
4 results
Coinfections in hospitalized COVID-19 patients are associated with high mortality: need for improved diagnostic tools
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, pp. s7-s8
-
- Article
-
- You have access
- Open access
- Export citation
-
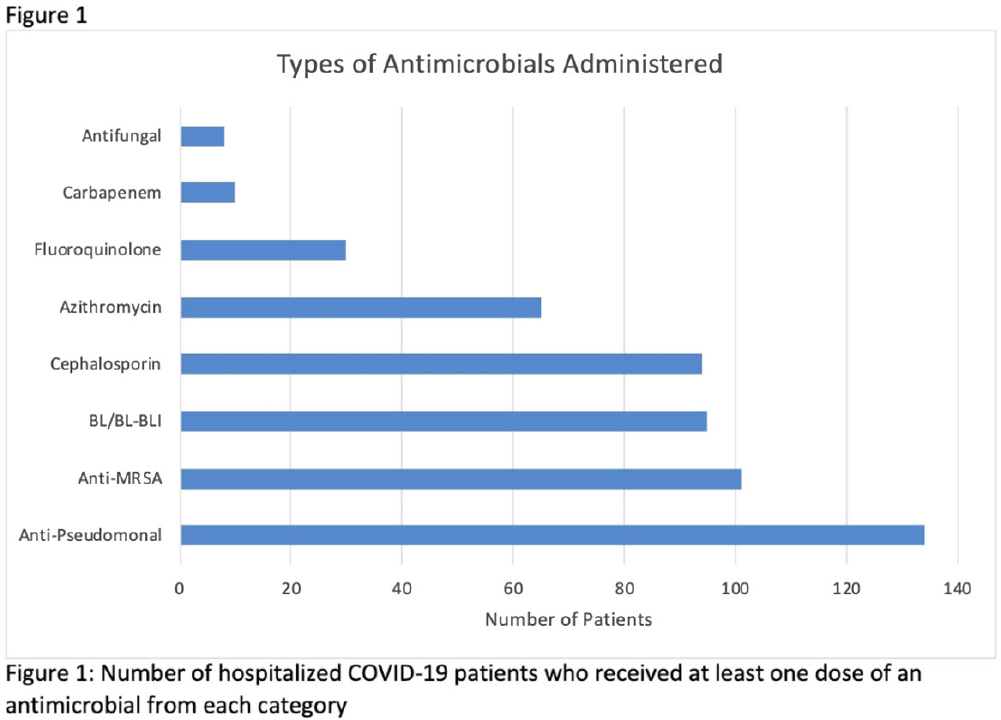
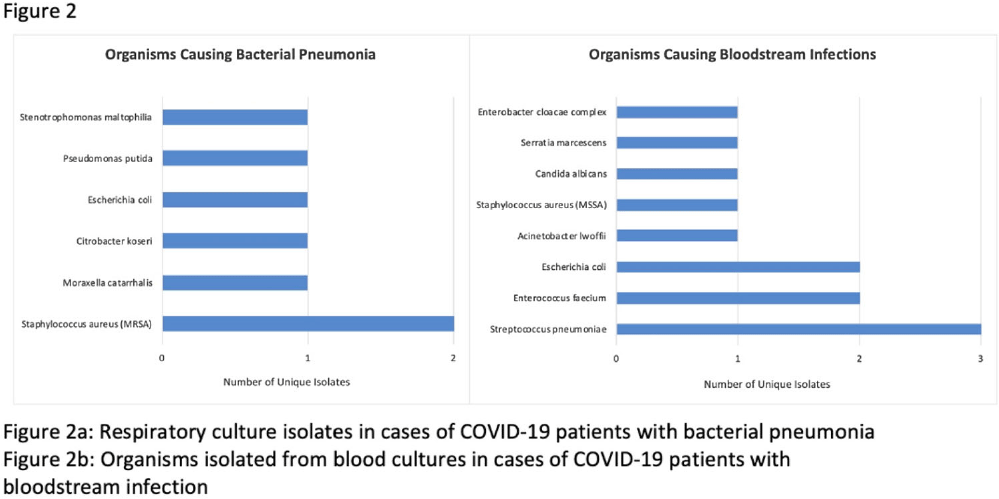
Background: Hospitalized patients with COVID-19 often receive antimicrobial therapies due to concerns for bacterial and fungal coinfections. We analyzed patients admitted with COVID-19 to our VA facility to understand antimicrobial use, frequency of coinfections, and outcomes in our population. Methods: This retrospective study included veterans who were 18 years or older and hospitalized with COVID-19 from March 10, 2020, to March 9, 2021 at the Louis Stokes VA Medical Center in Cleveland, Ohio. We identified antimicrobials administered and coinfections with bacterial or fungal pathogens. Patients were deemed to have coinfection if there was supporting microbiological data and a consistent clinical course upon review of clinical records. Urinary tract infections were excluded because of difficulty determining infection. Odds ratios (ORs) and 95% confidence intervals (CIs) for 30-day mortality were derived using multivariate logistic regression models that included age, Charlson comorbidity index (CCI), corticosteroid use, and time of infection. Results: In our cohort of 312 patients, the median age was 70 years and 97% of the patients were male. The mean CCI was 3.7 (SD, 3.0), and 111 patients (35.6%) had a score ≥5. Oxygen was administered to 250 patients (80.1%), and 20 (6.4%) required mechanical ventilation. Antimicrobials were administered to 164 patients (52.6%) (Fig. 1). Of 20 patients (6.4%) with coinfection, 11 (3.5%) had a bloodstream infection (BSI) and 9 (2.9%) had bacterial pneumonia (Fig. 2). The overall 30-day mortality rate was 12.5% (39 of 312). Among patients with coinfection, the 30-day mortality rate was 45% (9 of 20). Diagnoses of BSI (OR, 6.35; 95% CI, 1.41–26.30) and bacterial pneumonia (OR, 9.34; 95% CI, 2.01–46.34) were associated with increased mortality. Of the data available, 12 (63%) of 19 patients with coinfection had elevated procalcitonin levels (ie, >0.50). At the time of COVID-19 diagnosis, the median absolute lymphocyte count in patients who died was 0.7 K/mm3 (95% CI, 0.6–1.12) in comparison to 1 K/mm3 (95% CI, 0.7–1.4) in patients who survived at 30 days. Conclusions: Our analysis of hospitalized COVID-19 patients with advanced age and underlying comorbid conditions demonstrated that coinfections were infrequent but that they were independently associated with increased mortality. This finding highlights the need for better tools to diagnose the presence or absence of bacterial and fungal coinfection in COVID-19 patients. Our findings also emphasize the need for judicious use of antimicrobials while discerning which patients are at risk of critical illness and mortality.
Funding: None
Disclosures: None


Absence of racial and ethnic disparities in COVID-19 survival among residents of US Veterans’ Affairs community living centers
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 2 / Issue S1 / July 2022
- Published online by Cambridge University Press:
- 16 May 2022, p. s35
-
- Article
-
- You have access
- Open access
- Export citation
-
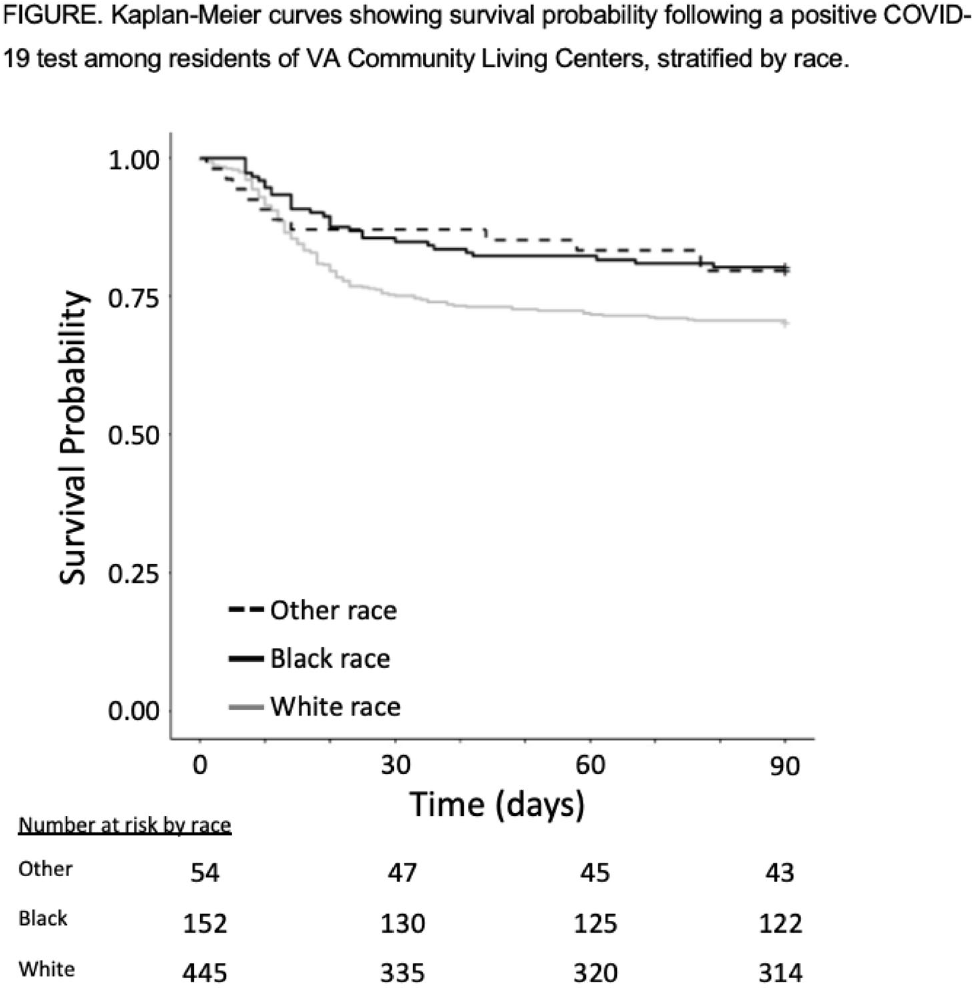
Background: COVID-19 has had a disproportionate effect on nursing homes residents as well as people from racial and ethnic minorities. Whether differences in mortality due to COVID-19 exists for nursing-home residents from racial and ethnic minorities is less clear, with some previous studies reporting systems-level disparities. The Department of Veterans’ Affairs (VA) has nursing homes, termed community living centers (CLCs), across the United States. We hypothesized that differences in COVID-19–related mortality among racial and ethnic minorities would be less pronounced among residents of CLCs. Methods: Using data from the VA Corporate Data Warehouse, we conducted a retrospective cohort study from April 14, 2020 (implementation of population-based testing) to December 10, 2020 (availability of a COVID-19 vaccine). Inclusion criteria were residents with a positive SARS-CoV-2 test while residing in or <48 hours before admission to a CLC. Positive tests <180 days after a prior positive test were excluded. We assessed the cohort for demographics, including self-reported race or ethnicity, clinical characteristics, and survival probability including all-cause 30-day mortality. A multivariable logistic regression model was used to estimate odds ratios (ORs) and 95% confidence intervals (CIs) for all-cause 30-day mortality that included race, ethnicity, age, and Charlson comorbidity index (CCI). Results: Among 14,759 CLC residents, 651 (4.4%) had a positive SARS-COV-2 test. Their mean age was 75.7 ± 11.3 years, and self-reported race or ethnicity was 68% White (445 of 651), 23% Black (152 of 651), and 4% Hispanic/Latinx (27 of 651). The mean CCI was lower among White residents than Black residents (4.15 ± 2.6 vs 4.61 ± 3.1, respectively). All-cause 30-day mortality for CLC residents following positive SARS-COV-2 test was 25% for White patients, 14% for Black patients, and 15% for Hispanic/Latinx patients (Fig. 1). Age (in years), but neither race or ethnicity nor CCI, was independently associated with all-cause 30-day mortality (OR, 1.07; 95% CI, 1.05–1.09) in CLC residents with COVID-19. Conclusions: Among VA CLC residents with a positive COVID-19 test, minority CLC residents did not have worse outcomes than white residents, suggesting that users of the VA healthcare system may enjoy abrogation of some aspects of health disparities.
Funding: None
Disclosures: None

Mortality Among Veterans’ Affairs Community Living Center (CLC) Residents with COVID-19
-
- Journal:
- Antimicrobial Stewardship & Healthcare Epidemiology / Volume 1 / Issue S1 / July 2021
- Published online by Cambridge University Press:
- 29 July 2021, pp. s52-s53
-
- Article
-
- You have access
- Open access
- Export citation
-
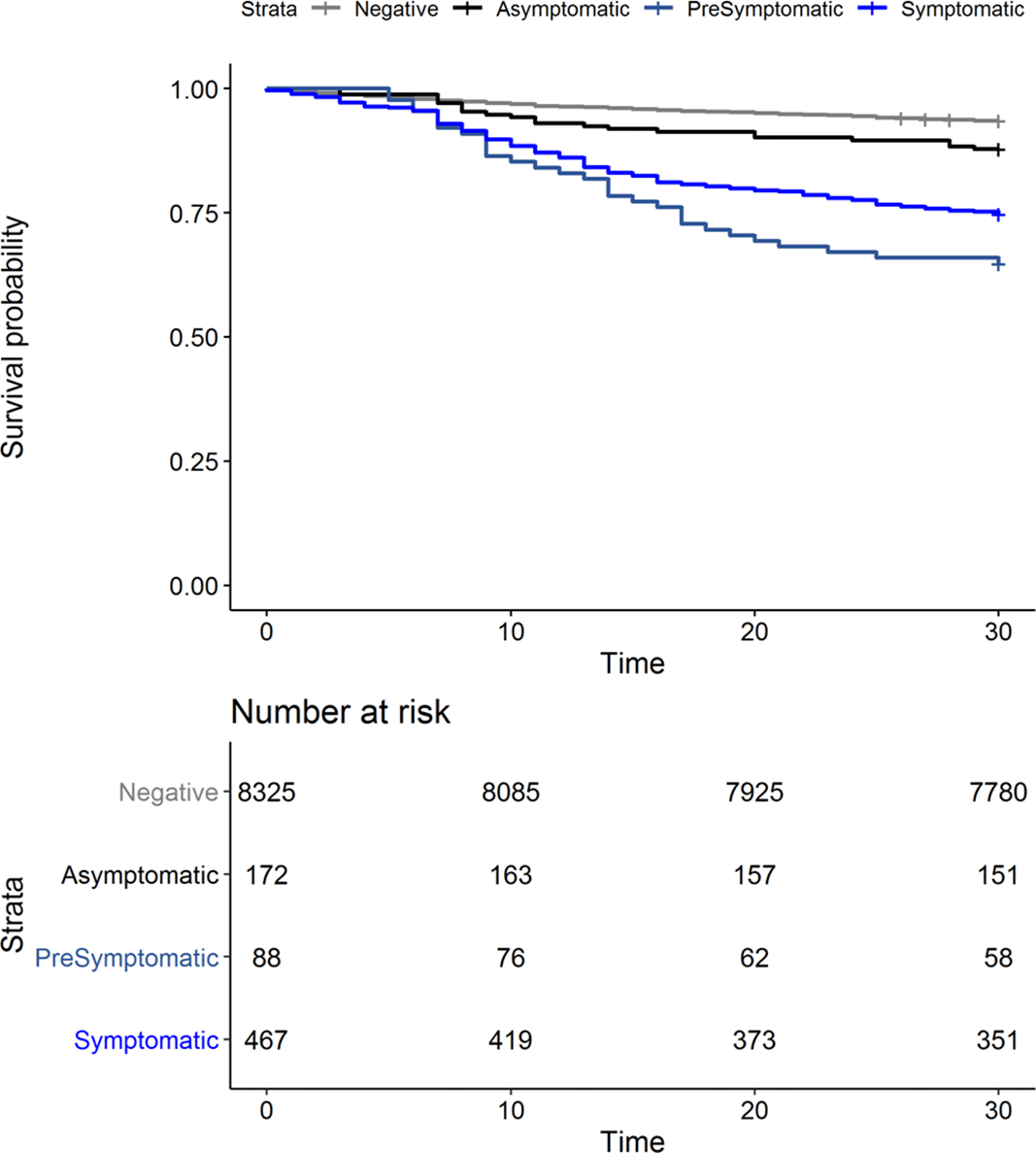
Background: Outcomes among nursing home residents with asymptomatic compared to symptomatic COVID-19 are not well characterized. We assessed all-cause mortality among Veterans’ Affairs (VA) community living center (CLC) residents; we compared those residents with a negative SARS-CoV-2 test to residents with symptomatic, presymptomatic, and asymptomatic SARS-CoV-2 infections. Methods: We conducted a national retrospective cohort study of CLC residents tested for COVID-19 between March 1 and July 31, 2020, based on data compiled through the VA COVID-19 shared data resource. Among those with a positive SARS-CoV-2 test, residents were considered symptomatic if they had experienced COVID-19 symptoms in the 30 days prior to the test. Residents were considered presymptomatic if they did not experience symptoms in the 30 days prior to testing and developed a fever (>38°C) or required supplemental oxygen within 14 and 60 days, respectively, following the test. Residents were considered asymptomatic in the absence of these pre- and posttest symptoms. Results: From March 1 to July 31, 2020, of 9,052 CLC residents screened for COVID-19, 8,325 (92%) tested negative (Table 1). Among 727 residents with positive tests, 467 (64%) were symptomatic, 88 (12%) were presymptomatic, and 172 (24%) remained asymptomatic. We observed significant differences in the racial makeup of these disease groups. Among CLC residents who were symptomatic or presymptomatic, 176 (32%) of 555 were black compared to 39 (23%) of 172 who were asymptomatic and 1,810 (22%) of 8,325 who tested negative for SAR-CoV-2. All-cause 30-day mortality rates for symptomatic and presymptomatic residents were 25% and 34%, respectively, which exceeded the all-cause 30-day mortality of asymptomatic residents (12%) and residents with a negative test (6%) (Figure 1). Conclusions: More than one-third of CLC residents with COVID-19 were asymptomatic at the time of testing. This finding highlights the importance of vigilant infection prevention and control measures. Our finding that mortality among presymptomatic residents exceeded that of symptomatic residents raises consideration for enhancing supportive care measures, such as supplemental oxygen and mitigation of inflammatory reactions, as a means to reduce mortality among nursing home residents with presymptomatic SARS-CoV-2 infections.
Funding: No
Disclosures: None
Table 1. 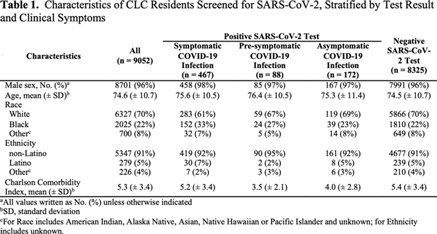
Figure 1.


Appropriateness of C. difficile Testing With Clinical Support Tool Versus Mandatory Infectious Diseases Attending Approval
-
- Journal:
- Infection Control & Hospital Epidemiology / Volume 41 / Issue S1 / October 2020
- Published online by Cambridge University Press:
- 02 November 2020, pp. s126-s127
- Print publication:
- October 2020
-
- Article
-
- You have access
- Export citation
