large healthcare system reduced incidence of postdischarge CDI. Methods: In August 2019, 4 acute-care hospitals in a large healthcare system replaced standalone FQ orders with order sets containing decision support. Order sets redirected prescribers to syndrome order sets that prioritize alternative antibiotics. Monthly patient days (PDs) and antibiotic days of therapy (DOT) administered for FQs and NHSN-defined broad-spectrum hospital-onset (BS-HO) antibiotics were calculated using patient encounter data for the 23 months before and 13 months after the intervention (COVID-19 admissions in the previous 7 months). We evaluated hospital-onset CDI (HO-CDI) per 1,000 PD (defined as any positive test after hospital day 3) and 12-week postdischarge (PDC- CDI) per 100 discharges (any positive test within healthcare system <12 weeks after discharge). Interrupted time-series analysis using generalized estimating equation models with negative binomial link function was conducted; a sensitivity analysis with Medicare case-mix index (CMI) adjustment was also performed to control for differences after start of the COVID-19 pandemic. Results: Among 163,117 admissions, there were 683 HO-CDIs and 1,009 PDC-CDIs. Overall, FQ DOT per 1,000 PD decreased by 21% immediately after the intervention (level change; P < .05) and decreased at a consistent rate throughout the entire study period (−2% per month; P < .01) (Fig. 1). There was a nonsignificant 5% increase in BS-HO antibiotic use immediately after intervention and a continued increase in use after the intervention (0.3% per month; P = .37). HO-CDI rates were stable throughout the study period, with a nonsignificant level change decrease of 10% after the intervention. In contrast, there was a reversal in the trend in PDC-CDI rates from a 0.4% per month increase in the preintervention period to a 3% per month decrease in the postintervention period (P < .01). Sensitivity analysis with adjustment for facility-specific CMI produced similar results but with wider confidence intervals, as did an analysis with a distinct COVID-19 time point. Conclusion: Our systemwide intervention using order sets with decision support reduced inpatient FQ use by 21%. The intervention did not significantly reduce HO-CDI but significantly decreased the incidence of CDI within 12 weeks after discharge. Relying on outcome measures limited to inpatient setting may not reflect the full impact of inpatient stewardship efforts and incorporating postdischarge outcomes, such as CDI, should increasingly be considered.
Funding: No
Disclosures: None
Figure 1.

Carbapenem-resistant Enterobacterales bacteriuria and subsequent bacteremia: A population-based study
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 42 / Issue 8 / August 2021
- Published online by Cambridge University Press:
- 10 December 2020, pp. 962-967
- Print publication:
- August 2021
-
- Article
- Export citation
Variation in Hospitalist-Specific Antibiotic Prescribing at Four Hospitals: A Novel Tool for Antibiotic Stewardship
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s56-s57
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
The impact of an electronic medical record nudge on reducing testing for hospital-onset Clostridioides difficile infection
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue 4 / April 2020
- Published online by Cambridge University Press:
- 10 February 2020, pp. 411-417
- Print publication:
- April 2020
-
- Article
- Export citation
3167 Evaluation of risk factors for progression from carbapenem-resistant Enterobacteriaceae bacteriuria to an invasive infection
-
- Journal:
- Journal of Clinical and Translational Science / Volume 3 / Issue s1 / March 2019
- Published online by Cambridge University Press:
- 26 March 2019, pp. 43-44
-
- Article
-
- You have access
- Open access
- Export citation
